
Evidence shows that lack of physical activity and sedentary time are associated with higher prevalence of low back pain (LBP).
ObjectiveTo investigate the association between replacing sedentary time and light physical activity with a higher physical activity level with the prevalence of LBP.
MethodsTwo hundred and sixty-six individuals from a city in southeastern Brazil were recruited to this cross-sectional study. Sedentary behavior and physical activity level were evaluated using an ActiGraph GT3X tri-axial accelerometer during 7 days. The prevalence of LBP was assessed using the Nordic questionnaire. Isotemporal substitution using logistic regression analyses were performed to investigate the association between replacing an activity with another in the prevalence of LBP.
ResultsReplacing time spent in sedentary behavior with moderate physical activity slightly reduced the prevalence of LBP (odds ratio [OR]= 0.97; 95% CI: 0.95, 0.98). In addition, replacing time spent in light physical activity with moderate physical activity also slightly reduced the prevalence of LBP (OR= 0.97; 95% CI: 0.95, 0.98). There was no association for replacing sedentary time and light or moderate physical activity with vigorous physical activity on the prevalence of LBP.
ConclusionsThe results suggest a small protective effect for LBP when replacing time in sedentary activities or light physical activity with moderate physical activity.
Low back pain (LBP) is the leading cause of years lived with disability in 126 out of 195 countries and territories included in the Global Burden of Disease in 2017.1 The direct costs related to LBP is of major consequences to the health care systems. In the United States, back pain was the leading condition in the ranking of health care spending, totaling $134.5 billion in 2016.2 In Brazil, $71.4 millions were spent on LBP in 2017, with a substantial proportion being attributable to spinal imaging.3 Most episodes of LBP (90%) are classified as non-specific LBP, that is when the pain cannot be attributed to a spinal pathology or nerve root dysfunction associated with a lumbar disc herniation.4 Therefore, identifying factors related to the prevalence of this condition may help developing new interventions and prevention strategies.
Evidence shows that physical activity and sedentary time are likely associated with the prevalence of LBP.5,6 While physical activity is defined as any bodily movement generating an energy expenditure,7 sedentary time is defined as any waking activity performed in lying, reclining, or sitting positions that expends less than 1.5 METs.8 These two behaviours have similar mechanisms to explain the prevalence of LBP, but with opposite directions. One explanation is that physical inactivity9 or increased times spent in sedentary activities10 may increase the production of pro-inflammatory cytokines, which are associated with a LBP episode.11 However, most studies investigate the role of physical activity and sedentary time in the prevalence of LBP separately, and their interaction on the prevalence of LBP remains unclear.
The isotemporal substitution analysis is an innovative approach which aims to understand the influence of substituting sedentary behavior with physical activity on a particular outcome.12
In people with musculoskeletal pain, replacing 10 minutes of sedentary behavior with 10 minutes of physical activity may decrease the chances of having musculoskeletal pain by 23%.13 Another study found that replacing sedentary time with vigorous physical activity is associated with a reduction in pain intensity in people already having chronic LBP.14 To our knowledge, no study has been conducted investigating the interaction of sedentary time and physical activity specifically in the prevalence of LBP. Therefore, the primary objective of this study was to investigate the effect of replacing sedentary time with physical activity on the prevalence of LBP. We also aimed to investigate the influence of replacing different physical activity intensities (i.e., light, moderate, and vigorous physical activity) with another intensity on the prevalence of LBP. Understanding the factors associated with the prevalence of LBP can help develop future interventions and prevention strategies.
MethodsStudy designThis is a cross-sectional study in a sample stratified by census sector in the city of Santo Anastácio located in Sao Paulo state, Brazil. The study design was based on the National Health Survey15 and the protocol of this study was described in a previous publication and registered in the ClinicalTrials.gov (register number: NCT03986879).16 The study was approved by the Ethics Research Committee of the Sao Paulo State University (UNESP), under the protocol CAAE: 72191717.9.0000.5402.
SampleThe recruitment of the participant targeted adults aged 18 years or older, in the city of Santo Anastácio-SP. The adult population of Santo Anastácio is approximately 16,000 inhabitants, according to the Brazilian Institute of Geography and Statistics. The sectors were divided based on a geographic map of the city. All neighborhoods, streets, and houses were registered to calculate the number of people to interview. Then, they were randomly selected using the SPSS “random” function. All residents of the randomly selected houses with or without LBP were considered eligible. However, we excluded individuals who required any assistance to move (e.g., using a wheelchair) or who were restricted to bed, unable to understand Portuguese, and did not use the accelerometer for the minimum required wear time.
The sample size calculation, based on 80% power, 5% alpha, and a correlation value of r=0.23, determined a minimum sample of 147 participants.17 However, anticipating that 30% of the participants could refuse to participate in the study and including 10 individuals for each event used (i.e., LBP, age, sex, and socioeconomic status), we estimated that 232 participants would be required for this study.
ProceduresParticipants were informed about the study's objective and those who accepted to participate were invited to voluntarily sign the consent form. Face-to-face interviews were conducted with participants using an electronic instrument (tablet), using the REDCap platform. After the interview, each participant were provided with a tri-axial accelerometer after receiving detailed instructions to its use.18
InstrumentsAnthropometric and sociodemographic data as well as the prevalence of LBP were initially collected from participants. Before the beginning of the data collection, all assessors received training to familiarize themselves with the administration of the questionnaires and the instructions to use the accelerometer. All instruments and measurements for this study are described below:
Anthropometric data: Body mass was measured using a digital scale (Plenna, Brazil) and height was measured using a stadiometer. Body mass index (BMI) was calculated and participants having a BMI less than 24.99 kg/m2 were classified as being normal weight, those from 25.00 kg/m2 to 29.99 kg/m2 were classified as overweight, and those greater than 30 kg/m2 were classified as obese.
Socioeconomic level: The “Brazilian Economic Classification Criteria”, established in 2014 by the Brazilian Association of Research Companies, were used to assess the socioeconomic level of participants. The questionnaire classifies the economic condition considering the education level, number of rooms in the house, and household items. The following classification was adopted: A1 and B1 high socioeconomic status; B2, C1, and C2 middle socioeconomic status; D and E low socioeconomic status.
Prevalence of low back pain: the Brazilian version of the Nordic Musculoskeletal Questionnaire was used to determine the prevalence of LBP.19 Participants were asked to look at a body image on the screen and indicate whether they experienced pain, discomfort, or numbness in any body segment. We administered the questionnaire once at baseline and patients reporting pain in the lower back region in the past six months were considered as having LBP. This instrument is reliable, valid, and considered easy to understand and interpret.19
Physical activity levels and sedentary time objectively measured: the ActiGraph GT3X tri-axial accelerometer (ActiGraph, LLC, Pensacola, FL, USA) was used to collect objective measures of physical activity and sedentary time. The ActiGraph is a portable device (4.6×3.3×1.5cm, 19g) able to record movements in three orthogonal planes: vertical, horizontal anteroposterior, and horizontal mediolateral. The ActiGraph data were processed using 60 second epoch and 30Hz acceleration.
Participants were instructed to use the accelerometer attached to the right hip while they were awake for 7 consecutive days, removing it only to sleep or to perform any water-based activities. We measured the activity level during a week to quantify their typical physical activity levels. No intervention was provided during this week and participants were instructed to keep their regular activities. Data were considered valid when the participant used the accelerometer at least 10 hours per day for at least four days.18,20 A non-wear period was defined as an interruption of activity from 0 to 100 counts/minute for at least two consecutive minutes.21 Consecutive hours of zero counts and days with less than 10 hours of monitoring were excluded from the data analysis. The accelerometer-derived measures of physical activity, in minutes per week, were time doing: light physical activity; moderate physical activity, vigorous physical activity, sedentary behavior. The following cut-offs were used in this study: sedentary time (below 100 counts/minute); light physical activity (101 to 2019 counts); moderate physical activity (2020 to 5998 counts); vigorous physical activity (5999 counts or more).18 Actilife 6 software (ActiGraph, LLC, Pensacola, FL, USA) was used for data processing.
Data analysisDescriptive statistics were calculated to obtain mean (standard deviation) for data with normal distribution and median (interquartile range) for data with non-normal distribution. Categorical and dichotomous variables were reported using frequency (percentage).
The isotemporal substitution analysis was performed consistent with previous studies.12,22 A multivariable logistic regression analysis was performed to understand the association between replacing 60 min per week at a specific activity level with 60 min per week with another activity level with the prevalence of LBP as the outcome of interest. In our study, the isotemporal substitution analysis focused on replacing sedentary time with light, moderate, or vigorous physical activity. Therefore, we included in the model light, moderate, or vigorous physical activity, and the total wear time (i.e. sedentary behavior + light, moderate, and vigorous physical activity) as independent variables. The coefficient of the physical activity intensities was the result of replacing sedentary time with a similar time in light, moderate, or vigorous physical activity. The prevalence of LBP was included as a dependent variable and sex, age, and socioeconomic level as covariables. In the secondary analyses, we maintained the time in sedentary behavior, but removed time spent in a specific physical activity intensity to quantify its influence on the prevalence of LBP. All analyses were performed using SPSS version 22.0 software and the statistical significance level was set at 0.05.
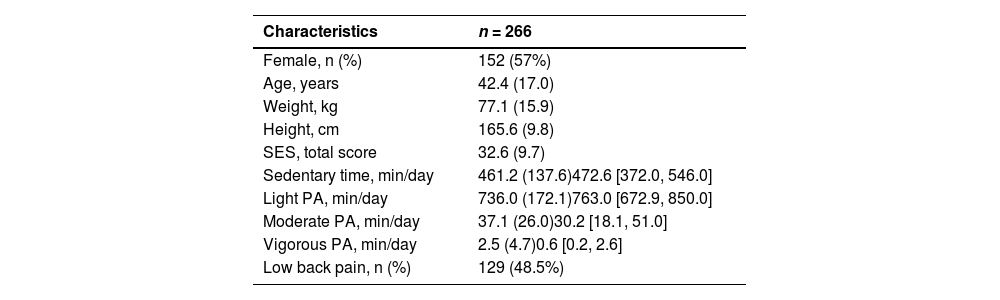
ResultsFrom December/2018 to June/2019, 306 participants agreed to participate. Of the initial 306 participants, 15 were excluded due to accelerometer misuse, 22 did not complete all the assessments, and three were excluded due to assessment error. Therefore, 266 individuals were considered eligible for this study. There were no technical issues and errors during the data collection, except for those who did not comply with the use of the accelerometer. There were also no adverse effects reported by the participants during the data collection. The average age was 42.4 (SD 17.0) years and most participants were female (57%). The mean time spent in sedentary behavior was 461.2 (SD 137.6) min/day and nearly half (48.5%) of participants reported having an episode of LBP in the past 6 months (Table 1).
Sample characteristics.
Values are mean (standard deviation) and median [interquartile range] unless otherwise specified. Abbreviations: SES, socioeconomic status; PA, physical activity.
SES score: the higher the score, the higher the socioeconomic status. Score variation: 0- 93 points.
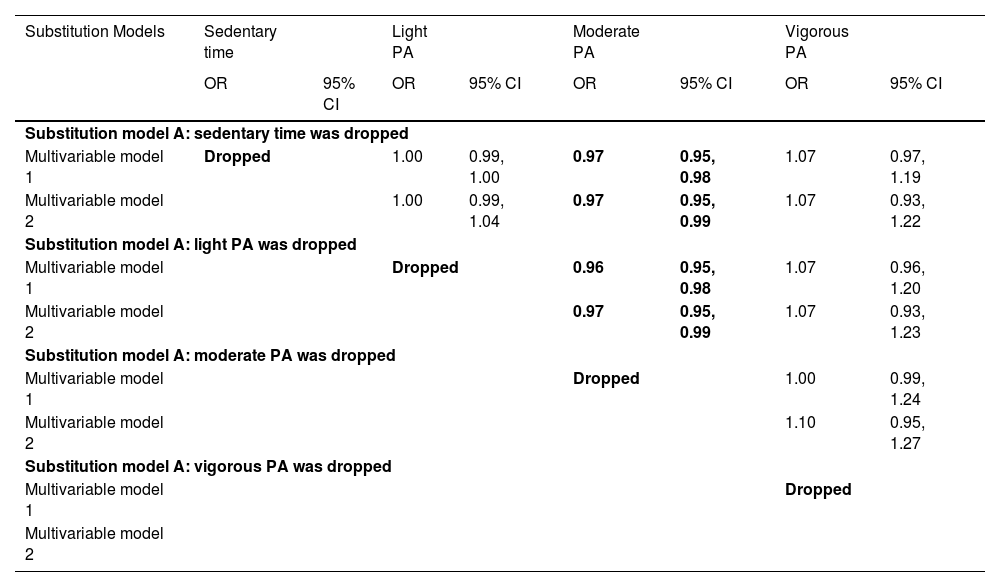
Table 2 shows the results of the association between the isotemporal substitution of sedentary behavior with physical activity and the prevalence of LBP. Replacing sedentary time with moderate physical activity resulted in slightly lower chances of reporting LBP (odds ratio [OR]adjusted= 0.97; 95% CI: 0.95, 0.99). The substitution of sedentary time with moderate physical activity was associated with 3% less chances of reporting LBP. In contrast, replacing sedentary time with light physical or vigorous physical activity was not associated with the prevalence of LBP. In the secondary analysis, replacing light physical activity with moderate physical activity, without reducing sedentary time, was associated with lower chances of reporting LBP (ORadjusted= 0.97; 95% CI: 0.95, 0.98). Similarly, replacing light physical activity with moderate physical activity, without reducing sedentary time, was associated with a 3% decrease in reporting LBP.
Association between the isotemporal substitution analysis of sedentary behavior with Moderate PA, Vigorous PA, and Light PA and the prevalence of low back pain
Abbreviations: PA, physical activity; OR, odds ratio; CI, confidence interval
Multivariable model 1: Not adjusted
Multivariable model 2: Adjusted for sex, age, and socioeconomic level
Our findings showed that replacing 60 min of sedentary time or 60 min of light physical activity per week with 60 min of moderate physical activity per week may reduce the prevalence of LBP. Although the effect was small, these two substitutions resulted in a protective factor for LBP. However, replacing sedentary time or light or moderate physical activity with vigorous physical activity was not associated with a change in prevalence of LBP.
Our findings align with the results of previous studies investigating the isotemporal substitution in different outcomes. Ryan et al.13 also found that replacing 10 minutes of sedentary behavior per day with 10 minutes of moderate physical activity per day was associated with the prevalence of musculoskeletal pain. The substitution reduced the risk of having LBP by 11%. Similar to our study, substituting sedentary time for light physical activity did not change the prevalence of musculoskeletal pain. A recent study14 also found that replacing sedentary time as well as light or moderate physical activity with 60 minutes of vigorous activity per week was significantly associated with reductions in pain intensity (1.5 out of 10 points) in people already having chronic LBP. Our findings also align with findings of individual studies investigating the influence of sedentary behaviour and physical activity in the prevalence of LBP.23,24 These findings imply that not only replacing sedentary behaviour with physical activity, but also replacing light physical activity with more intense physical activity, may play a role in the prevalence of LBP.
There are some explanations to our findings. One of them is the physiological consequences of practicing physical activity which activates endogenous inhibitory systems reducing serotonin transporter expression and increasing serotonin levels, and opioids which may reduce the prevalence of pain.25 The sedentary time of our sample may be considered high, similar to what has been reported by previous studies on the Brazilian population.26 Previous studies have shown that sedentary behavior reduces the cross-sectional area of muscle fibers and decreases the oxidative capacity and blood supply of the paraspinal muscles which can increase the chances of having spinal pain.27 However, evidence confirming the sedentary behaviour as a risk factor of LBP is inconsistent.28
Another co-shared mechanism is related to the concentration of pro-inflammatory cytokines. Previous studies showed that replacing sedentary time with moderate physical activity modulates the inflammatory status.29 The concentration of pro-inflammatory cytokines is also associated with higher chances of having LBP.11 Therefore, our findings strengthen the evidence that moderate physical activity is a protective factor in the development of LBP. Another factor to be considered is that physical activities of moderate intensity could be linked to spinal muscles strengthening and, consequently, greater postural stability. This type of intensity linked to postural exercises could strengthen the transversus abdominis and multifidus, reducing episodes of LBP.30
This study has some limitations. The study has a cross-sectional design and our findings do not imply cause and effect. Therefore, longitudinal studies investigating isotemporal substitution of sedentary behavior by physical activity are warranted. Another limitation is related to the use of the accelerometer to determine sedentary behavior, because of the limitation in distinguishing sitting/lying position to the standing position. However, previous studies showed that the accelerometer is a valid method to assess sedentary behaviour.31 Finally, we focused on the prevalence of LBP in adults as the dependent variable which restrict the generalizability of our findings. Therefore, our findings should not be generalizable to specific symptoms duration (e.g., chronic LBP) or other age groups. In fact, recent studies showed that sedentary activities may be involved in the prevalence and incidence of LBP in adolescents.23,24 Therefore, future studies should investigate the importance of the isotemporal substitution of sedentary behaviour by physical activity in adolescents. However, the current study has some strengths which includes the recruitment of a representative sample using probabilistic methods and the use of an objective method to quantify sedentary behavior and physical activity levels. The use of direct measurement of physical activity assessment decreases possible memory biases linked to different intensities of physical activity.32
Our study highlights the importance of encouraging the practice of moderate physical activity to reduce the risk of having LBP. Evidence on interventions to prevent LBP is scarce. Although a previous review showed that exercise may be effective to prevent LBP,33 these interventions mainly focus on increasing any type of physical activity levels. Therefore, future interventions should include strategies to promote moderate to vigorous physical activity combined with education and advice to reduce sedentary time.34 Future trials should also test interventions that promote physical activity but at the same time reduce time spent in sedentary behaviour and the consequences to prevent LBP.
ConclusionReplacing sedentary time or light physical activity with moderate physical activity has a small protective effect on the prevalence of LBP. There was no association when replacing sedentary time or light physical activity with vigorous physical activity in the prevalence of LBP. Future studies should investigate if these substitutions may prevent an episode of LBP.
This study was supported by Sao Paulo Research Foundation (FAPESP/grant number: 2017/07231-9). DGDC holds a Productivity Fellowship from the National Council for Scientific and Technological Development (CNPQ) (Grant number: 305886/2022-3).



