







To evaluate the Kinesio Taping effects with different directions and tensions on the strength of rectus femoris and range of movement of the knee in healthy individuals, but with a muscle imbalance caused by exposure to a continuous vibration.
MethodsThis is a randomized controlled trial. The subjects were randomly allocated into two groups: Group application of the Kinesio Taping using origin to insertion and Group application of the Kinesio Taping using insertion to origin. In both groups the dominant limb received the application of Kinesio Taping on rectus femoris (experimental limb) while the non-dominant limb was used as control of the study (control limb). Three assessments were carried out with each subject at different time-points (baseline, post-application, 24h later). These evaluations were performed with 0%, 10% and 75% of tension. The continuous vibration was conducted on the patella tendon for 20min before the first evaluation on each subject. A handheld dynamometer and a digital goniometer were used to evaluate the strength of the rectus femoris and the range of movement of the knee.
ResultsThe sample consisted of 42 subjects, 79% women and 21% men, mean age 20.5 (SD=4.6), body mass index average of 18.7 (SD=2.34). There were no between-group differences for all outcomes.
ConclusionThis study suggests that the use of Kinesio Taping in healthy individuals did not change muscle strength or increase range of movement. Future clinical trials are recommended for symptomatic patients.
Trial registration: NCT02501915 (https://clinicaltrials.gov/ct2/show/NCT025019150).
Kinesio Taping (KT) is a technique developed in Japan by Kenzo Kase in 1976, which uses a specific methodology with an elastic tape, the Kinesio Tex Tape (KTT). KTT is composed of a material that differs from other tapes since it presents unique qualities (elasticity, adherence, mechanical, texture and recoil) which may promote an increase of the somatosensory stimulation and consequently mechanoreceptors and proprioceptive input, enabling responses to inhibition, activation, muscle facilitation, in addition to many other mechanical effects.1–4
According to the recent literature, there are many studies relating to KT, muscle strength and ROM. In one recent systematic review and meta-analysis about Kinesio Taping and muscle strength, the authors concludes that Kinesio Taping does not increase muscle strength in healthy individuals and probably the effects are not dependent on muscle for the taping.5
There are some studies with healthy individuals, that found positive results such as reduced time to reach the peak torque,6,7 reduced movement time excursion on dorsiflexion8 and increased peak torque on the gastrocnemius.9 On the other hand, there are also some recent studies that did not find any positive results.10–12
According to the method, the increase of muscle strength occurs when it is applied with the facilitation technique (application from the muscle origin to its insertion with tension between 15% and 35%). The application in favor of muscle contraction improves neural communication with the mechanoceptors, increasing the number of motor units recruited. The inhibition technique (application from insertion to the muscle origin) promotes an inhibition of the motoneurons with consequent relaxation of the muscles and does not promote increases of muscle function.1 However, in relation to the presence of facilitation and inhibition, a study with healthy subjects did not find any difference on those applications. This study used a different way to tape, using the antagonist, but they evaluated the agonist effect.13
Regarding range of movement (ROM), many studies have been conducted with KT. Therefore, most of them attempt to identify the increase of ROM through the reduction of pain on some specific injury.4,14,15 While other studies, have also researched the increased ROM in healthy subjects and in normal conditions.3,8,9,16,17
Considering that most of the studies evaluated the effects of KT on muscle strength and ROM in healthy subjects, few studies have evaluated the hypothesis of facilitation and inhibition proposed by the KT method, and there are also few studies that evaluated the effects of KT according to the different tensions. Therefore, this study aims to evaluate the Kinesio Taping effects with different directions and tensions on the strength of rectus femoral and the ROM of the knee on healthy individuals, but with a muscle imbalance caused by exposure to a continuous vibration before the tape.
MethodsThis is a randomized controlled trial, in which the principal investigator who assessed the outcomes and the subjects were masked to the allocation of intervention.
The study was conducted in a Biomechanics laboratory located in a private institution in the city of Goiania, Brazil, was approved by the Ethics Committee of the Universidade Salgado Oliveira (UNIVERSO), Goiânia, Goiás, Brazil with the number 561.500, according to the Resolution of the Ministry of Health 466/12, and the subjects gave informed consent. This trial was prospectively registered at ClinicalTrials.gov (NCT02501915).
The inclusion criteria were: subjects of both genders, any race, ages between 18 and 40 years, healthy, with no musculoskeletal disorders, and no history of injury in the last six months in the lower limbs. The exclusion criteria were: subjects with body mass index greater than 24.99, with musculoskeletal disorders and related pain, history of tape allergy or skin sensitivity, any condition counter indicating physical activity, nerve root compromise, cardio respiratory conditions, pregnancy or previous knowledge of KT. All the subjects were asked to not exercise between the evaluations.
The sample of this study was determined based on a sample size calculation carried out in a pilot study with six individuals, to identify the correlation between the ratio found in KT applications for the different mean values found in the evaluations of the same. In this way, the Pearson Linear Correlation Coefficient r=0.5 was used, considering a level of significance of α=5%, also with 80% of statistical power.
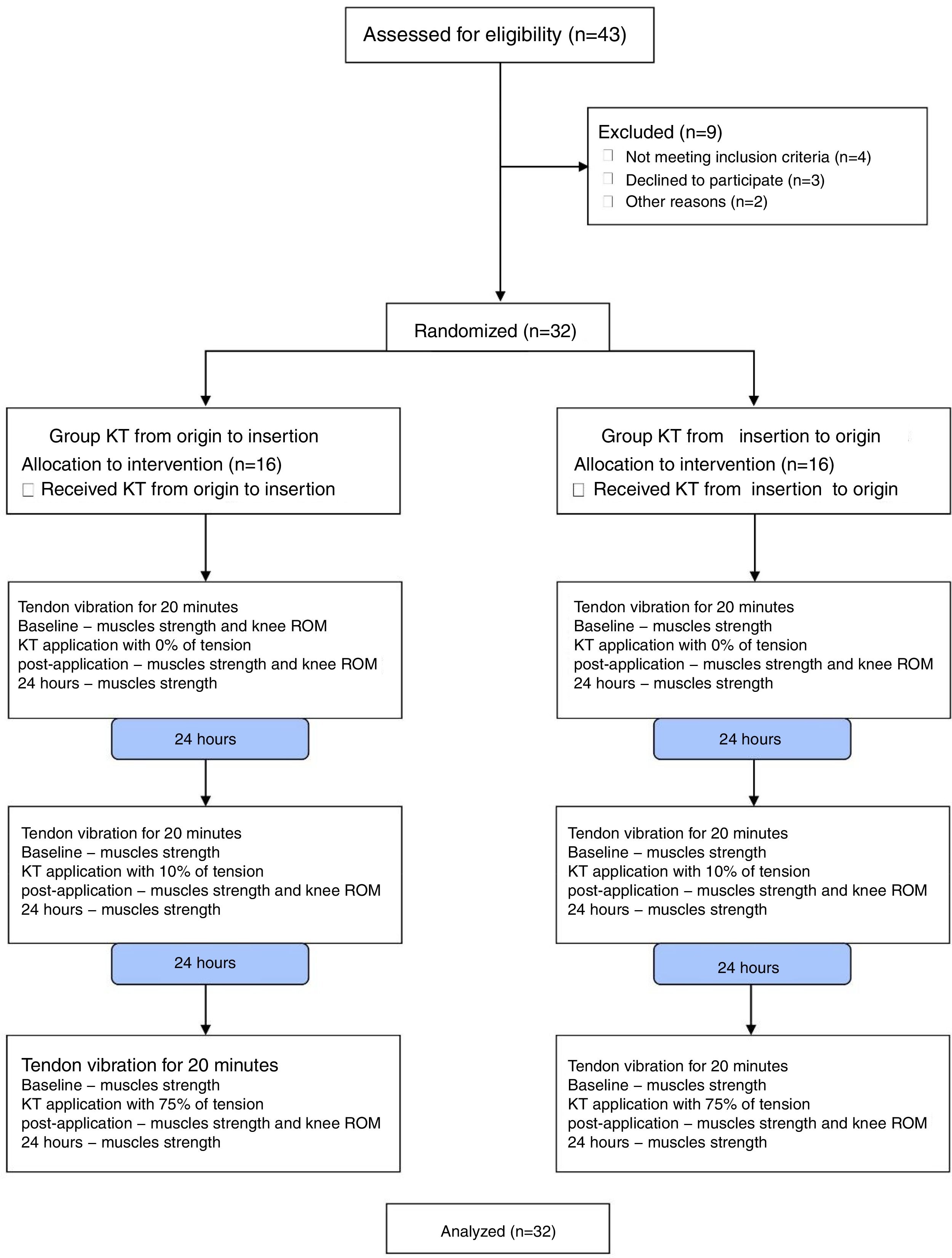
The participants were randomly allocated into two groups: Group KTT application from the muscle origin to its insertion, and Group KTT application from insertion to origin as shown in the diagram (Fig. 1). The dominant limb received the KTT application and the non-dominant limb was the control of the study on both groups. The study participants’ recruitment period was from February of 2014 to January of 2015. Participant selection and randomization were conducted by a person who was not involved with the interventions. The randomization schedule was generated by http://www.randomization.org. The intervention was conducted by physical therapist who has all the KT seminars and more than 4 years’ experience with the tape. The subjects and the principal investigator of the study were blinded to the treatment allocation.
The primary outcomes were muscle strength and ROM. The strength of the rectus femoral was evaluated using a hand held dynamometer (Lafayette), fixed on apparatus to stabilize it. The ROM of the knee was evaluated through a digital goniometer.
Muscle strength was evaluated nine times. First, prior to KT application; second immediately after KT placement; and third, 24h later. These evaluations were done with 0% of the tape tension; with 10% (paper off tension); and with 75%–100% (total tension) on both groups. The ROM was assessed four time; before and after the tape; with 0%; after the tape with 10%; and after the tape with 75% of tension.
None of the subjects of this study knew into which group they were allocated. In addition, they were informed during the explanation of the procedures that there would be a placebo group, in which they may, or may not be allocated. This was used with the intention of minimizing psychological conditions, such as placebo effects. The subjects were also asked about their knowledge, because the study intended to have a deceptive placebo, so the subjects must be free of expectations as much as possible. An assessment questionnaire was used at the end of the study to verify if the subject knew in which group they belong, and if they also had any previous knowledge about the KT.
Before the beginning of the procedures, the skin was cleaned with clear water, and excess oils removed using cleaning alcohol. In the case of excess of hair on the leg, the area was shaved.
The continuous vibration was conducted on the patella tendon for 20min before the first strength evaluation was completed on each subject. According to Cardinale and Bosco,18 the mechanical vibration (MV) is a stimulus characterized by an oscillatory motion, and this MV is a strong stimulus to the muscle, effecting and causing the need to modulate its stiffness quickly. Studies on the effects of MV on the neuromuscular system showed that it causes a proprioceptive deficit during and after the tendon stimulation. The effects of such MV stimulation are similar to a voluntary contraction, causing intrafusal muscle thixotropy, resulting in cross-bridge detachment from actin and myosin.19
After the vibration, the first intervention was performed with the KT without tension (0%) on the rectus femoral (RF) on the dominant limb (experimental) with the patient lying in a supine position with the knee off the table with 90 degrees of flexion, placing the muscle on an elongated position. This way the subject was unable (blinded) to watch the KT application. The same procedure was performed on the second and third day with the specific tension.
For the strength assessment, the subjects were positioned seated at the end of the table with 90 degrees of knee flexion, and the dynamometer placed 5cm above the lateral malleolus on the anterior part of the leg. They were instructed to make three maximum isometric contractions (MIC) with five seconds each, and the average of those three was used as the strength value. The hand held dynamometer used has excellent reproducibility for assessment of quadriceps muscle strength and is considered equivalent to the use of an isokinetic dynamometer for this muscle group.20
For the ROM assessment, the subjects were positioned on a prone position with the knee extended. The goniometer's fixed arm was positioned parallel to the lateral surface of the femur, the movable arm was positioned parallel to the lateral surface of the fibula, and the axis was positioned in the knee joint line. The subjects were instructed to perform the maximum knee flexion.
Data were analyzed in Statistical Package for Social Science (SPSS), version 22.0 and was considered p<0.05. An intention to treat analysis was conducted. The Shapiro–Wilk test was used to verify the normality of the data. Results were expressed as mean, standard deviation and 95% confidence intervals (CI). To compare the strength and ROM, the t test for independent samples was used to between-group comparisons (KTT×Without KTT; Group KTT application from the origin to insertion×Group KTT application from the insertion to origin) and the analysis of variance (ANOVA) for repeated measures with post hoc Bonferroni was used to within-group comparisons (0%×10%×75%; pre-application×pos-application×24h).
ResultsThe sample consisted of 43 subjects, 79% women and 21% men, with a mean age of 20.5 (SD=4.6) years, body mass index average of 18.7 (SD=2.34), 40.6% practicing some exercise weekly. When they were asked about their knowledge about the KT, four subjects answered they knew something about it, so they were excluded from the study. The other three declined to participate, and two failed to complete the study. In this context, the assessment of strength and ROM were made on 32 subjects (Group KTT application from the origin to insertion – n=16; Group KTT application from the insertion to origin – n=16).
No between-group differences were found on the strength of the RF on the dominant limb (KTT) between groups, with the different tensions (0%, 10%, and 75%), and times (pre-application, post-application and 24h) (p>0.05) Table 1. When the dominant (KTT) and non-dominant (without KTT) limbs were compared via unpaired t test, also no significant differences were found as well in both groups (p>0.05) Table 2. The Within-group differences related to muscle strength are shown in Fig. 2.
Between-groups comparison, mean (SD) and mean difference and 95% CIs for the outcomes of the study (n=32).
| Outcomes | Mean (SD) | Mean differences (95% CI) | p | |
|---|---|---|---|---|
| Group origin to insertion | Group insertion to origin | |||
| Muscle strength 0% | ||||
| Baseline | 21.30 (7.20) | 20.69 (6.46) | 0.60 (−4.34 to 5.54) | |
| Post-application | 22.59 (7.20) | 22.95 (6.59) | −0.36 (−5.36 to 4.63) | 0.88 |
| 24h | 22.85 (7.51) | 23.11 (7.62) | −0.26 (−5.72 to 5.19) | 0.92 |
| Muscle strength 10% | ||||
| Baseline | 22.34 (7.40) | 25.00 (6.56) | −2.64 (−7.69 to 2.40) | |
| Post-application | 22.75 (7.96) | 25.46 (6.56) | −2.71 (−7.98 to 2.55) | 0.30 |
| 24h | 21.88 (6.70) | 23.19 (5.97) | −1.31 (−5.89 to 3.26) | 0.56 |
| Muscle strength 75% | ||||
| Baseline | 21.76 (5.60) | 22.38 (6.43) | −0.61 (−4.98 to 3.75) | |
| Post-application | 22.89 (6.50) | 22.72 (6.10) | 0.16 (−4.38 to 4.71) | 0.94 |
| 24h | 22.53 (6.20) | 23.50 (6.95) | −0.96 (−5.72 to 3.79) | 0.68 |
| ROM 0% | ||||
| Baseline | 132.81 (5.75) | 135.32 (5.03) | −2.51 (−6.41 to 1.38) | |
| Post-application | 134.50 (7.23) | 134.40 (4.76) | 0.09 (−4.32 to 4.51) | 0.96 |
| ROM 10% | ||||
| Baseline | 132.81 (5.75) | 135.32 (5.03) | −2.51 (−6.41 to 1.38) | |
| Post-application | 135.33 (7.82) | 139.12 (5.49) | −3.78 (−8.66 to 1.09) | 0.12 |
| ROM 75% | ||||
| Baseline | 132.81 (5.75) | 135.32 (5.03) | −2.51 (−6.41 to 1.38) | |
| Post-application | 134.80 (7.80) | 137.71 (5.38) | −3.01 (−7.85 to 1.81) | 0.21 |
Muscle strength was measured by hand held dynamometer and expressed in Kgf; ROM was measured by goniometer and expressed in degrees. ROM, range of movement.
Between-members comparison, mean (SD) and mean difference and 95% CIs for the outcomes of the study (n=32).
| Outcomes | Mean (SD) | Mean differences (95% CI) | p | |
|---|---|---|---|---|
| KTT | Without KTT | |||
| Group origin to insertion | ||||
| Muscle strength 0% | ||||
| Baseline | 21.30 (7.20) | 20.32 (7.64) | 0.98 (−4.38 to 6.33) | |
| Post-application | 22.59 (7.20) | 21.53 (8.42) | 1.05 (−4.61 to 6.73) | 0.71 |
| 24h | 22.85 (7.51) | 21.17 (8.43) | 1.67 (−4.09 to 7.43) | 0.56 |
| Muscle strength 10% | ||||
| Baseline | 22.34 (7.40) | 21.76 (9.54) | 0.58 (−5.58 to 6.74) | |
| Post-application | 22.75 (7.96) | 22.83 (10.30) | −0.09 (−6.75 to 6.58) | 0.98 |
| 24h | 21.88 (6.70) | 21.10 (8.20) | 0.78 (−4.62 to 6.18) | 0.77 |
| Muscle strength 75% | ||||
| Baseline | 21.76 (5.60) | 19.67 (7.30) | 2.09 (−2.64 to 6.82) | |
| Post-application | 22.89 (6.50) | 20.79 (7.80) | 2.09 (−3.09 to 7.29) | 0.42 |
| 24h | 22.53 (6.20) | 21.47 (7.70) | 1.06 (−4.00 to 6.14) | 0.67 |
| ROM 0% | ||||
| Baseline | 132.81 (5.75) | 132.90 (7.01) | −0.09 (−4.72 to 4.53) | |
| Post-application | 134.50 (7.23) | 132.05 (8.46) | 2.44 (−3.23 to 8.12) | 0.39 |
| ROM 10% | ||||
| Baseline | 132.81 (5.75) | 132.90 (7.01) | −0.09 (−4.72 to 4.53) | |
| Post-application | 135.33 (7.82) | 134.77 (8.02) | 0.56 (−5.15 to 6.27) | 0.84 |
| ROM 75% | ||||
| Baseline | 132.81 (5.75) | 132.90 (7.01) | −0.09 (−4.72 to 4.53) | |
| Post-application | 134.80 (7.80) | 134.89 (9.37) | −0.19 (−6.41 to 6.02) | 0.95 |
| Group insertion to origin | ||||
| Muscle strength 0% | ||||
| Baseline | 20.69 (6.46) | 20.25 (7.19) | 0.44 (−4.48 to 5.38) | |
| Post-application | 22.95 (6.59) | 21.64 (5.57) | 1.31 (−3.09 to 5.72) | 0.55 |
| 24h | 23.11 (7.62) | 23.01 (7.29) | 0.09 (−5.28 to 5.48) | 0.97 |
| Muscle strength 10% | ||||
| Baseline | 25.00 (6.56) | 23.13 (5.72) | 1.85 (−2.58 to 6.29) | |
| Post-application | 25.46 (6.56) | 23.24 (6.56) | 2.22 (−2.51 to 6.96) | 0.35 |
| 24h | 23.19 (5.97) | 21.05 (4.96) | 2.14 (−1.82 to 6.10) | 0.28 |
| Muscle strength 75% | ||||
| Baseline | 22.38 (6.43) | 21.28 (4.81) | 1.10 (−2.99 to 5.19) | |
| Post-application | 22.72 (6.10) | 21.96 (4.95) | 0.76 (−3.23 to 4.76) | 0.70 |
| 24 hours | 23.50 (6.95) | 21.63 (5.69) | 1.87 (−2.71 to 6.45) | 0.411 |
| ROM 0% | ||||
| Baseline | 135.32 (5.03) | 134.58 (4.14) | 0.74 (−2.57 to 4.07) | |
| Post-application | 134.40 (4.76) | 134.37 (6.32) | 0.02 (−4.01 to 4.06) | 0.99 |
| ROM 10% | ||||
| Baseline | 135.32 (5.03) | 134.58 (4.14) | 0.74 (−2.57 to 4.07) | |
| Post-application | 139.12 (5.49) | 138.51 (5.39) | 0.61 (−3.31 to 4.54) | 0.75 |
| ROM 75% | ||||
| Baseline | 135.32 (5.03) | 134.58 (4.14) | 0.74 (−2.57 to 4.07) | |
| Post-application | 137.71 (5.38) | 136.57 (5.61) | 1.13 (−2.82 to 5.10) | 0.56 |
Muscle strength was measured by hand held dynamometer and expressed in Kgf; ROM was measured by goniometer and expressed in degrees. KTT, Kinesio Taping Technique; ROM, range of movement.
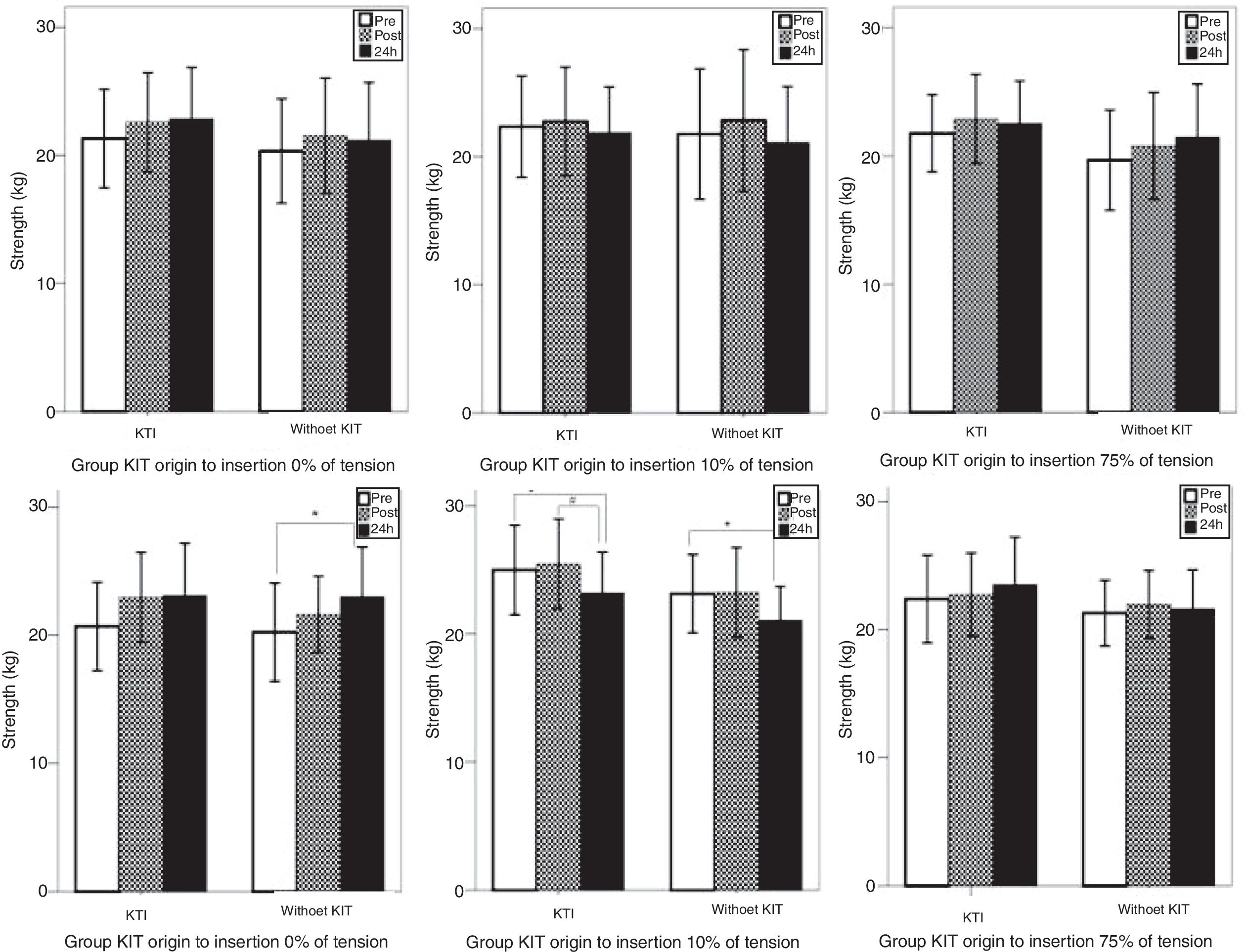
Maximum strength of rectus femoris showed in graphs comparing the different moments of the Kinesio Taping on groups KTT origin to insertion (n=16) and KTT insertion to origin (n=16). KTT, Kinesio Taping Technique; *, difference between pre and 24h; #, difference between post and 24h. p<0.05.
No differences were found on the ROM on the dominant limb (KTT) between groups, on different tensions (0%, 10%, and 75%), and times (pre-application, post-application and 24h) (p>0.05) Table 1. When the dominant (KTT) and non-dominant (Without KTT) limbs were compared via unpaired t test, no significant differences were also found as well in both groups (p>0.05) Table 2. The Within-group differences related to ROM are shown in Fig. 3.
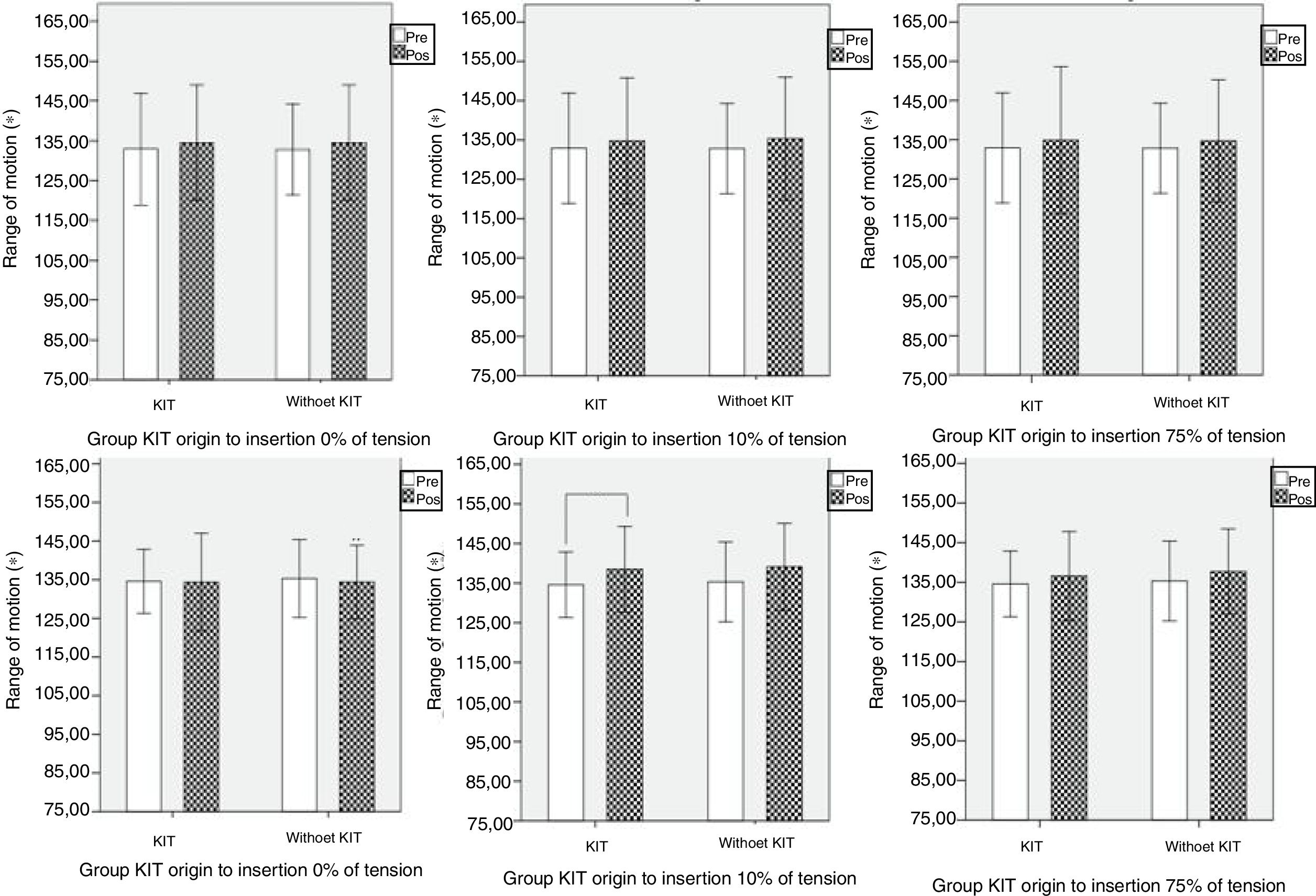
Range of movement (ROM) of the knee showed in graphs comparing the different moments of the Kinesio Taping on groups KTT origin to insertion (n=16) and KTT insertion to origin (n=16). KTT, Kinesio Taping Technique; #, difference between 0 and 10%; *, difference between pre-application and pos-application with 10%. p<0.05.
Kinesio Taping is a tool that brings a new therapy possibility in an attempt to prevent, treat and facilitate the movement dysfunctions, and consequently improves the functional activities of daily life. Most of the goals and actions of it are highlighted in theoretical and clinical levels, with no significant methodological studies showing its scientific effects.4 Much is due to various methodological misunderstandings about the method, and also from promises exposed by them that are not possible. One very common one is made by the placebo groups, using the KTT without tension and refers to a placebo condition, or even applying the tape or different kind of tape without the adequate methodology.11,12,21–25 In this study, Kinesio Taping applied with different directions, facilitation or inhibition, and with different amounts of tensions, 0%, 10% and 75%, did not improve rectus femoris strength and knee ROM immediately and 24h post-application in our sample.
According to the recent literature, there are many studies relating to Kinesio Taping, muscle strength and ROM.12,21–27 In relation to strength, three studies12,21,22 compared the effects of Kinesio Taping on quadriceps strength in health subjects and did not find any improvements when compared to a control group (no taping) and placebo group (KT without tension). Similarly, two studies23,24 did not find any improvements on quadriceps strength in soccer players when compared KT to placebo taping (KT without tension and micropore). In one systematic review and meta-analysis, the authors concluded that Kinesio Taping does not increase muscle strength in healthy individuals and probably the effects are not dependent on muscle type.5 In relation to ROM, similar results have been found on studies that evaluated the effects of Kinesio Taping, most of them did not evaluate the knee and were conducted in patients with back pain, knee arthroplasty, whiplash injury, myofascial pain, spasticity and achilles tendinopathy.28–31 Of the studies that evaluated the knee ROM, three25–27 compared the effects of KT with a placebo group (KT without tension) or control group (no taping) in subjects with osteoarthritis, no between-groups differences were found.
The studies above are clinical trials with low risk of bias and the results found in our trial corroborate with them. The strong point of the study is that were evaluated health subjects but with a muscle imbalance promoted by continuous vibration, only one study did something similar.32 Kim and colleagues32 evaluated the effects of KT on muscle activity and strength of subjects with quadriceps inhibition (90% or lower in central activation ratio) and did not find any significance on the Hoffmann reflex and maximum voluntary isometric contraction. Another strong point is that the different directions and amounts of tension were evaluated and the 0% of tension was not considered as a placebo application. The weak point is that the magnitude of the muscle imbalance and the time effect were not evaluated. Another weak point to consider is that the subjects were asymptomatic.
A possible explanation for the results of the study is that Kinesio Taping is designed as a complementary tool to help the individual facilitate a specific muscle activity, so it is not enough, alone, to reproduce isolated effects like muscle strength or gains in ROM. According to the results, Kinesio Taping should not be used in clinical practice to promote muscle strength and range of motion. The direction of application as well as the tension of the tape do not interfere with these variables and are factors that should not be considered by the clinicians when using KT.
Considering that the direction or the amount of tension are not related with muscle strength, the mechanisms that led other studies to find positive results remain unclear. Some studies have investigated the hypothesis that Kinesio Taping muscle effects are more related to the fascial movement and the relation between length and tensions. Another hypothesis raised is the placebo effect, related to psychological aspects.11 These are points that needs some in-depth study to discover their real implications. Future clinical trials with symptomatic patients and different populations should be conducted.
ConclusionThis study suggests that the use of Kinesio Taping on healthy individuals without any kind of dysfunction or injury has no influence on the strength of rectus femoris and ROM of the knee. The directions of the applications, facilitation or inhibition, and also the different amounts of tensions tested in this study did not generate any kind of changes. Future studies are recommended with different kind of injuries, imbalances and conditions to evaluate the strength and the ROM.
Conflicts of interestThe principal investigator is an International Kinesio Taping Instructor. This trial did not receive neither funding from Kinesio Taping Association nor any assistance in writing/analyzing the results of this trial. The other authors do not have any involvement with the Kinesio Taping Association.



