







Muscle strength is an important component of health.
ObjectiveTo describe and evaluate the studies which have established the reference values for muscle strength on healthy individuals and to synthesize these values with a descriptive meta-analysis approach.
MethodsA systematic review was performed in MEDLINE, LILACS, and SciELO databases. Studies that investigated the reference values for muscle strength of two or more appendicular/axial muscle groups of health individuals were included. Methodological quality, including risk of bias was assessed by the QUADAS-2. Data extracted included: country of the study, sample size, population characteristics, equipment/method used, and muscle groups evaluated.
ResultsOf the 414 studies identified, 46 were included. Most of the studies had adequate methodological quality. Included studies evaluated: appendicular (80.4%) and axial (36.9%) muscles; adults (78.3%), elderly (58.7%), adolescents (43.5%), children (23.9%); isometric (91.3%) and isokinetic (17.4%) strength. Six studies (13%) with similar procedures were synthesized with meta-analysis. Generally, the coefficient of variation values that resulted from the meta-analysis ranged from 20.1% to 30% and were similar to those reported by the original studies. The meta-analysis synthesized the reference values of isometric strength of 14 muscle groups of the dominant/non-dominant sides of the upper/lower limbs of adults/elderly from developed countries, using dynamometers/myometer.
ConclusionsMost of the included studies had adequate methodological quality. The meta-analysis provided reference values for the isometric strength of 14 appendicular muscle groups of the dominant/non-dominant sides, measured with dynamometers/myometers, of men/women, of adults/elderly. These data may be used to interpret the results of the evaluations and establish appropriate treatment goals.
Muscle strength is an important component of health and physical fitness.1,2 Muscle strength has a relevant role in the performance of many activities of daily living,2 and is known to be the most important predictor of function.3 In addition, muscle weakness is related to disability.4,5 Therefore, muscle strength is an important outcome and of great interest with regards to general health.1
The most common equipment or methods that provide quantitative measures of strength, such as the isokinetic6–8 and portable dynamometers,9–11 have been shown to provide valid and reliable measures.9–15 Isokinetic dynamometers provide both isokinetic (concentric and eccentric) and isometric measures, while portable dynamometers provide only isometric measures. Although less used than the isokinetic and portable dynamometers, the myometer also yields isometric measures and has shown to provide reliable measures of strength of both adults and children.16–18 An alternative method for the quantitative evaluation of isometric strength is the modified sphygmomanometer test (MST). This low-cost method also provides valid and reliable measures of strength of various populations and muscle groups.19–21
Since the 1980s, several studies were performed with the aim to establish reference values for muscle strength for some of these equipment or methods.16,17,22–65 Reference values are essential for the correct interpretation of the evaluations and establishment of appropriate treatment goals.43,66 In addition, they are useful for the evaluation of the effectiveness of interventions30 and for the provision of important prognostic parameters, such as the possibility to return to usual activities.43 Furthermore, reference values could also be used as motivation for patients during rehabilitation interventions.54
A systematic review of the reference values of muscle strength provides a comprehensive summary of the literature along with a critical analysis of the quality of the results of the included studies. This critical summary can help professionals with the clinical decision-making process. Furthermore, the results of a meta-analysis of reference values provide a better estimative of the true value of a population, since the combined sample size of the meta-analysis is larger than that of the individual studies. Two previous systematic reviews with meta-analysis were published with the aim to synthesize the reference values for the strength of the inspiratory67 and handgrip68 muscles. However, no systematic review has addressed the appendicular and axial muscles.
Reference values are relevant for the interpretation of the evaluation and clinical decision-making process. Since several equipment or methods that provide quantitative measures of strength are available and various studies have already established the reference values for muscle strength, the objectives of the present review were to describe and evaluate the methodological quality of these studies and synthesize, using a meta-analysis, the reference values already established for healthy individuals at any age.
MethodsData sources and search strategyThis systematic review was reported in compliance with the PRISMA guidelines.69–71 All the steps described below were performed by two independent examiners (PAB and LTA). A third examiner (CDCMF) was involved to solve any disagreements.
Electronic searches were conducted in the following electronic databases: Medical Literature Analysis and Retrieval System Online (MEDLINE), Latin American and Caribbean Literature in Health Sciences Literature (LILACS), and Scientific Electronic Library Online (SciELO), from the inception to December 2017, without any language restrictions. The search strategy used in the MEDLINE database was “muscle strength” OR “isometric contraction” OR “isotonic contraction” OR “isokinetic contraction” OR “muscle force” OR “muscular strength” OR “muscular force” AND “reference value*” OR “reference range*” OR “normative search” OR “normative standard*” OR “normative data*” OR “normative score*” OR “normal range*” OR “normative value*” OR norms OR “average value*”. This search strategy was then modified to meet the requirements of the LILACS and SciELO databases.
Study selection and eligibility criteriaTo be included, the studies had to have the objective to determine the reference strength values of two or more appendicular and/or axial muscle groups of health individuals at any age and employ any equipment or method to objectively obtain the strength measures. Studies that established reference strength values of the respiratory or facial muscles were excluded. The titles and abstracts of all the retrieved articles were screened for eligibility. Then, full-text articles were screened following the predefined criteria. The reference lists of the included studies were also manually searched.
QualityThe methodological quality of the included studies was evaluated using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2). The QUADAS is an evidence-based tool for the evaluation of methodological quality of systematic reviews.72 The QUADAS was already employed with the same purpose in a previous systematic review with meta-analysis for establishing the reference strength values of the inspiratory muscles.67 The QUADAS-2 is an updated version of the QUADAS tool, which allows for a more objective and transparent rating of bias and applicability.72 The QUADAS-2 includes four domains (patient selection, index test, reference standard, flow, and timing), which are evaluated in terms of risk of bias. In addition, the first three domains are also evaluated in terms of concerns of the applicability.72 As the purpose of the present review was not to describe the results, based on comparisons with gold standard measures, the reference standard domain was not evaluated. Therefore, the following five QUADAS-2 criteria were evaluated: risk of bias, related to the domains of patient selection, index test, and flow/timing, and applicability regarding patient selection and index test.72 It was considered as having adequate quality those studies that scored at least three out of five points (more than a half of the points) on the QUADAS-2.
Study characteristicsData extraction included country, where the study was carried out; sample size; population characteristics (age and sex); equipment or method used; and muscle groups evaluated. For the population age group, the following World Health Organization classification for developed countries was used: children (0–9 years), adolescents (10–19 years), adults (20–64 years), and elderly (≥65 years).73–75
For the studies that had adequate methodological quality, i.e., positive greater than negative evaluation on the five QUADAS-2 criteria72 and showed common characteristics, which allowed for the synthesis of the data, a descriptive meta-analysis was performed. The common characteristics, which were considered, included types of contraction, equipment or method of evaluation, population characteristics, age sub-groups, muscle groups, positioning of the individuals and of the equipment, descriptive statistics used, and data collection procedures. In addition, the evaluation side for the appendicular muscles, number of trials, duration of the contractions, rest intervals, familiarization with the procedures, verbal encouragement, and measurement units. The following data were extracted: sample size, descriptive statistics, and information regarding the procedures to obtain the muscle strength measures.
Data analysisStatistical analysis of the meta-analysis was performed using the RevMan 5 software (version 5.3.5, available at https://www.statstodo.com/ ComMeans_Pgm.php). Coefficient of variation (CV) of the synthesized values was also calculated using the Excel® software. CV is a statistical measure of the dispersion of data points in a data series around the mean. It represents the ratio of the standard deviation to the mean (expressed in %), and it is a unit-free value. The CV, as a measure of variability, is considered a practical statistics for comparing the degree of variation from one data series to another, even if the means are drastically different. It also can be easily used to reflect the degree of measurement error, i.e., the lower is the obtained value, the more repeatable the method is.66
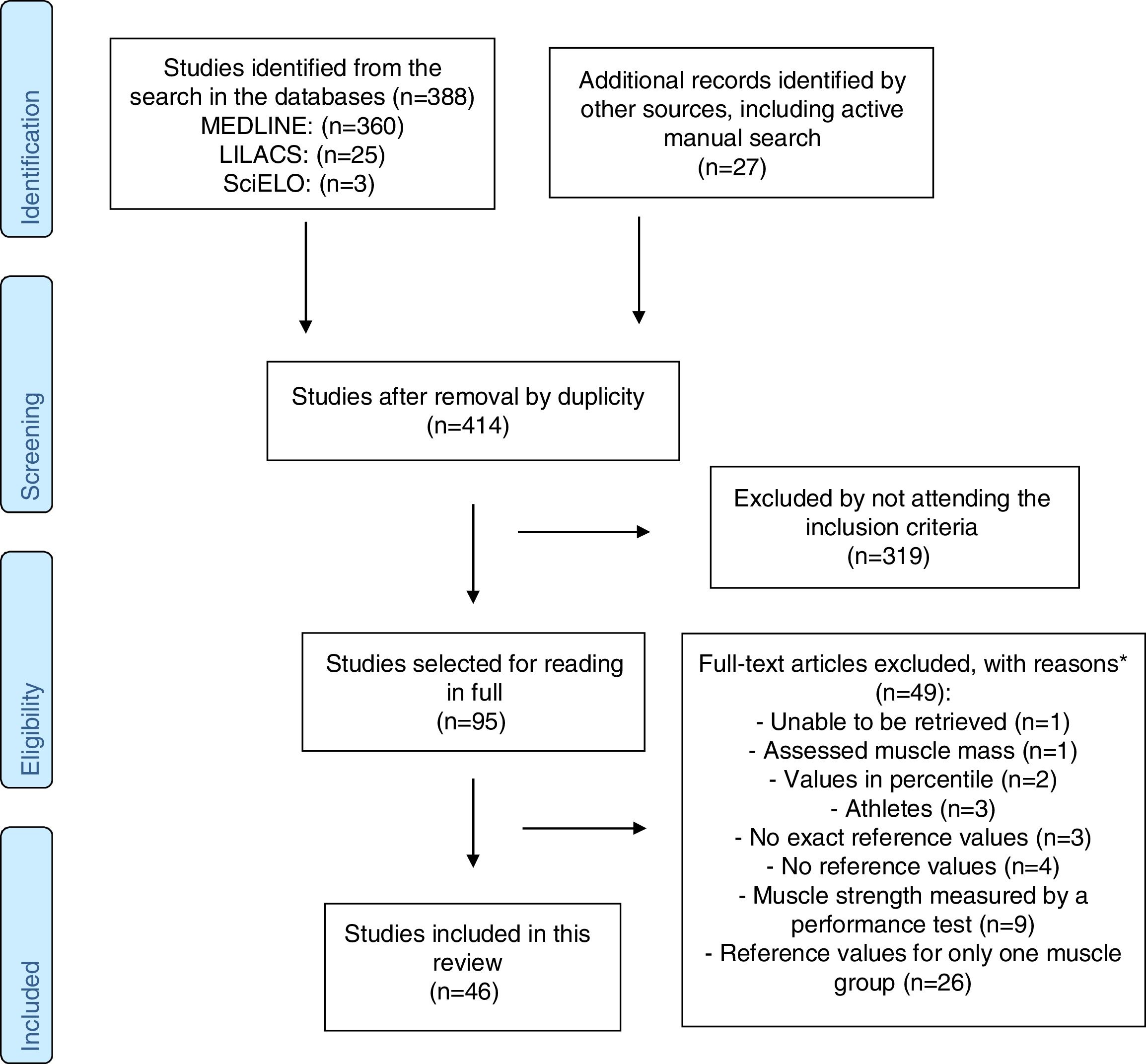
ResultsFlow of studies and qualityOf the 414 studies identified, 95 were selected for full-text evaluation, and of those, only 46 were eligible for this review (Fig. 1). As given in Table 1, the methodological quality of the included studies ranged from two to five (median=3 points). Most of the included studies scored at least three (58.7%)16,22–24,26,28–31,33–38,42,44–47,52–54,59,60,64,65 out of five points on the QUADAS-2.72 For all studies, the frequency of positive evaluation was higher than that of negative one on the five QUADAS-2 criteria72 (Table 1).
Methodological quality of the included studies, according to the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) (n=45).
| Study | Risk of bias | Applicability | Total (5 points) | |||
|---|---|---|---|---|---|---|
| Patient selection | Index test | Flow/timing | Patient selection | Index test | ||
| McKay et al.22 2017 | No | Yes | Yes | Yes | Unclear | 3 |
| Decostre et al.23 2015 | No | Yes | Yes | Yes | Yes | 4 |
| Harlinger et al.24 2015 | No | Yes | Yes | Yes | Yes | 4 |
| Molenaar et al.25 2011 | No | Unclear | Yes | Yes | Unclear | 2 |
| Riemann et al.26 2010 | No | Yes | Yes | Yes | Yes | 4 |
| Kim et al.27 2009 | No | Unclear | Yes | Yes | Unclear | 2 |
| Werle et al.28 2009 | Yes | Unclear | Yes | Yes | Unclear | 3 |
| Jansen et al.29 2008 | No | Yes | Yes | Yes | Yes | 4 |
| Meldrum et al.30 2007 | No | Yes | Yes | Yes | Yes | 4 |
| Eek et al.31 2006 | Unclear | Yes | Yes | Unclear | Yes | 3 |
| Hughes et al.32 1999 | No | Unclear | Yes | Yes | Unclear | 2 |
| Boatright et al.33 1997 | No | Yes | Yes | Yes | Yes | 4 |
| Andrews et al.34 1996 | No | Yes | Yes | Yes | Yes | 4 |
| Danneskiold-Samsøe at al.35 2009 | Yes | Yes | No | Yes | Yes | 4 |
| Stoll et al.36 2000 | No | Yes | Yes | Yes | Yes | 4 |
| Hogrel et al.37 2007 | No | Yes | Yes | Yes | Yes | 4 |
| Bohannon38 1997 | No | Yes | Yes | Yes | Yes | 4 |
| Holm et al.39 2008 | No | Unclear | Yes | Yes | Unclear | 2 |
| Hughes et al.40 1999 | No | Unclear | Yes | Yes | Unclear | 2 |
| Andersen and Henckel41 1987 | No | Unclear | Yes | Yes | Unclear | 2 |
| Backman et al.16 1995 | Yes | Unclear | Yes | Yes | Unclear | 3 |
| Crosby et al.42 1994 | Yes | Unclear | Yes | Yes | Unclear | 3 |
| Mathiowetz et al.43 1985 | No | Unclear | Yes | Yes | Unclear | 2 |
| Phillips et al.44 2000 | No | Yes | Yes | Yes | Yes | 4 |
| The National Isometric Muscle Strength (NIMS) Database Consortium45 1996 | No | Yes | Yes | Yes | Yes | 4 |
| Beenakker et al.46 2001 | Yes | Unclear | Yes | Yes | Unclear | 3 |
| Sunnegardh et al.47 1988 | Yes | Unclear | Yes | Yes | Unclear | 3 |
| Backman et al.17 1989 | Unclear | Unclear | Yes | Yes | Unclear | 2 |
| Lannersten et al.48 1993 | Yes | Unclear | No | Yes | Unclear | 2 |
| Murray et al.49 1985 | No | Unclear | Yes | Yes | Unclear | 2 |
| Rice et al.50 1989 | No | Unclear | Yes | Yes | Unclear | 2 |
| Gilbertson and Barber-Lomax51 1994 | No | Unclear | Yes | Yes | Unclear | 2 |
| Moraux et al.52 2013 | No | Yes | Yes | Yes | Yes | 4 |
| Cagnie et al.53 2007 | No | Yes | Yes | Yes | Yes | 4 |
| Peolsson et al.54 2001 | Yes | Yes | Yes | Yes | Yes | 5 |
| Vernon et al.55 1992 | No | Unclear | Yes | Yes | Unclear | 2 |
| Garcés et al.56 2002 | No | Unclear | Yes | Yes | Unclear | 2 |
| Chiu et al.57 2002 | No | Unclear | Yes | Yes | Unclear | 2 |
| Jordan et al.58 1999 | No | Unclear | Yes | Yes | Unclear | 2 |
| Salo et al.59 2006 | No | Yes | Yes | Yes | Yes | 4 |
| Paalanne et al.60 2009 | No | Yes | Yes | Yes | Yes | 4 |
| Nordin et al.61 1987 | No | Unclear | Yes | Yes | Unclear | 2 |
| Frontera et al.62 1991 | No | Unclear | Yes | Yes | Unclear | 2 |
| Ivey et al.63 1985 | No | Unclear | Yes | Yes | Unclear | 2 |
| Lundgren et al.64 2011 | Yes | Yes | Yes | Yes | Yes | 5 |
| Wiggin et al.65 2006 | No | Yes | Yes | Yes | Yes | 4 |
Yes, low risk of bias; No, high risk of bias; Unclear, unclear risk of bias.
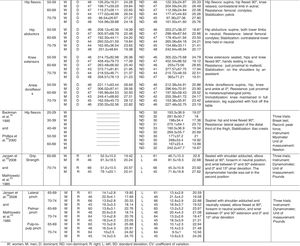
As shown in Tables 2 and 3, all studies involved samples from developed countries; the majority (95.6%) were from the Northern Hemisphere (Belgium,53 Denmark,35,41,58 Finland,59,60 France,23,37,52 Ireland,30 Netherlands,25,46 Norway,39 Scotland,51 Spain,56 Sweden,16,17,31,47,48,54,64 Switzerland,28,36 Canada,50,55 USA,24,26,27,29,32–34,38,40,42,43,45,49,61–63,65 and China).57 A large variation in sample size was noted: the largest sample included 3587 subjects, in a study that involved the evaluation of two muscle groups (knee flexors and extensors),65 whereas the smallest sample included 31 subjects, which involved the evaluation of seven muscle groups of the upper limbs.63 In only three studies (6.5%),27,56,65 a priori sample size estimation was reported. Only eight studies (17.4%) justified the separation of the reference values into different subgroups (age, sex, or side).23,25,31,33,34,38,53,62
Characteristics of the studies that established the reference values for isometric strength of the upper/lower limb and axial muscular groups.
| UPPER LIMB MUSCLES | |||
|---|---|---|---|
| Study and location | Participants (n; age; and sex) | Equipments or methods | Muscle groups |
| McKay et al.22 2017Australia | n=1000; 3–101 years;W/M: 500/500 | Hand-held dynamometer (Citec dynamometer CT 3001; CITTechnics, Groningen, Netherlands) | Elbow flexors/extensors, shoulder internal/external rotators; grip |
| Decostre et al.23 2015France | n=345; 5–79 years;W/M:198/147 | MyoWrist dynamometer | Wrist flexors/extensors |
| Harlinger et al.24 2015USA | n=180; 20–64 years; W/M:90/90 | Nicholas manual muscle tester (NMMT; Lafayette Instrument, Lafayette, IN) | Wrist and elbow flexors/extensors; shoulder internal/external rotators, abductors, flexors/extensors, and horizontal abductors/adductors |
| Molenaar et al.25 2011Netherlands | n=101; 4–12 years;W/M:52/49 | Rotterdam intrinsic hand myometer | Thumb flexors, oppositors and abductor; and abductors of the 2° and 5° fingers |
| Riemann et al.26 2010USA | n=181; 20–40 years;W/M:91/90 | Hand-held baseline 250 hydraulic push-pull dynamometer (Baseline Corporation, Invirgton, NY) | Shoulder internal/external rotators |
| aKim et al.27 2009USA | n=237; 40–86 years;W/M:93/144 | Isobex dynamometer (Cursor AG, Bern, Switzerland) | Shoulder external rotators and abductors |
| Werle et al.28 2009Switzerland | n=1023; 18–96 years;W/M:507/516 | Jamar dynamometer (Sammons Preston Rolyan, Bolingbrook, IL, USA);Pinch gauge (Baseline Fabrication Enterprises Inc., Irvingston, NY, USA) | GripLateral pinch |
| Danneskiold-Samsøe et al.35 2009Denmark | n=174; 20–80 years;W/M:121/53 | Lido active (Lido Multijoint II, Loredan Biomedical, Davis, CA, USA)Hand dynamometer (Type HKRM no.: D90116; AB Detector, Göteborg, Sweden) | Wrist and elbow flexors/extensors; shoulder internal/external rotators, abductors/adductors, and flexors/extensors;Grip (only men) |
| Holm et al.39 2008Norway | n=376; 7–12 years;W/M:191/185 | Jamar dynamometer (Jamar, Bolingbrook, IL, USA) | Grip |
| Jansen et al.29 2008USA | n=224; 65–92 years;W/M:140/84 | Jamar dynamometer;B & L pinch gauge | Grip; lateral, palmar, and pulp-to-pulp pinch |
| Meldrum et al.30 2007Ireland | n=494; 19–76 years;W/M:259/235 | Quantitative muscle assessment system | Elbow flexors/extensors; shoulder abductors/adductors |
| Hogrel et al.37 2007France | n=315; 20–80 years;W/M:168/147 | Quantitative muscle testing | Elbow flexors/extensors; shoulder internal/external rotators, abductors, flexors/extensors; grip |
| Eek et al.31 2006Sweden | n=149; 5–15 years;W/M:73/76 | Hand-held electronic dynamometer (Adapted Chatillon dynamometer; Axel Ericson Medical AB, S Vägen 12, 412 54 Gothenburg, Sweden) | Wrist extensors; elbow flexors/extensors; shoulder abductors |
| Beenakker et al.46 2001Netherlands | n=270; 4–16 years;W/M:131/139 | Hand-held dynamometer type CT 3001 (C.I.T. Technics, Groningen, The Netherlands) | Palmar pinch; Wrist extensors; elbow flexors/extensors; shoulder abductors; |
| Stoll et al.36 2000Switzerland | n=543, 20–82 years;W/M:290/253 | Hand-held pull gaugeMartin vigorimeter | Wrist and elbow flexors/extensors; shoulder internal/external rotators, abductors/adductors, flexors/extensors; grip |
| Phillips et al.44 2000Australia | n=200; 20–69 years;W/M:100/100 | Penny and Giles hand-held myometer (Penny & Giles Instrumentation Ltd., 4 Airfield Way, Christchurch, Dorset BH233TS, England) | Wrist extensors; elbow flexors/extensors; shoulder external rotators and abductors |
| Hughes et al.32 1999USA | n=120; 20–78 years;W/M:60/60 | Modified Cybex II dynamometer (Cybex, Ronkonkoma, New York) | Shoulder internal/external rotators, abductors/adductors and flexors/extensors |
| Hughes et al.40 1999USA | n=120; 20–78 years;W/M:60/60 | Cybex II dynamometer | Shoulder internal/external rotators, abductors/adductors, and flexors/extensors |
| Bohannon38 1997USA | n=231; 20–79 years;W/M:125/106 | Ametek digital hand-held dynamometer | Wrist extensors; elbow flexors/extensors; shoulder abductors and extensors |
| Boatright et al.33 1997USA | n=309; 20–97 years;W/M:208/101 | Jamar dynamometer (Asimow Engineering, Los Angeles, CA);Pinch gauge (B&L Engeneering, Santa Fe Springs, CA);Thumb abduction strength testing device | GripLateral pinchThumb abductors |
| Andrews et al.34 1996USA | n=156; 50–79 years;W/M:70/77 | Chatillon CSD400C hand-held dynamometer | Wrist extensors; elbow flexors/extensors; shoulder internal/external rotators, abductors and flexors/extensors |
| The National Isometric Muscle Strength (NIMS) Database Consortium,45 1996USA | n=493; 18–80 years;W/M:273/220 | Interface SM-250 electronic strain gauge (Interface, Inc., 7401 E. ButtherusDr., Scottsdale, AZ 85260)Jamar model 2A (Asimow Engineering Co., Santa Monica, CA.) | Elbow and shoulder flexors/extensorsGrip |
| Backman et al.16 1995Sweden | n=128; 17–70 years;W/M:63/65 | Portable electronic dynamometer (Myometer, Penny & Giles Transducers Ltd, Dorset, England)Strain gauge (Rank Stanley Cox) | Wrist extensors; elbow flexors; shoulder abductorsGrip |
| Crosby et al.42 1994USA | n=214; 16–63 years;W/M:109/105 | Jamar Dynamometer (Asimow Engineering, Los Angeles, CA).Pinch gauge (B& L Engineering, Santa Fe, CA) | GripLateral and pulp-to-pulp pinch |
| Gilbertson and Barber-Lomax51 1994Scotland | n=260; 15–92;W/M:130/130 | Jamar dynamometer (Asimov Engineering Co., Los Angeles, CA)B+L hydraulic pinch gauge (B+L Engeneering, Santa Fe Springs, CA) | GripLateral, palmar, and pulp-to-pulp pinch |
| Lannersten et al.48 1993Sweden | n=186; 19–65 years;W/M:90/96 | Electromechanical force transducer (Bofors, Suécia) | Shoulder external rotators, abductors, and flexors; |
| Rice et al.50 1989Canada | n=118; 62–92;W/M:81/37 | Modified sphygmomanometerHand-grip Stoelting dynamometer (Stoelting Co., 1350 South Kosner Ave, Chicago, IL 60651) | Elbow flexors/extensors; shoulder abductors and flexorsGrip |
| Backman et al.17 1989Sweden | n=217; 3.5–15 years;W/M:104/113 | Portable electronic dynamometer (Myometer, Penny and Gyles Transducers Ltd., Dorset, England) | Wrist extensors; elbow flexors/extensors; and shoulder abductors |
| Sunnegardh et al.47 1988Sweden | n=124; 8–13 years;W/M:65/59 | Pressure transducers (Presductor ®, ASEA) | Grip |
| Andersen and Henckel41 1987 Denmark | n=293; 6–19 years;W/M:165/128 | Strain gauge dynamometers | Elbow flexors |
| Murray et al.49 1985USA | n=40; 25–36 (young)/55–66 years (elderly); W/M:20/20 | U-shaped deflection-beam force gauges (Model X-T-KG, W. C. Dillon & Co., Inc., Van Nuys, California) | Shoulder internal/external rotators, abductors/adductors, and flexors/extensors |
| Mathiowetz et al.43 1985USA | n=628; 20–94 years;W/M:318/310 | Jamar dynamometer (Asimov Engineering Co.Los Angeles, CA)B & L pinch gauge (B&L Engineering, Tustin. CA) | GripLateral, palmar, and pulp-to-pulp pinch |
| LOWER LIMB MUSCLES | |||
|---|---|---|---|
| Study and location | Participants(n; age; and sex) | Equipments or methods | Muscle groups |
| McKay et al.22 2017Australia | n=1000; 3–101 years;W/M: 500/500 | Hand-held dynamometer (Citec dynamometer CT 3001; CITTechnics, Groningen, Netherlands)Fixed dynamometry (CSMi; HUMAC NORM, Stoughton, MA) | Ankle dorsiflexors/plantarflexors; knee flexors/extensors; hip internal and external rotators, and abductors |
| Moraux et al.52 2013France | n=345; 5–80 years;W/M:198/147 | Ankle dynamometer | Ankle dorsiflexors/plantarflexors |
| Danneskiold-Samsøe et al.35 2009Denmark | n=174; 20–80 years;W/M:121/53 | Lido active (Lido Multi Joint II, Loredan Biomedical, Davis, CA, USA) | Ankle dorsiflexors/plantarflexors; knee flexors/extensors; hip internal/external rotators, abductors/adductors, and flexors/extensors |
| Meldrum et al.30 2007Ireland | n=494; 19–76 years;W/M:259/235 | Quantitative muscle assessment system | Ankle dorsiflexors; knee flexors/extensors; and hip flexors |
| Hogrel et al.37 2007France | n=315; 20–80 years;W/M:168/147 | Quantitative muscle testing | Ankle dorsiflexors; knee and hip flexors/extensors |
| Eek et al.31 2006Sweden | n=149; 5–15 years;W/M:73/76 | Hand-held eletronic dynamometer (Adapted Chatillon dynamometer; Axel Ericson Medical AB, S Vägen 12, 412 54 Gothenburg, Sweden) | Ankle dorsiflexors/plantarflexors; knee flexors/extensors; hip abductors/adductors and flexors/extensors |
| Beenakker et al.46 2001 Netherlands | n=270; 4–16 years;W/M:131/139 | Hand-held dynamometer type CT 3001 (C.I.T. Technics, Groningen, The Netherlands) | Ankle dorsiflexors; knee flexors/extensors; hip abductors and flexors |
| Stoll et al.36 2000Switzerland | n=543, 20–82 years;W/M:290/253 | Hand-held pull gauge | Ankle dorsiflexors/plantarflexors; knee flexors/extensors; hip internal/external rotators, abductors/adductors, and flexors/extensors |
| Phillips et al.44 2000Australia | n=200; Age:20–69 years;F:100/M:100 | Penny and Gileshand-held myometer (Penny & Giles Instrumentation Ltd., 4 Airfield Way, Christchurch, Dorset BH233TS, England) | Ankle dorsiflexors; hip abductors and flexors |
| Bohannon38 1997USA | n=231; 20–79 years;W/M:125/106 | Ametek digital hand-held dynamometer | Ankle dorsiflexors; knee extensors; hip abductors and flexors |
| Andrews et al.34 1996USA | n=147; 50–79 years;W/M:70/77 | Chatillon CSD400C hand-held dynamometer | Ankle dorsiflexors; knee flexors/extensors; hip, abductors and flexors |
| The National Isometric Muscle Strength (NIMS) Database Consortium45 1996USA | n=493; 18–80 years;W/M:273/220 | Interface SM-250 electronic strain gauge (Interface, Inc., 7401 E. ButtherusDr., Scottsdale, AZ 85260) | Ankle dorsiflexors; knee and hip flexors/extensors |
| Backman et al.16 1995Sweden | n=128; 17–70 years;W/M:63/65 | Portable electronic dynamometer (Myometer, Penny & Giles Transducers Ltd, Dorset, England) | Ankle dorsiflexors; knee flexors/extensors; hip abductors and flexors |
| Backman et al.17 1989Sweden | n=217; 3.5–15 years;W/M:104/113 | Portable electronic dynamometer (Myometer, Penny and Gyles Transducers Ltd., Dorset, England) | Ankle dorsiflexors; knee flexors/extensors; hip abductors and flexors/extensors |
| Rice et al.50 1989Canada | n=118; 62–92 years;W/M:81/37 | Modified sphygmomanometer | Ankle dorsiflexors/plantarflexors; knee extensors; hip flexors/extensors |
| Sunnegardh et al.47 1988 Sweden | n=124; 8–13 years;W/M: 65/59 | Pressure transducers (Presductor ®, ASEA) | Knee extensors |
| Andersen and Henckel41 1987 Denmark | n=293; 16–19 years;W/M:165/128 | Strain gauge dynamometers | Knee extensors |
| AXIAL MUSCLES | |||
|---|---|---|---|
| Study and location | Participants(n; age; and sex) | Equipments or methods | Muscle groups |
| Paalanne et al.60 2009Finland | n=874; 19±0.2 years;W/M:493/381 | Computerized strain gauge dynamometer (New Test, Co., Oulu, Finland) | Trunk flexors/extensors and rotators |
| Danneskiold-Samsøe et al.35 2009 Denmark | n=174; 20–80 years;W/M:121/53 | Lido active (Lido Multi Joint II, Loredan Biomedical, Davis, CA, USA) | Trunk flexors/extensors |
| Cagnie et al.53 2007Belgium | n=96; 20–59 years;W/M:48/48 | Biodex isokinetic dynamometer | Neck flexors/extensors |
| Meldrum et al.30 2007Ireland | n=494; 19–76 years;W/M:259/235 | Quantitative muscle assessment system | Neck flexors |
| Hogrel et al.37 2007France | n=315; 20–80 years;W/M:168/147 | Quantitative muscle testing | Neck flexors |
| Salo et al.59 2006Finland | n=220; 20–59 years;W:220 | Specially designed measurement system | Neck flexors/extensors and rotators |
| aGarcés et al.56 2002Spain | n=94; 20->60 years;W/M:43/51 | Kin-Con ® computerized dynamometer | Neck flexors/extensors |
| Chiu et al.57 2002China | n=91; 20–84 years;W/M:46/45 | Multi cervical rehabilitation unit (Hanoun Medical Inc., Ontario, Canada) | Neck flexors/extensors; lateral flexors; protractors/retractors |
| Peolsson et al.54 2001Sweden | n=101; 25–63 years;W/M:50/51 | David back clinic 140 (DCB 140) | Neck flexors/extensors and lateral flexors |
| Beenakker et al.46 2001Netherlands | n=270; 4–16 years;W/M:131/139 | Hand-held dynamometer type CT 3001 (C.I.T. Technics, Groningen, The Netherlands) | Neck flexors |
| Stoll et al.36 2000Switzerland | n=543, 20–82 years;W/M:290/253 | Hand-held pull gauge | Neck flexors/extensors; trunk flexors and rotators |
| Phillips et al.44 2000Australia | n=200; 20–69 years;W/M:100/100 | Penny and Gileshand-held myometer (Penny & Giles Instrumentation Ltd., 4 Airfield Way, Christchurch, Dorset BH233TS, England) | Neck flexors |
| Jordan et al.58 1999Denmark | n=100; 20–70 years;W/M:50/50 | Strain-gauge dynamometer (Neck Exercise Unit, Norway) | Neck flexors/extensors |
| Vernon et al.55 1992Canada | n=40; 25±2 years;M:40 | Modified sphygmomanometer dynamometer(Magnatec Co. Ltd. Concord, Ontario, Canada) | Neck flexors/extensors; lateral flexors and rotators |
| Sunnegardh et al.47 1988 Sweden | n=124; 8–13 years;W/M:65/59 | Pressure transducers (Presductor ®, ASEA) | Trunk flexors/extensors |
| Andersen and Henckel41 1987 Denmark | n=193; 16–19 years;W/M:165/28 | Strain gauge dynamometer | Trunk flexors/extensors |
| Nordin et al.61 1987USA | n=101; 18–48 years;W:101 | Cybex II isokinetic dynamometer | Trunk flexors/extensors |
W: women; M: men; USA: United States of America.
Characteristics of the studies that established the reference values for isokinetic strength.
| Study and location | Participants (n; age; and sex) | Instrumentation | Muscular groups |
|---|---|---|---|
| Lundgren et al.64 2011Sweden | n=436; 6–12 years;W/M:190/246 | Computerized dynamometer (Biodex System 3®, Biodex Medical Systems, Inc., Shirley, NY, USA) | Knee flexors/extensors |
| Danneskiold-Samsøe et al.35 2009Denmark | n=174; 20–80 years;W/M:121/53 | Lido active (Lido Multi Joint II, Loredan Biomedical, Davis, CA, USA) | Shoulder, elbow, wrist, hip, knee and trunk flexors/extensors; shoulder and hip abductors/adductors, external/internal rotators; ankle dorsiflexors/plantarflexors |
| Holm et al.39 2008Norway | n=376; 7–12 years;W/M:191/185 | Cybex 6000 (Cybex-Lumex Inc, Ronkonkoma, NY,USA) | Knee flexors/extensors |
| aWiggin et al.65 2006USA | n=3587; 6–13 years;W/M: 2030/1557 | Biodex system II and III isokinetic dynamometers | Knee flexors/extensors |
| Frontera et al.62 1991EUA | n=200; 45–78 years;W/M:114/86 | Cybex II isokinetic dynamometer | Elbow and knee flexors/extensors |
| Sunnegardh et al.47 1988Sweden | n=124; 8–13 years;W/M:65/59 | Cybex II with a modified lever | Elbow flexors and knee flexors/extensors |
| Nordin et al.61 1987USA | n=101; Age: 18–48 years;W:101 | Cybex II isokinetic dynamometer | Trunk flexors/extensors |
| Ivey et al.63 1985USA | n=31; 21–50 years;W/M:13/18 | Cybex II isokinetic dynamometer | Shoulder flexors/extensors, abductors/adductors, external/internal rotators |
W: women; M: men; USA: United States of America.
Of the 46 included studies, 91.3% (n=42)16,17,22–61 reported reference values for isometric and 17.4% (n=8)35,39,47,61–65 for isokinetic strength, whereas 75.2%16,17,22–51 provided reference values for isometric strength of the upper limb muscles. For the evaluation of isometric strength, the most commonly employed equipment were portable dynamometers (52.3%)22–24,26–29,31,33,34,36,38,39,41–43,45,46,51,52,56,58 followed by isokinetic dynamometers (11.9%)32,35,40,53,61 and myometer (9.5%).16,17,25,44 Each of the other equipment or evaluation methods used to assess isometric strength was applied by a single study (Table 2).
In the majority of the studies (93.8%), the reference values for muscle strength were reported for both men and women. The references values for isometric strength were established for the majority of the appendicular and axial muscle groups of children (21.4%)17,22,23,25,31,39,46,47,52, adolescents (42.8%),16,17,22,23,25,28,31,39,41,42,45–48,51,52,60,61 adults (80.9%),16,22–24,26–28,30,32–38,40,42–45,48–61 and elderly (59.5%)16,22,23,27–30,32–38,40,43–45,49–52,56–58 (Table 2). The reference values for isokinetic strength were established for most appendicular and axial muscle groups of adults (50%)35,61–63 and elderly (25%)35,62 individuals. For the children, isokinetic strength values were only found for the following muscle groups: elbow flexors and knee flexors/extensors (50%).39,47,64,65 For the adolescents, the following muscle groups had their reference values described39,47,61,64,65 (Table 3): elbow flexors, knee flexors/extensors, and trunk flexors/extensors.
Meta-analysisAmong the 46 studies that established reference values for muscle strength, 13% (n=6)16,29,34,38,43,44 met the criteria established for synthesizing the values and performing the meta-analysis. All of these studies involved the evaluation of isometric strength. Considering that these criteria were similar, it was possible to synthesize the values of three pairs of studies, whose statistical analysis is given in Table 4. In two of these studies, the isometric strength of 10 muscle groups was evaluated, bilaterally (dominant and nondominant sides), in men and women of the following age groups: 50–59, 60–69, and 70–79 years34,38 (reference values of muscle strength ranged from 66.73±16.02 to 458.45±79.73N). In two other studies, the isometric strength of the hip flexors of the dominant side of men and women in the following age groups was evaluated: 20–29, 30–39, 40–49, 50–59, and 60–69 years16,44 (reference values of muscle strength ranged from 167±23.4 to 281.8±50.7N). Finally, two other studies evaluated the isometric strength of the handgrip muscles, as well as the lateral, palmar, and pulp-to-pulp pinches, bilaterally (right and left sides), in men and women in the 60–69 and 70–74 age groups29,43 (reference values of muscle strength ranged from 9.5±1 to 91.3±18.5 Pounds). The reference values for the muscle strength presented by the meta-analysis decreased with age for men and woman. Moreover, for the same age group, men tended to have a higher muscle strength than women and the dominant side tend to have a higher muscle strength than the nondominant side. See reference values in Table 4. As given in Table 4, the CV of the combined values ranged from 15% to 29.84% and 10.6% to 32.9% for men and women, respectively, and the most common values ranged from 20.1% to 30% (56.8% for men and 69.1% for women).
Discussion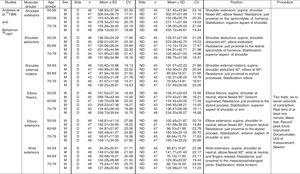
The present review described and evaluated the methodological quality of the studies, which established the reference strength values for the axial and appendicular muscles of healthy subjects. In addition, it also provided a synthesis with a descriptive meta-analysis of the previously established reference values. Most of the studies had adequate methodological quality, and reported the reference values for isometric strength of the upper limb muscles of adults and elderly of developed countries of the Northern Hemisphere, using portable dynamometers. For children and adolescents, the reference values for isometric strength of most muscle groups of the upper and lower limbs were reported. The meta-analysis synthesized the reference values of six studies, which were grouped into pairs, for 14 muscle groups of the upper and lower limbs of adults and elderly individuals of both sexes, using portable dynamometers and myometer. The CVs of the combined values of these studies ranged mainly from 20.1% to 30% and were also similar to those of the original studies.
Establishing criteria is also important to determine possible subgroups (e.g., age, sex, side) for reporting the results of the descriptive statistics of the reference values. Of the 46 included studies, only 17.4% (n=8) justified the subgroups, while reporting the results of the descriptive statistics,23,25,31,33,34,38,53,62 of which 62.5% (n=5) did not clearly justify the reasons to support the applied criteria.25,31,33,53,62 Between-group comparisons,23,25,33,34,53,62 correlations,34,38 and regression25,31,34,38 were the types of statistical analyses used to justify the subgroup divisions.
Regarding the age subgroups, most of the studies, which established reference strength values for children and adolescents, reported their subgroup results in 1-year intervals.25,28,31,39,41,46,64,65 This is probably justified by the rapid changes in the development of these subjects. For adults and elderly, the results for the subgroups were described per decades.16,23,27,30,32,34,35,38,40,44,52–54,58,59,62 Pessoa et al.,67 in a systematic review with meta-analysis for the reference strength values of the inspiratory muscles in adults and elderly, reported the age subgroup results per decade.67 On the other hand, Bohannon et al.,68 in their systematic review with meta-analysis for the reference values of handgrip strength for the same population, provided the subgroup results in 5-year intervals.68 Perhaps, the definition of age subgroups in these two previous meta-analyses67,68 followed the definition adopted by the majority of the studies, which were included in the reviews. As the population groups were similar (adults and elderly) between the two reviews67,68 associated with the results of the present study, it is possible to conclude that there is no clear criterion, neither a consensus regarding the age range to group the subjects, when reporting reference values of muscle strength.
The lack of description and differences in methods and evaluation procedures limited the number of studies included in the present meta-analysis, i.e., only six out of 46 studies (13%). Among the 41 evaluated muscle groups, only 14 (34.1%) had their results synthesized in the meta-analysis. In addition, only the hip flexor muscle group of the dominant side was evaluated in two pairs of studies, one that employed a portable dynamometer34,38 and the other a myometer,16,44 and both evaluated isometric strength. Data from four16,34,38,44 of the six studies, which were included in the meta-analysis, could have been grouped, if the adopted procedures were similar. Similar results were found in two previous systematic reviews with meta-analysis of inspiratory67 and handgrip68 muscle strength, i.e., differences in methods and evaluation procedures also limited the number of the included studies.67,68
The CVs were similar to those calculated with the descriptive statistics reported by all of the studies, except for values related to the hip flexor muscles of the nondominant side reported by the studies of Backman et al.16 and Phillips et al.44: the CVs of the present meta-analysis ranged from 14% (see Table 4, CV=23.4/167) to 23.7% (see Table 4, CV=64.1/270.1), whereas those reported by Backman et al.16 and Phillips et al.44 ranged from 10.9% (CV=20/183) to 26% (CV=84/323) and 6.6% (CV=16/241) to 13.5% (CV=25/185), respectively. In general, these results indicate adequacy of reference values reported in the present meta-analysis, since they are mostly similar to those of the original studies.
The reference values for muscle strength have already been established for subjects from developed countries, most of them from the Northern Hemisphere, who have specific ethnic characteristics, which may interfere with strength measures, such as body fat mass and muscle mass indices, height, and weight.76 The possible differences in strength among ethnic groups77 confirm the importance of determining reference values for population groups, who have specific demographic characteristics. For professionals on developing countries, no information is available on the reference strength values for the appendicular and axial muscles. Therefore, the interpretations of the evaluation of strength and, consequently, the clinical decision-making within clinical settings are limited. In addition, specifically for children and adolescents, the reference values for the following muscles groups have not been established: shoulder and hip external/internal rotators, shoulder adductors, neck and trunk lateral flexors, and lateral rotators.
This systematic review with meta-analysis has both strengths and limitations that need to be considered. First, the electronic searches were conducted in only three databases (MEDLINE, LILACS, and SciELO), which may have prevented the inclusion of some relevant studies. Considering that the MEDLINE database is one of the most complete bibliographic databases78 of biomedical literature records79; that LILACS and SciELO databases also comprise articles published in Portuguese or Spanish that may not be found at MEDLINE; and that the reference list of the included articles was screened to identify further ones, it can be considered that a comprehensive systematic review was performed. A strength of this study is the analysis of the methodological quality of the studies and the comparison of the CV of the results of the meta-analysis with the CV of the original studies. In addition, another strength of this systematic review is the applicability of the results for the measurement of different muscle groups.
In conclusion, the studies, that reported reference values of strength for the appendicular and axial muscles, showed, in general, adequate methodological quality and provided both isometric and isokinetic measures for all age groups, mainly adults and elderly. Establishing the reference values is still necessary for other muscle groups of children and adolescents and other methods of evaluation, such as the MST, whose data are scarce. Furthermore, no study was found that provided reference values of strength of the axial and appendicular muscles of people from developing and undeveloped countries. The present meta-analysis provided normative data for the isometric strength of 14 appendicular muscle groups of the dominant and nondominant sides of both men and women, aged 20–79 years. It is necessary to adapt the procedures and methods for the evaluation of reference values in future studies to carry out a more comprehensive meta-analysis including children and adolescents and some muscle groups for adults and the elderly. In general, the CV values that resulted from the meta-analysis were similar to those reported by the original studies. This indicates adequacy of reference values reported in the present meta-analysis. These data may be used to interpret the results of the evaluations and establish appropriate treatment goals.
Conflicts of interestThe authors report no conflict of interest.
Financial support for this research was provided by CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior), FAPEMIG (Fundação de Amparo à Pesquisa do Estado de Minas Gerais), CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico) and PRPq/UFMG (Pró-reitoria de Pesquisa da Universidade Federal de Minas Gerais).



