





The Iconographical Falls Efficacy Scale (Icon-FES) is an innovative tool to assess concern of falling that uses pictures as visual cues to provide more complete environmental contexts. Advantages of Icon-FES over previous scales include the addition of more demanding balance-related activities, ability to assess concern about falling in highly functioning older people, and its normal distribution.
ObjectiveTo perform a cross-cultural adaptation and to assess the measurement properties of the 30-item and 10-item Icon-FES in a community-dwelling Brazilian older population.
MethodsThe cross-cultural adaptation followed the recommendations of international guidelines. We evaluated the measurement properties (i.e. internal consistency, test–retest reproducibility, standard error of the measurement, minimal detectable change, construct validity, ceiling/floor effect, data distribution and discriminative validity), in 100 community-dwelling people aged ≥60 years.
ResultsThe 30-item and 10-item Icon-FES-Brazil showed good internal consistency (alpha and omega >0.70) and excellent intra-rater reproducibility (ICC2,1=0.96 and 0.93, respectively). According to the standard error of the measurement and minimal detectable change, the magnitude of change needed to exceed the measurement error and variability were 7.2 and 3.4 points for the 30-item and 10-item Icon-FES, respectively. We observed an excellent correlation between both versions of the Icon-FES and Falls Efficacy Scale – International (rho=0.83, p<0.001 [30-item version]; 0.76, p<0.001 [10-item version]). Icon-FES versions showed normal distribution, no floor/ceiling effects and were able to discriminate between groups relating to fall risk factors.
ConclusionIcon-FES-Brazil is a semantically and linguistically appropriate tool with acceptable measurement properties to evaluate concern about falling among the community-dwelling older population.
Improved health and longevity have accelerated the pace of population aging around the world.1 Global population estimates from 2013 show that 841 million people are aged 60 years or over, and demographic projections show that this number can reach 2 billion by 2050.2 In Brazil, the population growth follows a similar trend. People aged 60 years or over represented 10% (19.6 million) of the Brazilian population in 2010 and it is expected to reach 29.4% (66 million) in 2050.3 Falls represent one of the major problems among the older population.4 Around 30% of people aged 65 years or older fall each year, and often suffer fall-related injuries, long-term disability, loss of independence, hospitalization and death.5–8 On an individual level, falls often result in a concern about falling.9,10 Concern about falling in older people can present itself as a persistent feeling of concern about the risk of falling during one or more activities of daily living, with a negative impact on quality of life. Adaptive behaviors, such as avoidance of concern-related activities or being overly cautious, can lead to a decline in physical and functional performance, and social isolation.11–13
Over time, a number of scales have been developed to assess concern about falling. The Falls Efficacy Scale – International (FES-I) is considered the gold standard with excellent measurement properties across a range of settings and cultures.14 However, the FES-I is skewed toward assessing people with lower levels of concern about falling,15 and does not specify detailed contextual elements. To address the limitations of the FES-I, a group of Australian researchers developed the Iconographical Falls Efficacy Scale (Icon-FES), a scale that assesses concern about falling in an innovative way, including many different activities and using pictures to provide clear and unambiguous contexts.15 The use of images may increase the understanding of the situational context of the older person and therefore make the evaluation process more reliable. Previous studies have demonstrated that the Icon-FES and FES-I are measuring related constructs. Both measures have excellent measurement properties, with the main advantage of the Icon-FES being its normal distribution in healthy older adults.16
The Icon-FES has not been cross-culturally adapted for the Brazilian population. A rigorous cross-cultural validation is particularly important for a contextual scale such as the Icon-FES to ensure that the situational contexts apply to the cultural setting where it is used.17 The main objective of this study was to translate and cross-culturally adapt the Icon-FES, both 30-item and 10-item versions, into Brazilian-Portuguese and to investigate their measurement properties (i.e., internal consistency, test–retest reproducibility, standard error of the measurement, minimal detectable change, construct validity, ceiling and floor effect, data distribution and discriminative validity). As a secondary aim, we compared the performance of the FES-I on specific measurement properties (i.e. ceiling and floor effect, data distribution and discriminative validity) to both versions of the Icon-FES.
MethodsStudy designThis is a cross-sectional study that follows the recommended taxonomy and definition from the COnsensus-based Standards for the selection of health Measurement IMstruments (COSMIN).17 The present study was approved by the Human Ethics Committee of the Universidade Estadual Paulista (UNESP), Presidente Prudente, SP, Brazil (CAAE 54578215.8.0000.5402).
ParticipantsA total of 100 people aged ≥60 years participated in this study. Participants were recruited via advertisements in health centers and community organizations in the urban area of Presidente Prudente. Eligible participants were community-dwelling, without cognitive deficits as determined with Mini-Mental State Examination (i.e., 18 points for people with low and medium schooling, and 26 points for those with University degree),18 and agreed to sign the informed consent form. Exclusion criteria were neurological, cardiovascular or major musculoskeletal impairments that precluded participants from completing physical assessments. The sample size for the present study was based on COSMIN benchmarks.19 According to COSMIN, studies assessing internal consistency, reliability and construct validity should include more than 100 participants to be judged as having excellent methodology. Therefore, our sample size was based on COSMIN benchmarks to be considered a study with at least excellent methodological quality (i.e. more than 100 participants).
Icon-FES measureThe Icon-FES provides information on level of concern about falling through a combination of illustrating activities of daily living and matching short phrases. There are two version of the Icon-FES available, the long version with 30 items and the short version with 10 items. For each item, the study participants were requested to “look at each picture carefully, and try to imagine performing the activity using their normal walking aid”. The level of concern about falling when performing each activity is scored on a 4-point scale (1=not at all concerned to 4=very concerned). The total score for the 30-item Icon-FES ranges from 30 to 120 and the 10-item Icon-FES ranges from 10 to 40.
Translation proceduresThe cross-cultural adaptation of the Icon-FES was divided into 5 phases (i.e., initial translation, synthesis of translation, back-translation, consensus version, evaluation and testing phase), following a previously published standard protocol.20,21 In the ‘initial translation’ phase, two Brazilian bilingual physiotherapists translated the scale into Brazilian-Portuguese. In the ‘synthesis of translation’ phase, the translators and two other researchers prepared a single consensus of the translated scale. In the ‘back-translation’ phase, two native English speakers who had no previous contact with the original version of the scale independently translated the consensus Brazilian-Portuguese version back into English. In the ‘consensus version and evaluation’ phase, a committee of experts consisting of two Brazilian bilingual translators, one physical therapist with 8 years of clinical experience in geriatric rehabilitation, one Brazilian researcher (DS) with experience in administering the English version of the Icon-FES and one university lecturer (RZP) experienced with the process of cultural adaptation, analyzed all reports and developed the prefinal version of the questionnaire. The committee of experts was in close contact with the original developers of the Icon-FES during the whole process. The members of the committee checked all items independently for equivalence with the original questionnaire. In case of disagreement by one member, the committee reached a consensus. For the ‘testing phase’ (pilot study), the culturally adapted Icon-FES-Brazil questionnaire was administered in 30 older people meeting the eligibility criteria for this study to check if participants were able to understand the questionnaire without difficulty. The items not understood by at least 20% of the participants in the pilot study would need to be reformulated. The same approach has been adopted in previous studies.22,23
Assessment proceduresAfter the cross-cultural adaptation process, we evaluated the measurement properties of the Icon-FES-Brazil questionnaires, a process that included two face-to-face interviews. In the first interview, we collected data on demographic characteristics (e.g. age, gender, educational level) and history of falls since the age of 60 years. The Mini-Mental State Examination18 was used to assess cognitive status. Standing balance was assessed as the time in second to stand on one leg with eyes open.24 Participants were given two attempts and the best time was recorded. Mobility was assessed using the timed chair stand and gait speed tests from the Short Physical Performance Battery.25 The time to complete five repetitions of the sit-to-stand test and to walk 4 meters at a comfortable pace were recorded in seconds for the chair stand and gait speed tests. Participants were also asked to complete the FES-I-Brazil (16-item) and the 30-item Icon-FES-Brazil questionnaires to assess concern about falling on a 4-point scale (1=not at all concerned to 4=very concerned). The total score for the 10-item Icon-FES-Brazil was calculated using the scores from the corresponding items in the 30-item version (i.e. item 2, 4, 5, 6, 9, 10, 15, 16, 24 and 25). Total score of 10-item icon-FES, 16-item FES-I, and 30-item icon-FES ranges from 10, 16 and 30 (no concern about falling) to 40, 64 and 120 (severe concern about falling) points, respectively.14,15,26 In the second interview, seven days after the initial interview, participants were reassessed on the Icon-FES-Brazil questionnaires for assessment of reproducibility.
Statistical analysesDescriptive analyses were conducted for the total sample. Normal and non-normal distributed data was expressed as mean and standard deviation (SD) or median and interquartile range (IQR), respectively. For categorical and dichotomous variables, frequency and proportion were calculated. Measurement properties of the 30-item and 10-item version of the Icon-FES-Brazil questionnaires were evaluated on both reliability and validity measures. All analyses were performed using SPSS for Windows Version 20.0 (IBM Corporation, Somers, New York, USA), except for omega coefficient in which the R software27 was used following the instructions published elsewhere.28
Reliability and measurement property analysesInternal consistency was assessed using the Cronbach's alpha and the omega to determine how well the items on each subscale measured the same construct – the coefficients were considered adequate if greater than 0.70.29Test–retest reproducibility was assessed using the type 2,1 intraclass correlation coefficient (ICC2,1) to measure reproducibility – results were interpreted as poor (lower than 0.40), good (from 0.40 to 0.75) or excellent (above 0.75) reproducibility.30Standard error of the measurement (SEM) and minimal detectable change (MDC) were calculated to reflect the variability associated with individual scores in the questionnaire and the magnitude of change that a measurement must demonstrate to exceed the anticipated measurement error and variability, respectively. The formulas used for calculating the SEM and MDC were SEM=SD √1-ICC and MDC=1.96 √2 SEM.31Ceiling and floor effects were established by calculating the percentage of respondents who answered the maximum score (ceiling effect) and the minimum scores (floor effect). Ceiling and floor effects were defined as when more than 15% of the respondents answer the maximum and/or minimum score, respectively.32Distribution of the data. Skewness and kurtosis tests were used to assess normality. For the skewness and kurtosis tests, values between −1 and +1 indicate that the distribution is within the limits of normal distribution. Given that one advantage of the Icon-FES over the FES-I is its normal distribution, we analyzed the ceiling and floor effects and the data distribution of the FES-I for comparison purposes.
Validity analysesConstruct validity was assessed using the Spearman's correlation (rho) coefficient to determine the correlation between FES-I and Icon-FES-Brazil. The magnitude of association was interpreted as no relationship (from 0.00 to 0.25), fair relationship (from 0.25 to 0.50), moderate to good relationship (from 0.50 to 0.75), and good to excellent relationship (above 0.75).30 Given that both instruments assess concerns about falling, we hypothesized at least a moderate relationship between both measures. The other aspect investigated was the discriminative validity. Discriminative validity of the 30-item Icon-FES, 10-item Icon-FES and FES-I was assessed using independent t-test or Mann–Whitney U test, depending on the distribution of the data, to examine between-group differences in total scores according to age, gender, education levels, history of falls, balance, mobility and cognitive measures. These variables were chosen because they have previously been associated with falls and concern about falling.33–36 We hypothesized that females, older participants, participants with history of falls, poor mobility and cognitive deficits would show higher levels of concern about falling. With regards to education levels, we hypothesized that, because the Icon-FES uses pictures, no difference in the levels of concern about falling would be found between groups with different education levels. For the discriminative validity analyses, continuous variables (i.e. age, balance, mobility and cognitive measures) were dichotomized using their median values. For education levels, given that the use of pictures in the Icon-FES may facilitate the assessment of those with a lower education level we compared the ‘incomplete primary school’ group with the remaining groups (i.e. ‘complete primary school or above’). Effect sizes for between-group comparisons were compared by normalizing both scales (by dividing the total score by the number of item), and then by subtracting the mean in the first group from that in the second group and dividing the result by the pooled standard deviation.14,16
ResultsTable 1 shows the cross-cultural adaptation process used to develop the final Brazilian-Portuguese version of the Icon-FES-Brazil questionnaire. During this process, the committee of experts decided to replace the activity in item 25 of the 30-item Icon-FES, ‘cleaning the gutter’, by another activity ‘changing the bulb’ considered to be more familiar but with the same level of difficulty for the Brazilian population. In addition, the accompanying phrase in item 30 of the 30-item Icon-FES, ‘crossing the street against the lights’ (Portuguese translation: ‘atravessar a rua quando o sinal está fechado’), was modified to enhance clarity to ‘crossing the street when the lights are closed to pedestrians’ (Portuguese translation: ‘atravessar a rua quando o sinal está fechado para pedestres’). There were no changes to other items apart from those related to the translation process. The sample recruited in the pilot study (n=30) had a mean age of 67.4 (SD 5.6, range 61–82) years, 30% (n=9) of the participants completed higher education and the majority (n=27) were female. Participants reported no difficulties with the cross-cultural adapted items. The cross-culturally adapted 30-item and 10-item versions of the Icon-FES-Brazil are available on the following link https://www.neura.edu.au/apps/iconfes/instructions/.
Original version, consensus Brazilian-Portuguese version, back translations and final Brazilian-Portuguese version of the Icon-FES instructions, items and 4-point scale.
| Original version | Translations | Consensus Brazilian-Portuguese version | Back translations | Final Brazilian-Portuguese version |
|---|---|---|---|---|
| Icon-FES instructions | ||||
| 1. Please look at each picture carefully, and try to imagine yourself performing the activity. | T1: Olhe cada desenho com bastante atenção, e tente imaginar o(a) senhor(a) mesmo(a) fazendo cada atividade. T2: Por favor olhe para cada desenho com bastante atenção e tente imaginar o(a) senhor(a) fazendo cada atividade. | Olhe cada desenho com bastante atenção, e tente imaginar o(a) senhor(a) mesmo(a) fazendo cada atividade. | T1: Look at each drawing with a lot of attention, and try to imagine you doing each activity. T2: Look at each drawing carefully and try to imagine yourself doing each activity. | Olhe cada desenho com bastante atenção, e tente imaginar o(a) senhor(a) mesmo(a) fazendo cada atividade. |
| 2. If you currently don’t do the activity (e.g. If someone does your shopping for you), please answer to indicate whether you think you would be concerned about falling IF you did the activity. | T1: Se o(a) senhor(a) atualmente não realiza a atividade (por exemplo, alguém lhe ajuda a fazer as compras de mercado), por favor responda da forma que o(a) senhor(a) se sentiria SE estivesse realizando a atividade. T2: Se o(a) senhor(a) atualmente não realiza a atividade (por exemplo, alguém faz suas compras de mercado), por favor indique se estaria preocupado com a possibilidade de cair. | Se o(a) senhor(a) atualmente não realiza a atividade (por exemplo, alguém lhe ajuda a fazer as compras de mercado), por favor responda da forma que o(a) senhor(a) se sentiria SE estivesse realizando a atividade. | T1: If you actually don’t do these activities (for example, somebody else helps you to do the shopping), please answer the way you would feel IF you could do the activity. T2: If nowadays you don’t do the activity (for exmple, someone helps you shop at the market), please answer as how you would feel IF you were doing it. | Se o(a) senhor(a) atualmente não realiza a atividade (por exemplo, alguém lhe ajuda a fazer as compras de mercado), por favor responda da forma que o(a) senhor(a) se sentiria SE estivesse realizando a atividade. |
| 3. Imagine that you are using your normal walking aid. | T1: Imagine que o(a) senhor(a) está usando o seu andador normal. T2: Imagine-se usando o seu andador normal. | Imagine que o(a) senhor(a) está usando o seu andador normal. | T1: Imagine yourself using your regular walker. T2: Imagine you are using your normal walker. | Imagine que o(a) senhor(a) está usando o seu andador normal. |
| 4. We would like to know how concerned you are about the possibility of galling while doing any of the following activities, as pictured on the drawings. | T1: Nós gostaríamos de saber qual seria o seu medo de cair enquanto estivesse fazendo quaisquer das atividades que estão sendo mostradas nos desenhos. T2: Nós gostaríamos de saber o quão preocupado(a) o(a) senhor(a) estaria com a possibilidade de cair enquanto realiza alguma das atividades mostradas nas figuras. | Nós gostaríamos de saber qual seria o seu medo de cair enquanto estivesse fazendo quaisquer das atividades que estão sendo mostradas nos desenhos. | T1: We would like to know which fear of falling would you have while doing any of these activities that are being showed by the drawings. T2: We would like to know what would be your fear of falling down if you were doing any of these activities that are shown in the drawings. | Nós gostaríamos de saber qual seria o seu medo de cair enquanto estivesse fazendo quaisquer das atividades que estão sendo mostradas nos desenhos. |
| 5. For each of the following activities, please show the level of concern which is closest to your own opinion to show how concerned you are that you might fall if you did this activity. | T1: Em cada uma das atividades seguintes, por favor mostre qual é o nível do receio que o(a) senhor(a) tem. T2: Em cada uma das atividades seguintes, por favor mostre qual é o nível do receio que o(a) senhor(a) tem de acordo com a escala seguinte. | Em cada uma das atividades seguintes, por favor mostre qual é o nível do receio que o(a) senhor(a) de acordo com a escala seguinte (mostre a escala). | T1: In any of these activities ahead, please show us the level of fright in which you would feel following the scale ahead (show him/her the scale). T2: For each of these following activities, please show what your level of fear would be according to this scale. | Em cada uma das atividades seguintes, por favor mostre qual é o nível do receio que o(a) senhor(a) tem. |
| Icon-FES items | ||||
| 1. Cleaning the house. | T1: Limpando a casa (ex: passar pano, aspirar ou tirar a poeira). T2: Limpando a casa (ex: passar pano, aspirar ou tirar a poeira). | Limpando a casa. | T1: Cleaning the house. T2: Cleaning the house. | Limpando a casa. |
| 2. Getting dressed.a | T1: Vestindo ou tirando a roupa. T2: Vestindo ou tirando a roupa. | Vestindo ou tirando a roupa. | T1: Putting on or taking off clothes. T2: Wearing or removing of clothes. | Vestindo ou tirando a roupa. |
| 3. Preparing a simple meal. | T1: Preparando refeições simples. T2: Preparando refeições simples. | Preparando refeições simples. | T1: Preparing simple meals T2: Preparing simple meals | Preparando refeições simples. |
| 4. Taking a bath.a | T1: Tomando banho de banheira. T2: Tomando banho de banheira. | Tomando banho de banheira | T1: Taking a bath T2: Taking a bath | Tomando banho de banheira. |
| 5. Taking a showera | T1: Tomando banho. T2: Tomando banho. | Tomando banho. | T1: Taking a shower. T2: Taking a shower. | Tomando banho. |
| 6. Going to the shop.a | T1: Indo às compras. T2: Indo às compras. | Indo ás compras. | T1: Do the shopping. T2: Going shopping. | Indo ás compras. |
| 7. Getting out of a chair. | T1: Sentando ou levantando de uma cadeira. T2: Sentando ou levantando de uma cadeira. | Sentando ou levantando de uma cadeira. | T1: Sitting on or standing up from a chair. T2: Sitting or standing up. | Sentando ou levantando de uma cadeira. |
| 8. Going up the stairs. | T1: Subindo ou descendo escadas. T2: Subindo escadas. | Subindo escadas. | T1: Going up stairs T2: Climbing stairs | Subindo escadas. |
| 9. Going down the stairs.a | T1: Subindo ou descendo escadas. T2: Descendo escadas. | Descendo escadas. | T1: Going down stairs. T2: Descend stairs. | Descendo escadas. |
| 10. Walking around in the neighborhood.a | T1: Caminhando pela vizinhança. T2: Caminhando pela vizinhança. | Caminhando pela vizinhança. | T1: Walking by the neighborhood. T2: Hiking through the neighborhood. | Caminhando pela vizinhança. |
| 11. Walking around in the neighborhood in rainy weather. | T1: Andando pela vizinhança num dia de chuva. T2: Andando pela vizinhança em um dia de chuva. | Andando pela vizinhança em um dia de chuva. | T1: Walking by the neighborhood in a rainy day. T2: Walking by the neighborhood on a rainy day. | Andando pela vizinhança em um dia de chuva. |
| 12. Walking around in the neighborhood in windy weather. | T1: Andando pela vizinhança num dia de muito vento. T2: Andando pela vizinhança em um dia de muito vento. | Andando pela vizinhança em um dia de muito vento. | T1: Walking by the neighborhood in a really windy day. T2: Walking by the neighborhood on a very windy day. | Andando pela vizinhança em um dia de muito vento. |
| 13. Walking around in the neighborhood in the dark. | T1: Andando pela vizinhança após escurecer. T2: Andando pela vizinhança após escurecer. | Andando pela vizinhança após escurecer. | T1: Walking by the neighborhood while sunset darkening. T2: Walking by the neighborhood after dark. | Andando pela vizinhança após escurecer. |
| 14. Reaching for something above your head (ground). | T1: Pegando algo acima de sua cabeça. T2: Na ponta dos pés para alcançar algo que está acima da sua cabeça. | Na ponta dos pés para alcançar algo que está acima de sua cabeça. | T1: On the top of your toes to reach something above your head. T2: Standing on tiptoe to reach for something over your head. | Na ponta dos pés para alcançar algo que está acima de sua cabeça. |
| 15. Reaching for something above your head (safe step).a | T1: Pegando algo acima de sua cabeça. T2: Utilizando uma escada para alcançar algo que está acima da sua cabeça. | Utilizando uma escada para pegar algo que está acima de sua cabeça. | T1: Using stairs to fetch something above your head. T2: Using a ladder to reach for something over your head. | Utilizando uma escada para pegar algo que está acima de sua cabeça. |
| 16. Reaching for something above your head (chair).a | T1: Pegando algo acima de sua cabeça. T2: Utilizando uma cadeira para alcançar algo que está acima da sua cabeça. | Utilizando uma cadeira para pegar algo que está acima de sua cabeça. | T1: Using a chair to fetch something above your head. T2: Using a chair to reach for something over your head. | Utilizando uma cadeira para pegar algo que está acima de sua cabeça. |
| 17. Reaching for something on the ground. | T1: Pegando algo do chão. T2: Pegando algo do chão. | Pegando algo do chão. | T1: Catching something from the floor. T2: Reaching for something on the floor. | Pegando algo do chão. |
| 18. Going to answer the telephone before it stops ringing. | T1: Ir atender o telefone antes que pare de tocar. T2: Ir atender o telefone antes que pare de tocar. | Ir atender o telefone antes que pare de tocar. | T1: Go answer the phone before it stops ringing. T2: Answering the phone before it stops ringing. | Ir atender o telefone antes que pare de tocar. |
| 19. Walking on a slippery surface. | T1: Andando sobre superfície escorregadia (ex: chão molhado). T2: Andando sobre superfície escorregadia (ex: chão molhado). | Andando sobre superfície escorregadia. | T1: Walking by a slippery surface. T2: Walking on a slippery surface. | Andando sobre superfície escorregadia. |
| 20. Visiting a friend or relative. | T1: Visitando um amigo ou parente. T2: Visitando um amigo ou parente. | Visitando um amigo ou parente. | T1: Visiting a friend or a relative. T2: Visiting a friend or a relative. | Visitando um amigo ou parente. |
| 21. Walking in a place with crowds | T1: Andando em lugares cheios de gente. T2: Andando em lugares cheios de gente. | Andando em lugares cheio de gente. | T1: Walking by crowded places T2: Walking on crowded places | Andando em lugares cheio de gente. |
| 22. Walking on an uneven surface. | T1: Caminhando sobre superfície irregular (com pedras, ou esburacada). T2: Caminhando sobre superfície irregular (com pedras, ou esburacada). | Caminhando sobre superfície irregular. | T1: Walking by irregular surfaces T2: Walking on an irregular surface | Caminhando sobre superfície irregular. |
| 23. Walking down a slope. | T1: Subindo ou descendo uma ladeira. T2: Subindo ou descendo uma ladeira. | Subindo ou descendo uma ladeira. | T1: Going up or down a hill. T2: Climbing or descending a ladder. | Subindo ou descendo uma ladeira. |
| 24. Going out to a social event.a | T1: Indo a uma atividade social (ex: igreja, reunião de família ou encontro no clube). T2: Indo a uma atividade social (ex: igreja, reunião de família ou encontro no clube). | Indo a eventos sociais. | T1: Going to social events. T2: Going to social events. | Indo a eventos sociais. |
| 25. Changing the light bulb.a | T1: Trocando uma lâmpada. T2: Trocando uma lâmpada. | Trocando a lâmpada. | T1: Changing the light bulb. T2: Changing the light bulb. | Trocando a lâmpada. |
| 26. Taking the escalator. | T1: Subindo de escada rolante. T2: Subindo de escada rolante. | Subindo de escada rolante. | T1: Using the escalator. T2: Getting on an escalator. | Subindo de escada rolante. |
| 27. Running to catch the bus. | T1: Correndo para pegar o ônibus. T2: Correndo para pegar o ônibus. | Correndo para pegar o ônibus. | T1: Running to get in a bus. T2: Running to catch the bus. | Correndo para pegar o ônibus. |
| 28. Crossing the street. | T1: Atravessando a rua. T2: Atravessando a rua. | Atravessando a rua. | T1: Crossing the street. T2: Crossing the street. | Atravessando a rua. |
| 29. Crossing a busy street | T1: Atravessando uma rua muito movimentada. T2: Atravessando uma rua muito movimentada | Atravessando uma rua muito movimentada. | T1: Crossing a busy street. T2: Crossing a busy street. | Atravessando uma rua muito movimentada. |
| 30. Crossing the street against the lights. | T1: Atravessando a rua quando o sinal está fechado. T2: Atravessando a rua quando o sinal está fechado. | Atravessando a rua quando o sinal está fechado. | T1: Crossing the street while the red light sign. T2: Crossing the street while the lights are red. | Atravessando a rua quando o sinal está fechado para pedestre. |
| Icon-FES 4-point scale | ||||
| 1. Not at all concerned | T1: Nem um pouco preocupado T2: Nem um pouco preocupado(a) | Nem um pouco preocupado | T1: Not even a little bit worried T2: Not worried at all | Nem um pouco preocupado |
| 2. Somewhat concerned | T1: Um pouco preocupado T2: Um pouco preocupado(a) | Um pouco preocupado | T1: A little worried T2: A little worried | Um pouco preocupado |
| 3. Fairly concerned | T1: Muito preocupado T2: Muito preocupado(a) | Muito preocupado | T1: A lot worried T2: Very worried | Muito preocupado |
| 4. Very concerned | T1: Extremamente preocupado T2: Extremamente preocupado(a) | Extremamente preocupado | T1: Extremely worried T2: Extremely worried | Extremamente preocupado |
T1, first translator; T2, second translator.
To evaluate the measurement properties of the questionnaire, one hundred older people were recruited between August 2016 and May 2017. The mean age of participants was 71.4 (SD 7.3, range 60 to 90) years, and the majority was female (n=82, 82%). Complete demographic and clinical data are summarized in Table 2.
Participants’ characteristics.
| Total sample (n=100) | |
|---|---|
| Age, years | 71.4±7.3 |
| Sex | |
| Female | 82 (82%) |
| Male | 18 (18%) |
| BMI, kg/m2 | 26.4 (4.8) |
| Educational levela | |
| Incomplete primary school | 27 (27%) |
| Complete primary school | 10 (10%) |
| Incomplete secondary school | 6 (6%) |
| Complete secondary school | 14(14%) |
| Incomplete higher education | 3 (3%) |
| Complete higher education | 40 (40%) |
| Falls since 60 years, n (%) | |
| Yes | 56 (56%) |
| No | 44 (44%) |
| Falls in the last 12 months, n (%) | |
| Yes | 15 (15%) |
| No | 85 (85%) |
| MMSE, score | 27 [26–29] |
| Balance eyes open, seconds | 6.7 [3.3–11.6] |
| 4-meter walking test, seconds | 5.3±1.4 |
| Sit-to-stand test, seconds | 15.5±4.1 |
| FES-I | 22.5 [20.0–27.0] |
Values are mean±standard deviation, median [interquartile range] or frequency (proportion).
Abbreviations: BMI, body mass index; MEEM, Mini-Mental State Examination; FES-I, Falls Efficacy Scale.
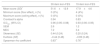
Table 3 shows the measurement properties of the 30-item and 10-item Icon-FES questionnaires. The internal consistency was considered adequate for the 30-item and 10-item Icon-FES. The intra-rater reproducibility was considered excellent with an intraclass correlation coefficient of higher than 0.70 for both Icon-FES versions. SEM and MDC values showed that the variability associated with individual scores was small (i.e. 2% and 3% of the total score for the 30-item and 10-item versions, respectively) and the magnitude of the change needed to exceed the anticipated measurement error and variability of the Icon-FES questionnaires was 7.2 points for 30-item version and 3.4 points for the 10-item version. The correlation between the Icon-FES and FES-I questionnaires was acceptable (rho=0.83, p<0.001), demonstrating that both instruments are measuring similar constructs in relation to concern about falling. No ceiling or floor effects were identified for the Icon-FES questionnaires. According to the data distribution, both versions of the Icon-FES questionnaires were within the normal limits of normal distribution. In addition, FES-I did not show ceiling and floor effect (minimum score=2% [n=2] and maximum score=0% [n=0]) but FES-I score were slightly skewed (Skewness=1.02 [standard error=0.24]; Kurtosis=0.50, [standard error=0.48]).
Descriptive analyses, internal consistency analysis, test–retest reliability, standard error of the measure, minimal detectable change and construct validity of the 30-item and 10-item Icon-FES questionnaire.
| 30-item Icon-FES | 10-item Icon-FES | |
|---|---|---|
| Mean score (SD)* | 51.6±12.9 | 17.9±4.6 |
| Minimum score (floor effect), n (%) | 0 (0%) | 4 (4%) |
| Maximum score (ceiling effect), n (%) | 0 (0%) | 0 (0%) |
| Cronbach's alpha | 0.94 | 0.83 |
| ICC2,1 (95% CI) | 0.96 (0.95–0.98) | 0.93 (0.90–0.95) |
| SEM | 2.6 | 1.2 |
| MDC | 7.2 | 3.4 |
| Skewness (SE) | 0.44 (0.24) | 0.20 (0.24) |
| Kurtosis (SE) | −0.44 (0.48) | −0.69 (0.48) |
| Spearman rho coefficient | 0.83** | 0.76** |
Abbreviations: ICC, intraclass correlation coefficient; IC, confidence interval; SEM, standard error of the measurement; SE, standard error; SD, standard deviation; MDC, minimal detectable change.
The discriminative validity analysis revealed significantly higher Icon-FES scores for both versions for participants who experienced any falls since the age of 60 years, participants with poor balance, and participants who were slower on the sit-to-stand-test and timed 4-m walk (Table 4). These results show that the 10-item Icon-FES was as sensitive to group differences relating to falls risk factors as the 30-item version. For FES-I, scores were significantly higher for those participants with lower education level, history of falls since the age of 60 years, and who were slower on the timed 4-m walk. Most effect sizes for statistically significant between-group differences were similar for both Icon-FES versions and FES-I.
Means and standard deviation of 30-item Iconographical Falls Efficacy Scale (Icon-FES; 30–120 scale), 10-item Icon-FES (10–40 scale) and medians and interquartile range of Falls Efficacy Scale – International (FES-I, 16–64 scale) for subgroups based on demographic characteristics, fall risk factors and cognitive performance.
| Group 1 | Group 2a | Effect sizeb | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 30-item Icon-FES | 10-Item Icon-FES | FES-I | n | 30-item Icon-FES | 10-Item Icon-FES | FES-I | 30-item Icon-FES | 10-Item Icon-FES | FES-I | |||
| Age, yearsc | ≤71 | 54 | 51.1±12.9 | 17.7±4.8 | 23.0 [19.0–26.3] | >71 | 46 | 52.3±13.0 | 18.1±4.5 | 22.0 [20.0–28.3] | 0.10 | 0.11 | 0.14 |
| Gender | Female | 82 | 52.3±13.0 | 18.0±4.7 | 23.0 [20.0–28.0] | Male | 18 | 48.7±12.2 | 17.4±4.4 | 21.0 [19.0–24.5] | 0.28 | 0.12 | 0.50 |
| Education level | Incomplete primary school | 27 | 55.5±14.2 | 19.1±5.2 | 26.0 [22.0–32.0] | Complete primary school or above | 73 | 50.2±12.2 | 17.5±4.4 | 21.0 [19.0–26.0]** | 0.40 | 0.34 | 0.64 |
| Falls since 60 | Yes | 56 | 54.8±12.8 | 19.1±4.5 | 23.0 [21.0–28.8] | No | 44 | 47.6±12.0** | 16.4±4.4** | 20.5 [19.0–24.0]** | 0.58 | 0.61 | 0.58 |
| Falls Last year | Yes | 15 | 52.9±14.9 | 17.7±5.0 | 23.0 [20.0–30.0] | No | 85 | 51.4±12.6 | 17.9±4.6 | 22.0 [19.5–27.0] | 0.11 | 0.06 | 0.09 |
| Balance eyes open, secondsc | ≤6.7 | 50 | 55.5±13.6 | 19.2±4.7 | 23.0 [20.0–29.0] | >6.7 | 50 | 47.8±10.9** | 16.6±4.3** | 22.0 [19.0–26.0] | 0.62 | 0.59 | 0.36 |
| 4-meter walking test, secondsc | >5.12 | 50 | 55.6±13.6 | 19.3±4.8 | 23.0 [20.0–30.0] | ≤5.12 | 50 | 47.6±10.8** | 16.5±4.2** | 21.0 [19.0–26.0]* | 0.65 | 0.61 | 0.52 |
| Sit-to-stand test, secondsc | >15.03 | 50 | 54.9±14.0 | 18.9±4.8 | 23.0 [19.8–30.0] | ≤15.03 | 50 | 48.4±10.8* | 16.9±4.3* | 22.0 [19.8–26.0] | 0.51 | 0.46 | 0.45 |
| MMSE, scorec | <27 | 42 | 52.5±13.1 | 18.3±4.6 | 23.0 [20.0–29.0] | ≥27 | 58 | 50.9±12.8 | 17.6±4.7 | 22.0 [19.0–26.5] | 0.12 | 0.17 | 0.28 |
Values are mean±standard deviation or median [interquartile range].
MMSE, Mini-Mental State Examination.
The objective of this study was to translate and cross-culturally adapt the Icon-FES into Brazilian-Portuguese and to test the measurement properties of the 30-item and 10-item versions of the Icon-FES-Brazil. During the translation and cross-cultural adaptation process, only one item or activity from the original Icon-FES had to be modified because it was not considered a common activity of daily living for the Brazilian community-dwelling older population (i.e. lack of experiential equivalence). Our findings revealed that both versions of the Icon-FES-Brazil showed acceptable estimates for all tested measurement properties and may be considered a better tool than the FES-I at assessing concern about falling, suggesting that the long and short versions can be used in clinical practice and research.
Both versions of the Icon-FES-Brazil showed internal consistency and reproducibility estimates similar to the original English version of the questionnaire. The Cronbach alpha coefficients found for the 30-item and 10-item Brazilian-Portuguese versions were respectively 0.94 and 0.83, which was similar to the coeficients reported for the English versions of the questionnaire (30-item version, alpha=0.96; 10-item version, alpha=0.87).16 The high internal consistency indicates that all items from both Icon-FES-Brazil versions adequately measure the construct related to concern of falling. Similarly to the English version, the Brazilian-Portuguese versions showed excelent reproducibility (i.e., ICC greater than 0.90) and absence of floor and ceiling effects.16 In addition, the SMD and MDC values found in this study indicate that the magnitude of the change required to exceed the variability of the Icon-FES questionnaires is 7.2 points for the 30-item version, and 3.4 points for the 10-item version. Clinicians should be aware of these values when assessing concern of falling using these instruments in clinical practice. It has been suggested that given the wide range of activities including of variety of more demanding balance-related activities, the Icon-FES may be used as treatment utility tool to identify target activities for cognitive behavioral therapy program37 and could possibly be more sensitive to detect changes in levels of concern.38
The validity of the Icon-FES-Brazil questionnaires for measuring the construct of concern of falling was investigated using the FES-I, an existing well-validated measure.15,26 The FES-I score showed good to excellent relationship with both versions of the Icon-FES-Brazil. The magnitude of correlation coefficient found for the long version of Icon-FES-Brazil (rho=0.83, p<0.001) was even higher than the one found for the original English version (rho=0.74, p<0.001).16 The 30-item and 10-item versions of the Icon-FES-Brazil were able to discriminate between groups relating to history of falls (i.e., experienced falls since the age of 60 years), balance and both measures of mobility (i.e., sit-to-stand and 4-m walking tests). FES-I, however, was able to discriminate between groups relating to education level, falls since the age of 60 and 4-m walking test. Given that our sample consisted of older people living in the community, the results from the discriminative validity analyses provide support to the ability of the Icon-FES-Brazil versions to assess concern about falling in highly functioning older people and suggest that Icon-FES is better at assessing ‘true’ concern of falling than the FES-I. We would argue, however, that the lack of difference between groups for gender, history of falling in the last year and age might be due to the lower proportion of males and fallers in the preceding year as well as the inclusion of a relatively young population (i.e. median age of 71 years) as compared to the validation study of the original English version. Other advantages of the Icon-FES over the existing concern about falling measures are its normal distribution. Our results provide support to the normal distribution of the Icon-FES-Brazil and the non-normal distribution of the FES-I.
The Icon-FES is an innovative tool that measures the level of concern of falling during a range of daily activities using pictures and brief texts embedded within specific environmental contexts. Hence, the Icon-FES might be even better than the FES-I at assessing concern about falling in countries or population with low education levels. In fact, our results for the discriminative validity analysis showed that the Icon-FES-Brazil scores were not affected by the different levels of education. In contrast, the education level of the participants influenced the FES-I scores with the ‘incomplete primary school’ group reporting higher concern of falling compared to ‘complete primary school and above’ group. This result, however, should be further confirmed in futures studies with a larger proportion of older people with low education levels, including illiterates.
Given that our sample was drawn from the community, a limitation of this study is that our results may not be generalized to, for instance, frailer older people. Although our sample size was based on a COSMIN benchmarks to be rated as having excellent methodology (i.e. more than 100 patients), the lack of sample size calculation to obtain an optimal number of participants should also be seen as a limitation. Factor analysis of the 30-item English version revealed one factor with two dimensions assessing concerns of less and more demanding daily activities. Future studies with larger sample sizes are still needed to investigate whether these questionnaires are also sensitive in detecting changes in levels of concern among frail older people and the Icon-FES-Brazil versions show similar overall structure to the original English version. Future studies investigating the predictive ability and responsiveness of the Icon-FES are still warranted.
The 30-item and the 10-item Icon-FES-Brazil proved to have acceptable measurement properties to assess concern of falling among Brazilian community-dweeling older people. Our findings also demonstrated that the short and long versions of the Icon-FES-Brazil were better than FES-I at assessing concern about falling. Therefore, we would advocate these tools to be used in clinical practice and in future research.
Authors’ contributionThe study was conceived and designed by MRF, KD, DS, RZP and CMP. The data was collected and analyzed by MRF, BYE, MSF, GA. The interpretation of the data and results were made by all authors. MRF, BYE, MSF, GA prepared the first draft of the manuscript and successive drafts were contributed by all authors. KD, DS, RZP and CMP contributed with critical revision for the review. The final version of the manuscript was approved by all authors.
Conflicts of interestThe authors declare no conflicts of interest.
This work was supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) [grant numbers 2015/07704-9, 2015/23884-7, 2016/15697-5 and 2017/15539-3].



