


To identify intervention categories encountered by physical therapists working in aquatic therapy with disabled children, using the International Classification of Functioning, Disability and Health-Children and Youth (ICF-CY).
MethodsAquatic physical therapists were asked to describe concepts related to the functioning of disabled children and their contextual factors. Data were collected in three rounds using the Delphi technique. All answers were translated (‘linked’) to the ICF-CY and analyzed to determine the degree of consensus.
ResultsAnswers were linked and organized into four diagnostic groups. Overall, in the four groups, 41 Body Functions, 8 Body Structures, 36 Activities and Participation, and 6 Environmental Factors categories were identified as intervention targets. In addition, 8 Environmental Factors that influence aquatic physical therapy were identified.
ConclusionsThis study highlights the variety of intervention categories available to aquatic physical therapists when treating children in the water.
The preamble of the constitution of the World Health Organization (WHO) underlines the importance of promoting healthy development during childhood, which entails the ability to live harmoniously in an ever-changing environment.1,2 The role of physical therapists is to overcome the limitations or improve the functioning of people as a whole, by addressing all their biopsychosocial needs.3 In the case of children and teenagers with disabilities, early intervention is a key factor influencing their physical, mental, and social recovery.4
The International Classification of Functioning, Disability and Health-Children and Youth (ICF-CY) is a classification that enables the description of changes in body function and structure, addressing both what a person can do in a standard surrounding (their level of capacity) or what they do in their usual environment (their level of performance).5
The objective of the ICF-CY is to create a framework to assess relevant aspects of functioning and health in children and youth. This is a useful classification that can be used by health systems to promote participation,6 develop ICF Core Sets,7 and identify important domains within professional interventions such as physical therapy, occupational therapy, and speech therapy.8
Aquatic Physical Therapy (APT) is defined as “the special practice of physiotherapy, with therapeutic intent toward the rehabilitation or attainment of specific physical and functional goals of individuals using the medium of water”.9 Prior studies have shown that aquatic therapy produces an improvement in motor symptoms and increases physical activity levels and that these levels are maintained six months after program completion in children with developmental disabilities and other motor disorders.10,11 Aquatic interventions also produce a positive influence on social interactions or behaviors12,13 and participation levels14 of children with neurological damage.
Despite the well-described benefits of aquatic therapy, it is unknown what areas should be routinely assessed or targeted by professionals working in this field. The present study methodology is framed within the initial phases of the Rehab-Cycle model.15 This model is a guide for healthcare professionals and provides a logical sequence of activities for the purpose of designing recommended intervention plans according to the specific needs of the individual.3,15 The first steps of this model involve a process of analysis and identification of functioning categories in children and their possible relation with relevant factors regarding the person and the environment, in order to define the therapeutic objectives.
The objectives of this study were (1) to identify intervention categories encountered by aquatic physical therapists working with children with neurological disorders [central and peripheral neurological disorders (ND), autism spectrum disorders (ASD), psychomotor delay (PMD)] and musculoskeletal disorders2 (MD), respectively, and (2) to summarize these concepts using the ICF.
MethodsThis study was exempted from ethics application by the Spanish National Ethics Committee.
Study designWe conducted a cross-sectional study using an open-ended internet 3-round survey of international experts based on the Delphi method.16 The Delphi method is a structured process based on anonymity, iteration with controlled feedback, statistical group responses, and informed feedback.17 The purpose of this method is to develop and facilitate consensus by recognized experts with knowledge in the matter under study.18
Four different groups of aquatic physical therapists participated in online and email surveys. The physical therapists in all four groups were working in APT at the time and treating children related to the four diagnostic areas cited in the study objectives.
Participants and sampling methodologyRecruitment for this study took place in spring 2012. Expert aquatic physical therapists were identified and recruited based on the following sources: (a) authors of articles, (b) lists of participants from the international courses organized by the Association International Aquatic Therapy Faculty (IATF) since the year 1998, and (c) a list of experts provided by the World Confederation of Physical Therapy-Aquatic Physical Therapy International (WCPT-APTI) in 2012. Both institutions provided consent for the disclosure of data. At the onset, the number of proposals received from the IATF and the WCPT-APTI was 97 and 53, respectively. Another 15 of these were located by searching within the articles of the specific literature.
Aquatic physical therapists had to meet the following criteria to be included as ‘experts’ in the survey: (a) they had to be qualified physical therapists, (b) work in APT, (c) work with children, (d) have over two years of experience treating children related to the four major groups of specified health conditions (ND, ASD, PMD, MD), and (e) be able to communicate either in Spanish, English, or Portuguese.
The sampling technique was non-probabilistic. The main experts responsible for APT in each participating country were contacted (representatives of the IATF and the WCPT-APTI). These organizations were asked to provide names and mailing lists of potential experts, who were subsequently contacted via email.
The proposal with the explanation of the project was sent to all those individuals included on the lists provided by both institutions. After creating a list of experts, these were sent an information sheet and an online link to the Delphi round 1 questionnaire via email.
Up to 165 experts from 34 countries (from five WHO regions) were contacted after receiving the lists provided from the IATF and WCPT-APTI groups and after reviewing the databases. These belonged to hospitals, universities, and associations. Of these, 32 were rejected as they did not fulfill the inclusion criteria, 10 refused to participate, and 25 failed to respond.
Altogether, 69 physical therapists participated in at least one round of the Delphi exercise. These included 29 participants from the WHO Region of the Americas, 33 from the European Region, 5 from the Western Pacific Region, one from the South-East Asia Region, one from the Eastern-Mediterranean Region, and none from the African Region (see online link). Table 1 shows the number of aquatic physical therapists from each language group who responded to the different Delphi rounds (35 did so in Spanish, 11 in Portuguese, and 23 in English), the median of the number of years of experience treating children, and the corresponding response rates. Because a few physical therapists did not participate in all three Delphi rounds, the number of respondents in each round was slightly different.
Participants and response rate.
| ND | ASD | PMD | MD | Total no. | Distribution of language (%) | |
|---|---|---|---|---|---|---|
| Round 1 – addressed | ||||||
| Participants (n) | 67 | 5 | 16 | 10 | 98 | |
| Respondents (n) | 49 | 3 | 11 | 6 | 69 | |
| Response rate (%) | 73 | 60 | 69 | 60 | 71 | |
| Spanish (n) | 24 | 1 | 8 | 2 | 35 | 51 |
| English (n) | 16 | 1 | 2 | 4 | 23 | 33 |
| Portuguese (n) | 9 | 1 | 1 | 0 | 11 | 16 |
| Round 2 – addressed | ||||||
| Participants (n) | 49 | 3 | 11 | 6 | 69 | |
| Respondents (n) | 30 | 2 | 8 | 5 | 45 | |
| Response rate (%) | 61 | 66 | 72 | 83 | 65 | |
| Spanish (n) | 17 | 0 | 7 | 2 | 26 | 58 |
| English (n) | 11 | 0 | 1 | 3 | 14 | 31 |
| Portuguese (n) | 2 | 2 | 0 | 0 | 4 | 9 |
| Round 3 – addressed | ||||||
| Participants (n) | 49 | 3 | 11 | 6 | 69 | |
| Respondents (n) | 36 | 3 | 8 | 4 | 51 | |
| Response rate (%) | 73 | 100 | 72 | 66 | 73 | |
| Spanish (n) | 19 | 1 | 6 | 2 | 28 | 55 |
| English (n) | 10 | 0 | 1 | 2 | 13 | 25 |
| Portuguese (n) | 7 | 2 | 1 | 0 | 9 | 18 |
| No. of years treating children (median±SD) | 11.6±9.3 | 11.6±8.6 | 8.6±5.5 | 9.1±9.2 | ||
ND, neurological disorder; ASD, autism spectrum disorder; PMD, psychomotor delay; MD, musculoskeletal disorder.
The ICF-CY classification distinguishes five components of functioning, namely (1) Body Functions and (2) Body Structures; (3) Activities & Participation; (4) Environmental Factors; and (5) Personal Factors. Each component consists of several chapters, with hierarchical ICF-CY categories as the units of classification.5 The ICF-CY components make up more than 1400 ICF-CY categories, with the exception of Personal Factors, which has not yet been classified.
Data collectionThe survey was performed in three languages (Spanish, English, and Portuguese), and translated both ways, in order to ensure clear communication with the experts using the language in which they were most fluent. The translations were performed by native experts and translators, for each of the languages employed in the survey.
Each participant was granted two weeks to respond to each round. Additionally, the leading researcher (JGR) sent out reminders approximately two days before and two days after the response deadline. Participants were blinded to the identities of the other participants in the Delphi survey at all times. Each Delphi round lasted approximately two and a half months, including time to respond and to analyze the data.
In round 1, all potential participants were sent an information sheet and a link to an online questionnaire by email (link to Delphi round 1 brief questionnaire). These questionnaires requested aquatic physical therapists to provide lists of Body Functions, Body Structures, Activities and Participation, and Environmental Factors that they considered to be influenced by APT interventions. Furthermore, the questionnaires requested participants to provide lists of relevant environmental factors influencing APT interventions. The participants responded to the questionnaire directly onto a digital platform created exclusively for this study. The Delphi participants were not required to use ICF language in their responses provided during round 1.
The information sheet provided participants with background information on the study: the study aim; the definitions for Body Functions, Body Structures, Activities and Participation, and Environmental Factors according to the WHO; a detailed study time line; and instructions on completing the questionnaires.
The second Delphi round consisted of a closed-ended questionnaire that was sent to participants by email, together with accompanying instructions (link to Delphi round 2 questionnaire). This questionnaire was designed based on responses from the ICF-CY linking performed in round 1. This second questionnaire included: (a) summary lists with all Body Functions, Body Structures, Activities and Participation, and Environmental Factors named in round 1 in the corresponding Delphi group, (b) details regarding whether the participant had named each ICF-CY category in the first round, and (c) the total percentage of participants who had named each ICF-CY category in the corresponding group.
In Delphi round 3, participants who had responded to at least one of the prior two rounds were emailed a third questionnaire together with instructions (link to Delphi round 3 questionnaire). The questionnaire used in round 3 included identical ICF-CY categories as Delphi round 2, however it provided information regarding individual participant answers from round 2, together with compiled group responses from round 2 from the corresponding group. In order to reinforce the motivation for participating in round 3 and to increase the response rate, a “Scree Test”19 was performed, after which the data of the categories that were not resolved in round 2 were presented and therefore those that had not reached an 80% consensus.
Linking processThis study relied on established linking rules,20 in order to link participants’ responses from Delphi round 1 to the ICF-CY. These linking rules allow concepts to be linked to the ICF-CY categories in a systematic and standardized way. Thus, the ICF-CY language was used to provide a summary of the participants’ answers to questionnaires in rounds 2 and 3.
In order to avoid possible bias (improve reliability), calibration linking was performed by two different health professionals who were trained in the ICF-CY linking. We calculated the number and frequency of linked categories for the different groups and the overall frequency of identification for each category.
Data analysisAt the onset of the data analysis stage, two physical therapists trained in ICF-CY linked 20% of the answers separately.16 Decisions regarding which ICF-CY category should be linked to each response were agreed by consensus. The advice of a third person trained in the linking rules was sought in the case of disagreements between both physical therapists regarding the selected categories. In these cases, the two health professionals stated their pros and cons for linking the specific answer to a specific ICF-CY category, which enabled the third person to make an informed decision. Only one researcher linked 80% of the answers. Finally, a physical therapist checked the correctness of the linked categories, after all data was entered.
Response rates were analyzed using descriptive statistics. Upon completion of each Delphi round, the percentage of participants who had considered an ICF-CY category as relevant to be treated by aquatic physical therapists was calculated individually for each participating group.
The second level of the classification presents the ICF-CY categories included in the study. Here we report the ICF-CY categories that obtained a frequency of 80% or higher.16
ResultsIn total, 98 experts agreed to participate and received the survey. Of these, 69 participated in at least one round. The mean age of participants was 38.5±3.53 years, and the mean years of professional experience in water was 14.89±6.36. The mean experience working with children in water was 10.9±2.12 years.
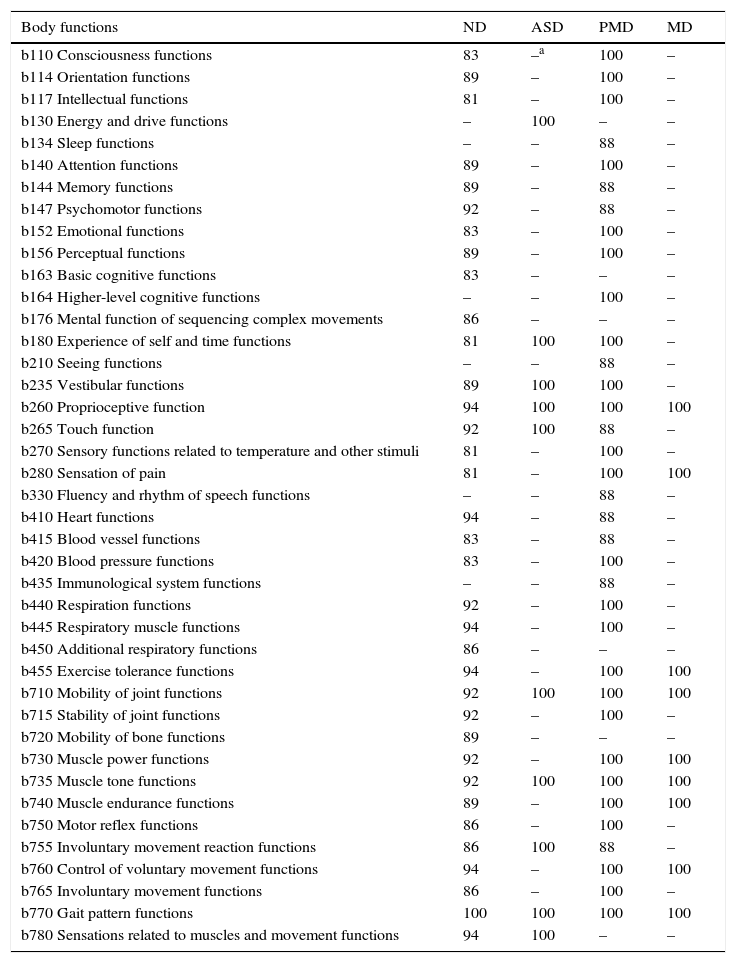
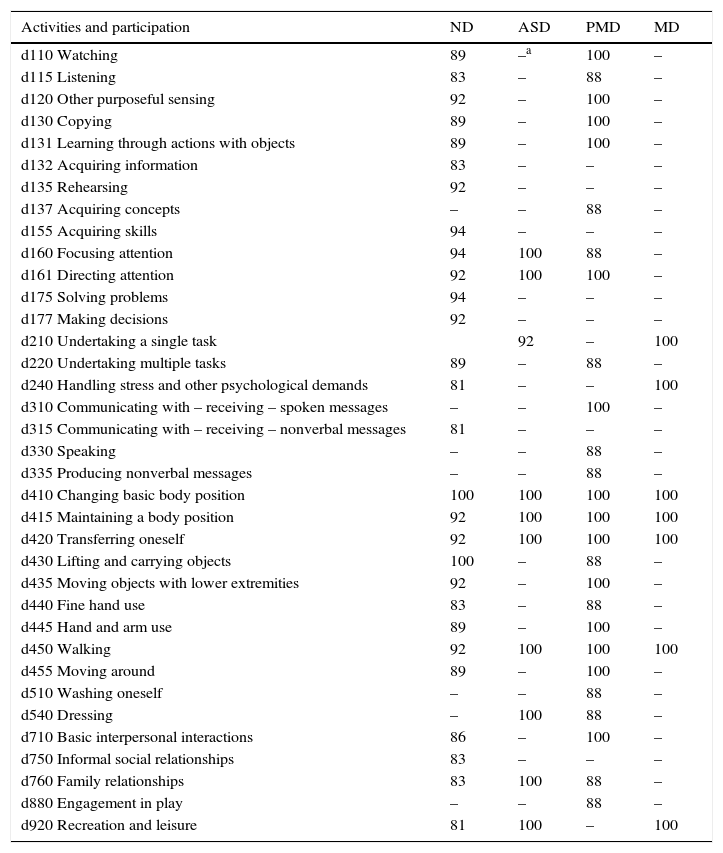
Tables 2 through 5 present the ICF-CY second level categories that 80% of participants in at least one of the four groups considered to be treated by aquatic physical therapists. These categories pertain to the Body Functions, Body Structures, Activities and Participation, and Environmental Factors components and appear according to the order of categorization of the ICF-CY.
International Classification of Functioning, Disability and Health-Children and Youth (ICF-CY). Categories in the body functions component considered to be relevant or typically influenced by aquatic physical therapy according to ≥80% of the participants in at least one group.
| Body functions | ND | ASD | PMD | MD |
|---|---|---|---|---|
| b110 Consciousness functions | 83 | –a | 100 | – |
| b114 Orientation functions | 89 | – | 100 | – |
| b117 Intellectual functions | 81 | – | 100 | – |
| b130 Energy and drive functions | – | 100 | – | – |
| b134 Sleep functions | – | – | 88 | – |
| b140 Attention functions | 89 | – | 100 | – |
| b144 Memory functions | 89 | – | 88 | – |
| b147 Psychomotor functions | 92 | – | 88 | – |
| b152 Emotional functions | 83 | – | 100 | – |
| b156 Perceptual functions | 89 | – | 100 | – |
| b163 Basic cognitive functions | 83 | – | – | – |
| b164 Higher-level cognitive functions | – | – | 100 | – |
| b176 Mental function of sequencing complex movements | 86 | – | – | – |
| b180 Experience of self and time functions | 81 | 100 | 100 | – |
| b210 Seeing functions | – | – | 88 | – |
| b235 Vestibular functions | 89 | 100 | 100 | – |
| b260 Proprioceptive function | 94 | 100 | 100 | 100 |
| b265 Touch function | 92 | 100 | 88 | – |
| b270 Sensory functions related to temperature and other stimuli | 81 | – | 100 | – |
| b280 Sensation of pain | 81 | – | 100 | 100 |
| b330 Fluency and rhythm of speech functions | – | – | 88 | – |
| b410 Heart functions | 94 | – | 88 | – |
| b415 Blood vessel functions | 83 | – | 88 | – |
| b420 Blood pressure functions | 83 | – | 100 | – |
| b435 Immunological system functions | – | – | 88 | – |
| b440 Respiration functions | 92 | – | 100 | – |
| b445 Respiratory muscle functions | 94 | – | 100 | – |
| b450 Additional respiratory functions | 86 | – | – | – |
| b455 Exercise tolerance functions | 94 | – | 100 | 100 |
| b710 Mobility of joint functions | 92 | 100 | 100 | 100 |
| b715 Stability of joint functions | 92 | – | 100 | – |
| b720 Mobility of bone functions | 89 | – | – | – |
| b730 Muscle power functions | 92 | – | 100 | 100 |
| b735 Muscle tone functions | 92 | 100 | 100 | 100 |
| b740 Muscle endurance functions | 89 | – | 100 | 100 |
| b750 Motor reflex functions | 86 | – | 100 | – |
| b755 Involuntary movement reaction functions | 86 | 100 | 88 | – |
| b760 Control of voluntary movement functions | 94 | – | 100 | 100 |
| b765 Involuntary movement functions | 86 | – | 100 | – |
| b770 Gait pattern functions | 100 | 100 | 100 | 100 |
| b780 Sensations related to muscles and movement functions | 94 | 100 | – | – |
The results are presented at the first and second levels of the International Classification of Functioning, Disability and Health-Children and Youth (ICF-CY). ND, neurological disorder; ASD, autism spectrum disorder, PMD, psychomotor delay; MD, musculoskeletal disorder.
International Classification of Functioning, Disability and Health-Children and Youth (ICF-CY). Categories in the body structures component considered to be relevant or typically influenced by aquatic physical therapy according to ≥80% of the participants in at least one group.
| Body structures | ND | ASD | PMD | MD |
|---|---|---|---|---|
| s430 Structure of respiratory system | –a | – | 88 | – |
| s710 Structure of head and neck region | – | – | 100 | – |
| s720 Structure of shoulder region | 89 | – | 100 | – |
| s730 Structure of upper extremity | 89 | – | 100 | – |
| s740 Structure of pelvic region | 83 | – | 100 | – |
| s750 Structure of lower extremity | 89 | – | 100 | 100 |
| s760 Structure of trunk | 92 | 100 | 100 | 100 |
| s770 Additional musculoskeletal structures related to movement | 92 | – | 100 | 100 |
The results are presented at the first and second levels of the International Classification of Functioning, Disability and Health-Children and Youth (ICF-CY). ND, neurological disorder; ASD, autism spectrum disorder; PMD, psychomotor delay; MD, musculoskeletal disorder.
International Classification of Functioning, Disability and Health (ICF-CY). Categories in the component activities and participation considered to be relevant or typically influenced by aquatic physical therapy according to ≥80% of the participants in at least one group.
| Activities and participation | ND | ASD | PMD | MD |
|---|---|---|---|---|
| d110 Watching | 89 | –a | 100 | – |
| d115 Listening | 83 | – | 88 | – |
| d120 Other purposeful sensing | 92 | – | 100 | – |
| d130 Copying | 89 | – | 100 | – |
| d131 Learning through actions with objects | 89 | – | 100 | – |
| d132 Acquiring information | 83 | – | – | – |
| d135 Rehearsing | 92 | – | – | – |
| d137 Acquiring concepts | – | – | 88 | – |
| d155 Acquiring skills | 94 | – | – | – |
| d160 Focusing attention | 94 | 100 | 88 | – |
| d161 Directing attention | 92 | 100 | 100 | – |
| d175 Solving problems | 94 | – | – | – |
| d177 Making decisions | 92 | – | – | – |
| d210 Undertaking a single task | 92 | – | 100 | |
| d220 Undertaking multiple tasks | 89 | – | 88 | – |
| d240 Handling stress and other psychological demands | 81 | – | – | 100 |
| d310 Communicating with – receiving – spoken messages | – | – | 100 | – |
| d315 Communicating with – receiving – nonverbal messages | 81 | – | – | – |
| d330 Speaking | – | – | 88 | – |
| d335 Producing nonverbal messages | – | – | 88 | – |
| d410 Changing basic body position | 100 | 100 | 100 | 100 |
| d415 Maintaining a body position | 92 | 100 | 100 | 100 |
| d420 Transferring oneself | 92 | 100 | 100 | 100 |
| d430 Lifting and carrying objects | 100 | – | 88 | – |
| d435 Moving objects with lower extremities | 92 | – | 100 | – |
| d440 Fine hand use | 83 | – | 88 | – |
| d445 Hand and arm use | 89 | – | 100 | – |
| d450 Walking | 92 | 100 | 100 | 100 |
| d455 Moving around | 89 | – | 100 | – |
| d510 Washing oneself | – | – | 88 | – |
| d540 Dressing | – | 100 | 88 | – |
| d710 Basic interpersonal interactions | 86 | – | 100 | – |
| d750 Informal social relationships | 83 | – | – | – |
| d760 Family relationships | 83 | 100 | 88 | – |
| d880 Engagement in play | – | – | 88 | – |
| d920 Recreation and leisure | 81 | 100 | – | 100 |
The results are presented at the first and second levels of the International Classification of Functioning, Disability and Health-Children and Youth (ICF-CY). ND, neurological disorder; ASD, autism spectrum disorder; PMD, psychomotor delay, MD, musculoskeletal disorder.
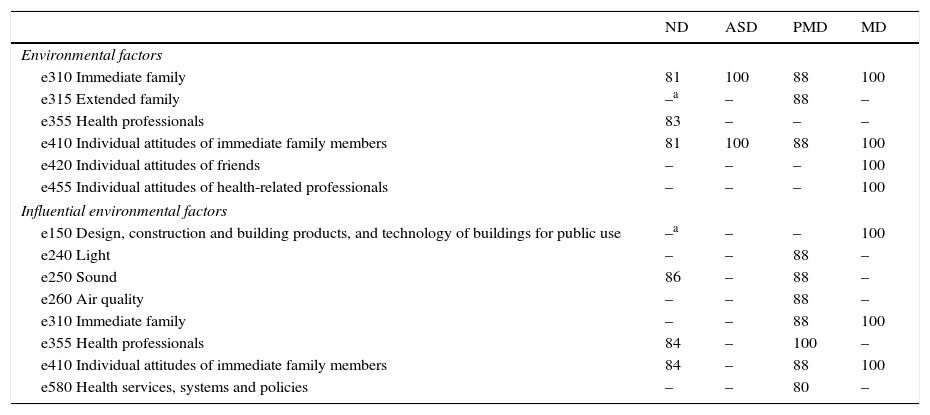
International Classification of Functioning, Disability and Health-Children and Youth (ICF-CY). Categories in the environmental factors component considered to be relevant or typically influenced by aquatic physical therapy according to ≥80% of the participants in at least one group.
| ND | ASD | PMD | MD | |
|---|---|---|---|---|
| Environmental factors | ||||
| e310 Immediate family | 81 | 100 | 88 | 100 |
| e315 Extended family | –a | – | 88 | – |
| e355 Health professionals | 83 | – | – | – |
| e410 Individual attitudes of immediate family members | 81 | 100 | 88 | 100 |
| e420 Individual attitudes of friends | – | – | – | 100 |
| e455 Individual attitudes of health-related professionals | – | – | – | 100 |
| Influential environmental factors | ||||
| e150 Design, construction and building products, and technology of buildings for public use | –a | – | – | 100 |
| e240 Light | – | – | 88 | – |
| e250 Sound | 86 | – | 88 | – |
| e260 Air quality | – | – | 88 | – |
| e310 Immediate family | – | – | 88 | 100 |
| e355 Health professionals | 84 | – | 100 | – |
| e410 Individual attitudes of immediate family members | 84 | – | 88 | 100 |
| e580 Health services, systems and policies | – | – | 80 | – |
The results are presented at the first and second levels of the International Classification of Functioning, Disability and Health-Children and Youth (ICF-CY). ND, neurological disorder; ASD, autism spectrum disorder; PMD, psychomotor delay; MD, musculoskeletal disorder.
Within the Body Functions component, a consensus of 80% or higher was obtained in at least one of the four groups for 41 ICF-CY categories. Throughout all four groups, only four categories obtained a consensus of 80% or higher. These were: “gait pattern functions” (b770) (with 100% in all categories), “proprioceptive function” (b260), “mobility of joint functions” (b710), and “muscle tone functions” (b735). Another nine categories in chapters b1 (mental functions), b2 (sensory functions and pain), b4 (functions of the cardiovascular, hematological, immunological, and respiratory systems), and b7 (neuromusculoskeletal and movement related functions) reached a consensus of 80%, or higher, in at least three groups.
Twenty-nine categories in chapters b1 (mental functions), b2 (sensory functions and pain), b4 (functions of the cardiovascular, hematological, immunological, and respiratory systems), and b7 (neuromusculoskeletal and movement-related functions) were considered as being treated by physical therapists by 100% of the participants in at least one group.
Regarding the Body Structures component, eight ICF-CY categories obtained a consensus of 80% or higher in at least one of the four groups. A consensus of 80% or higher was obtained in a single category, namely “structure of trunk” (s760). Only two categories, “structure of lower extremity” (s750) and “additional musculoskeletal structures related to movement” (s770), reached a consensus of 80% or higher in three groups. Another four categories in chapter s7 (structures related to movement) reached a consensus of 80% or higher in at least two groups.
As for the Activities and Participation component, up to 36 ICF-CY categories obtained a consensus of 80% or higher for at least one of the health conditions. The ICF-CY category “changing basic body position” (d410) reached a consensus of 100% in all four groups. Three categories [i.e., “maintaining a body position” (d415), “transferring oneself” (d420), and “walking” (d450)] reached a consensus of at least 80% in four groups. The ICF-CY categories “focusing attention” (d160), “directing attention” (d161), “family relationships” (d760), and “recreation and leisure” (d920) reached a consensus of at least 80% in three groups.
In the Environmental Factors component, the responses were divided among the factors to be influenced (six categories) and the environmental factors that influence the therapy (eight categories). Only two categories of factors to be influenced [i.e., “immediate family” (e310) and “individual attitudes of immediate family members” (e410)] reached a consensus of 80% or higher throughout all four groups. However, of the influential factors, only the ICF category “individual attitudes of immediate family members” (e410) reached a consensus of 80% or higher in three groups.
DiscussionThis study is the first to employ a Delphi technique to identify the most relevant areas of intervention in APT using the ICF-CY framework. This study contributes to the current knowledge on APT in our practices as our findings reveal a high consensus among aquatic physical therapists regarding the most relevant and common categories of functioning dealt with among children with different disorders (i.e., with ND, ASD, PMD, and MD) in APT. Furthermore, the participating experts specialized in different clinical contexts and/or treated different phases of the illness, thus extending the field of expertise. Our findings provide insight regarding the particular areas of functioning and disability that physical therapists target with their treatment interventions in water.
All four groups achieved consensus levels of 80% or higher for categories spanning all ICF-CY components: Body Functions, Body Structures, Activities and Participation, and Environmental Factors. Of the four groups, the longest lists were those pertaining to the Body Functions and Activities and Participation components. Within these components, the highest consensus obtained in most groups was related to movement categories. These results coincide with the study by Cunha et al.,21 in which aquatic therapy performed in children stabilized the progression in the lower limbs of spinal muscular atrophy type II as well as gains in functional mobility.22
In the second place, in all four groups, categories referring to Mental Function and its involvement in learning were emphasized. Our results coincide with prior studies that show how aquatic therapy helps improve certain aspects in children, such as attention,23 social behavior in the presence of ASD,24 and cerebral palsy (CP).25 These results show the importance of promoting this field of intervention within APT such as mental functions. Our results support the notion that movement and learning and their relationship are the main areas of competence among aquatic physical therapists.
Regarding Body Structures, chapter 7 (Structures related to movement) gathers 89% of the responses. In addition, the only category to have achieved consensus in the four groups was “structure of trunk” (s760). Some authors show that aquatic therapy improves the trunk involved in the subsequent gross motor function.26,27
Concerning Activities and Participation, categories related to gait and posture were emphasized. Our results coincide with prior studies23 that demonstrate that all the categories are correlated, based on movement as a primary aim. This continues to be a top priority for aquatic therapists. Other categories worth highlighting are those related to learning and the application of knowledge.
Regarding the influence of aquatic therapy upon environmental factors, there was a notable consensus regarding the support, relationships, and attitudes of family members [“immediate family” (e310) and “individual attitudes of immediate family members” (e410)]. These results are supported by everyday practice, in which family-centered interventions are a part of the intervention nucleus in children.28 According to the experts participating in this study, within the barriers for the application of aquatic therapy (Influential Environmental Factors), the category “individual attitudes of immediate family members” (e410) was the most frequent in three of the groups, followed by “sound” of the installations (e250) and “individual attitudes of health professionals” (e450), represented in two groups with values over 80%.
Our results reveal a consensus in the relevance of Body Functions and Activities and Participation in the ND and PMD groups. In clinical practice, this translates into the planning of common objectives and interventions, independent of the medical diagnosis.
This study contributes to the current knowledge on APT in our practices, as this is the first study to attempt to define the therapeutic objectives in the aquatic medium specifically targeted to the child population, based on the point of view of experts in APT. Prior research studies7,8 have used the Delphi technique to gather the opinions of experts in diseases such as CP. Schiariti et al.7 assessed functioning in CP from the perspective of different professionals (pediatricians, neurologists, physical therapists, and speech therapists). Moreover, Vargus-Adams and Martin8 described the domains according to a general therapy, while at the same time using different professionals such as neurologists, physical therapists, occupational therapists, and speech therapists. Philbois et al.29 recently verified the level of understanding of a group of health professionals regarding clinical concepts and their correlation with the ICF, confirming the use of this classification to describe domains.
One of the strengths of this Delphi study was the rate of responses, which exceeded 65% in the three rounds and reached the highest rate in round 3 (73%). Our results coincide with the response rates of prior studies, which range from 59% to 90%.7,16,30 In addition, prior studies31 indicate that it is necessary to have response rates of 50% or greater than one round in order to ensure the validity of the Delphi studies. In our study, we chose not to include new participants in each round, as this could have modified the results of the expert consensus in-between rounds. Furthermore, the validity of this Delphi study is strengthened by the fact that various relevant categories show different percentages depending on the health conditions included in each group. The long series of categories mentioned by the experts in ND reflect the high levels of burden of the health conditions included within this specialty.
This study has several limitations. In the first place, the cut-off point was set at 80% for practical reasons. In part, this may be arbitrary and is therefore subject to criticism. Indeed, several Delphi studies have used this cut-off point for practical reasons.16 The second limitation is that not all six world regions proposed by the WHO were represented (we were lacking the African region), therefore this may have influenced the results obtained by this study.
ConclusionsThis Delphi exercise demonstrated the consensus process among experts of five WHO regions, creating a preliminary list of intervention categories. This study is the first of a series of preparatory studies using the standardized WHO methodology (Core Sets) to identify a list of relevant intervention categories for APT treatments, according to the ICF-CY in children. These preparatory studies are in progress to increase generalizability, considering that any consensus process may also highlight differences, due to the varied group of experts involved. In order to validate this whole process, further clinical studies with children and the performance of a consensus conference are needed in future to implement the results.
Grant supportThis study was supported by grants from the Colegio Profesional de Fisioterapeutas de Madrid (CPFM) Research Award.
Conflicts of interestThe authors declare no conflicts of interest.
We thank all expert survey participants in the Delphi exercise for their time and invaluable contribution to the demanding questionnaires (in alphabetical order, sorted by health condition):
Neurological Disorders: Vaulet A, Itsaso A, Martín A, Madirolas B, Vanson C, Montserrat CA, Gutierrez C, Petronio C, Sa C, Uehlinger C, Burja C, Krapf C, Germano C, Bahamonde E, López E, Salguero E, Iglesias E, Moscoso F, Bottetano F, Quintanilla F, Aravena G, Styer-Acevedo J, Marcos J, Martínez J, Lee J, Abeledo JL, Nicola K, Mendes L, Lipnik L, Carroll L, Ruiz M, Barile M, Fragala-Pinkham M, Guevara ML, Carneiro MS, Risco M, Bigatello M, Soto P, Palmieri P, Rico P, Geigle P, Prashanth CG, Okano R, Alvarez R, Volmir R, Barroso R, Skoutelis V, Fabiano W, Youngeun-Lim.
Autism Spectrum Disorders: Marques A, Rodriguez C, McSharry M, Gutierres P.
PsychoMotor Delay: Moller A, Domingo A, Salar C, Casado D, Lopez G, Durango J, Gorritxategi J, Alonso M, Santiago R, Villanueva S.
Musculoskeletal Disorders: García de la Rosa A, Copponi A, McIntyre A, Ballaz L, Guille S, Harrison S.
We also extend a special thanks to Dr Alarcos Cieza for her support throughout the research and to Isabel Quintero for her assistance with the write-up and review of this study.
The following are the supplementary data to this article:



