
Pectoralis minor muscle length is believed to play an important role in shoulder pain and dysfunction. Current clinical procedures for assessing pectoralis minor muscle length may not provide the most useful information for clinical decision making.
ObjectiveTo establish the reliability and construct validity of a novel technique to measure pectoralis minor muscle length under actively and passively lengthened conditions.
DesignCross-sectional repeated measures.
MethodsThirty-four healthy adults (age: 23.9, SD=1.6 years; 18 females) participated in this study. Pectoralis minor muscle length was measured on the dominant arm in three length conditions: resting, actively lengthened, and passively lengthened. Based upon availability, two raters, out of a pool of five, used a caliper to measure the distance between the coracoid process and the 4th rib. The average of two pectoralis minor muscle length measures was used for all muscle length conditions and analyses. Intraclass correlation coefficients determined intra-and inter-rater reliability, and measurement error was determined via standard error of measurement and minimal detectable change. Construct validity was assessed by ANOVA to determine differences in muscle length across the three conditions.
ResultsOur intra- and inter-rater reliability values across all three conditions ranged from 0.84 to 0.92 and from 0.80 to 0.90, respectively. Significant differences (p<0.001) in muscle length were found among all three conditions: rest-active (3.66; SD=1.36cm), rest-passive (4.72, SD=1.41cm), and active-passive (1.06, SD=0.47cm).
ConclusionsThe techniques described in this study for measuring pectoralis minor muscle length under resting and actively and passively lengthened conditions have acceptable reliability for clinical decision making.
Shoulder pain has been reported to affect up to 67% of the general population across the lifetime.1 Rotator cuff disease is the most common cause of shoulder pain, interferes with work and functional related activities, and has a negative impact on health-related quality of life.2–7
The alignment–impairment model has been proposed as a way to understand how multiple factors contribute to the development of shoulder pain and dysfunction.8,9 This model describes how alignment deviations give rise to structural alterations, which then lead to pathomechanical alterations and development of shoulder pain. The model proposes that several factors contribute to resting scapular alignment, including the thoracic spine, shoulder girdle musculature, and tissue flexibility. Persistent postures and repetitive activities that place the shoulder in a protracted position are believed to result in adaptive muscle shortening, which may contribute to malalignment, pain, and ultimately movement dysfunction.8–10 Collectively, these impairments are believed to lead to development of shoulder pain and dysfunction.8,11–15
The pectoralis minor muscle is believed to play an important role in shoulder girdle alignment and movement.16 The relationship between resting pectoralis minor muscle length and scapulothoracic movement has been studied in a healthy, young population.11,12,17 Individuals with shorter resting pectoralis minor muscle length have been shown to have reduced scapular upward rotation and scapular posterior tilting during humeral elevation.11 The significance of this information is that these motion patterns are similar to those reported in individuals with shoulder pain secondary to subacromial impingement,14 rotator cuff disease, and glenohumeral instability.18,19 Based on this, clinical assessment of resting scapular alignment and pectoralis minor muscle length is widely performed as part of a physical therapy examination for individuals with shoulder pain and dysfunction.16
While resting pectoralis minor muscle length appears to provide potentially useful information about scapular alignment and scapulothoracic motion, it does not provide all of the necessary information for determining how much the muscle can lengthen (muscle extensibility). In light of the fact that a modeling study has shown that the pectoralis minor muscle elongates up to 67% of its initial length during overhead arm motions,20 information about pectoralis minor muscle extensibility could provide further clinical insight into the influence of this muscle on scapulothoracic motion.9,10,21 However, determining pectoralis minor muscle extensibility requires a valid and reliable method for measuring pectoralis minor muscle length when the muscle is in a lengthened position.
Therefore, the purposes of this study were to establish the rater reliability and construct validity of our technique for measuring pectoralis minor muscle length under actively and passively lengthened conditions. It was hypothesized that our proposed technique would demonstrate good relative and absolute reliability and result in a significant increase in pectoralis minor muscle length as compared to the resting length, thereby establishing the validity of the technique. These measures of pectoralis minor muscle length were then used to determine pectoralis minor muscle extensibility.
MethodsStudy designA cross-sectional, repeated-measures design was employed.
ParticipantsParticipants were recruited from a university campus by personal contact and advertisements. Individuals were eligible to participate if they were between 18 and 35 years of age, free of current shoulder pain, and able to elevate their arms at least 130°. Individuals were excluded from participating if they self-reported any of the following: previously diagnosed scoliosis; a current episode of cervical or lumbar spine pain; shoulder, elbow, forearm, wrist, or hand pain; brachial plexus injury; or nerve palsy affecting the shoulder girdle or upper extremity. Thirty-five participants (female=18) met the criteria and were enrolled in the study.
Ethical approval statementAll participants signed an informed consent, approved by the Drexel University Institutional Review Board (Protocol # 1408003050), Philadelphia, PA, USA, prior to beginning study procedures.
RatersFive raters (two licensed physical therapists and three final year physical therapy students) underwent an approximately 90-min measurement procedure training session. This session consisted of reviewing the measurement procedures and having each rater practice on one another until all raters felt comfortable performing all measurements. Rater selection for all participant measurement sessions was based upon rater availability. All raters contributed to data collection sessions, and an attempt was made to balance the number of measurement sessions among raters.
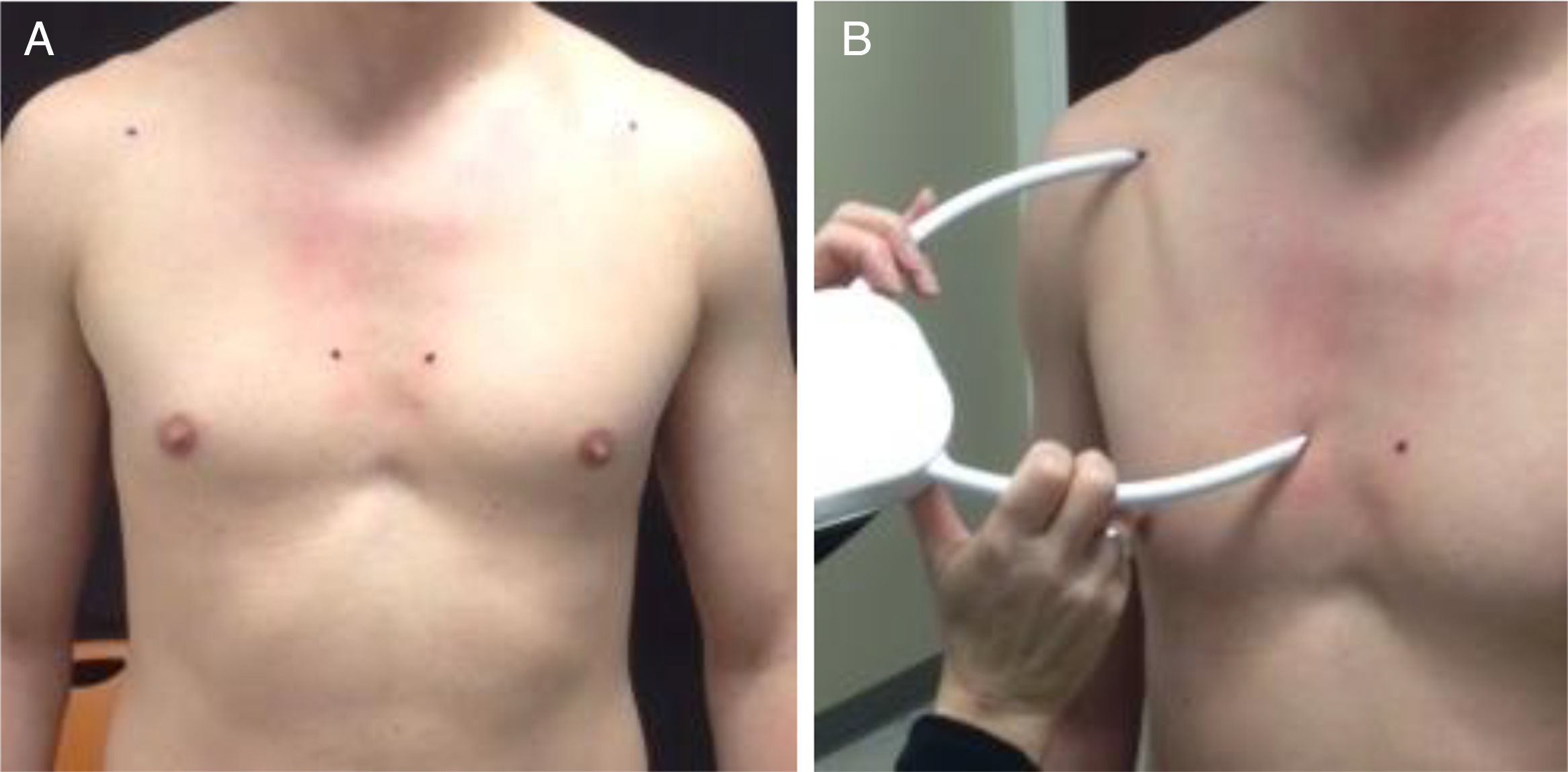
Study proceduresPectoralis minor muscle lengthPectoralis minor muscle length was defined as the distance between two bony landmarks: the coracoid process and the inferior medial aspect of the 4th rib adjacent to the sternocostal junction. Initial landmark identification occurred with the participant supine where the landmarks were palpated and marked with a dark marker. Landmark location was reassessed while the participant stood in their natural relaxed posture and any necessary adjustments in landmark location were made (Fig. 1A). In an attempt to minimize the influence of anterior chest wall soft tissue mass on pectoralis minor muscle length measures, we used a caliper (palpation meter – PALM) rather than a tape measure. To prevent bias and to mask the rater, for all measures the PALM was placed with the meter facing away from the rater. A second examiner read the caliper dial, recorded the length measurement, and returned the caliper to the zero position. All measurements were repeated twice. Following the standard procedure for obtaining pectoralis minor muscle length in our clinic, if these measures differed by more than 0.50cm, the measure was repeated until two measures were within 0.50cm of one another. These two measures were then averaged, and the averaged value was used for all subsequent analyses.
 Identification of anatomical landmarks (4th rib and coracoid process); (B) caliper (PALM) measurement of pectoralis minor muscle length in resting position.")
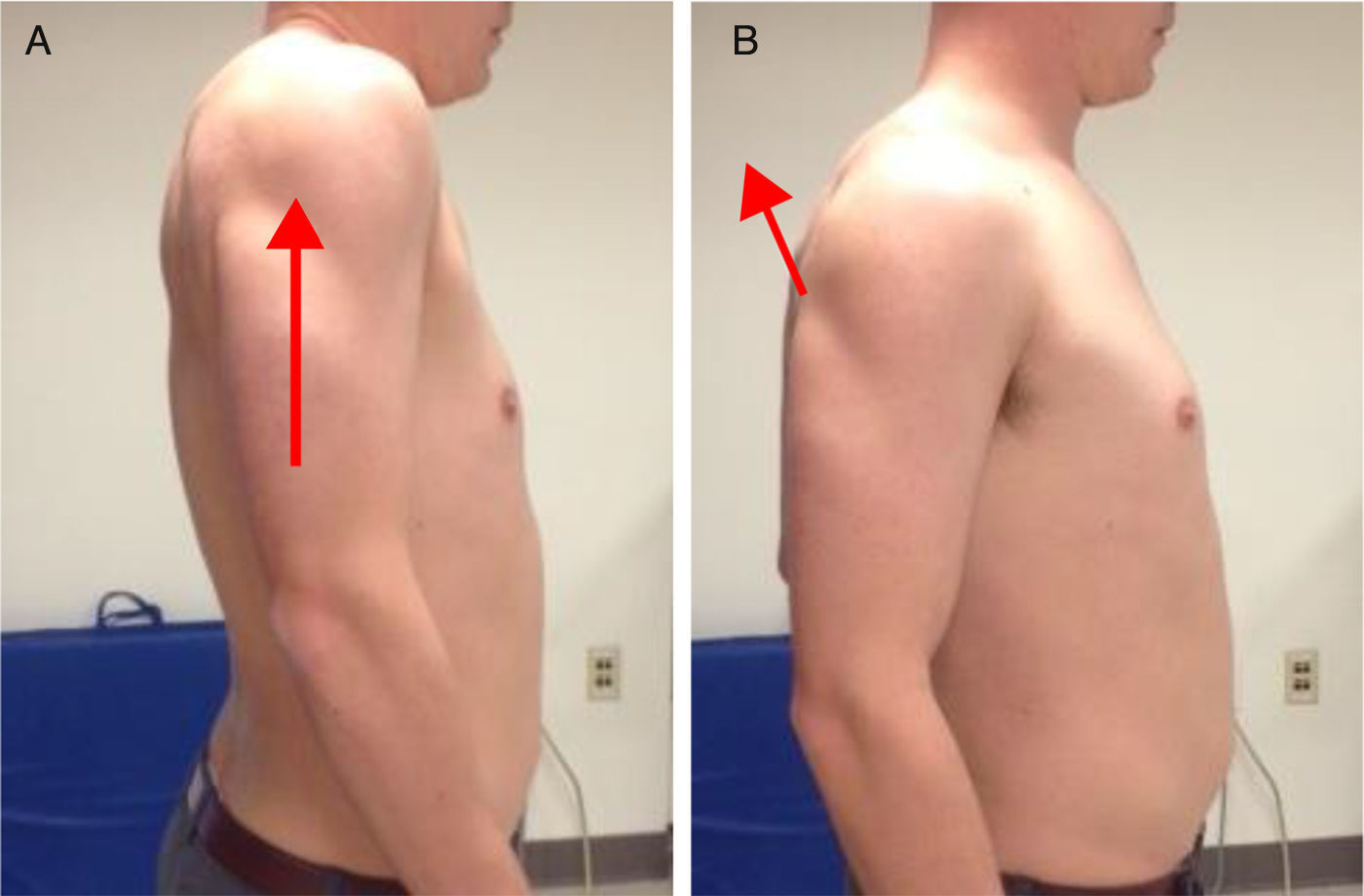
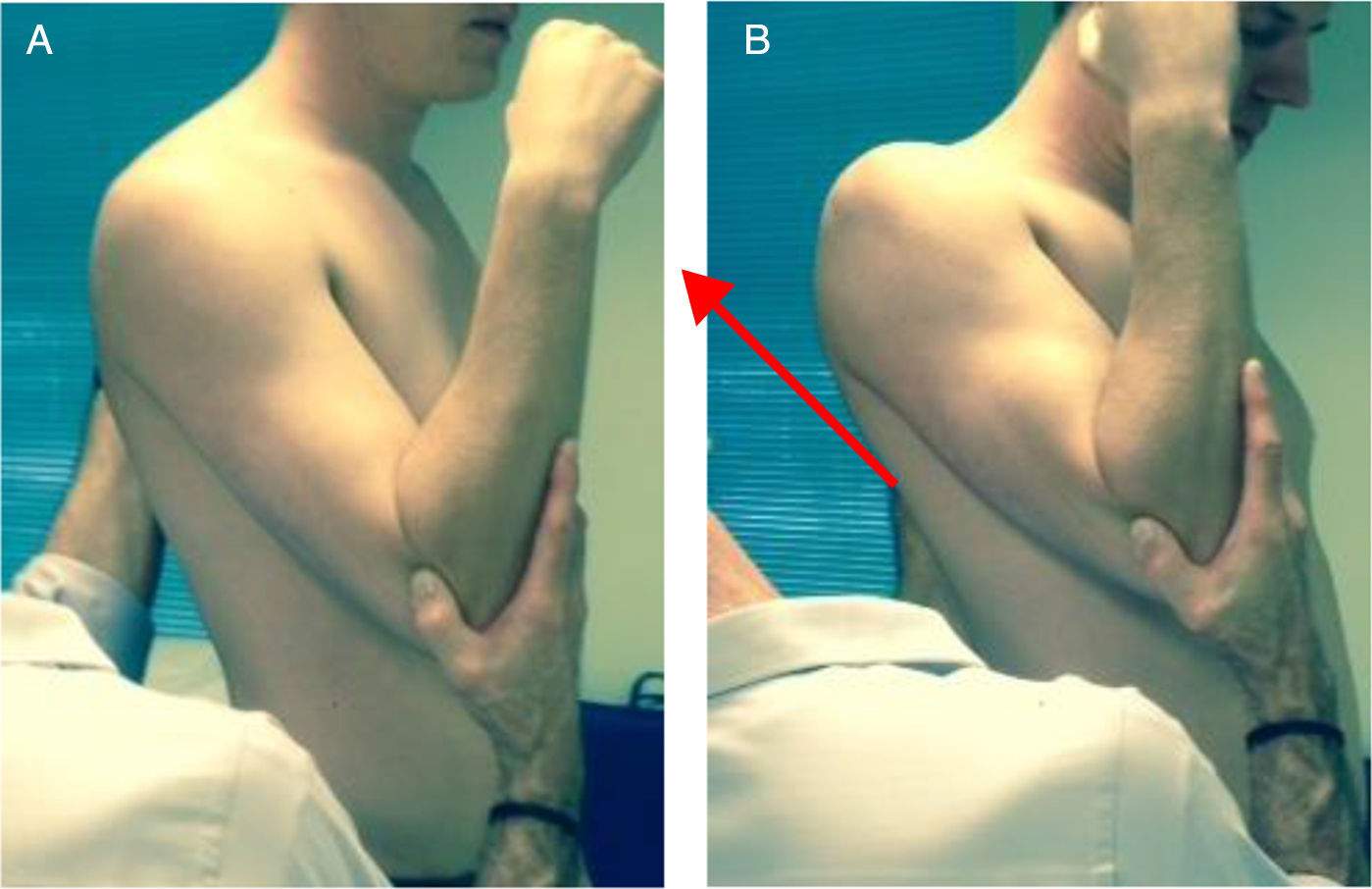
Resting pectoralis minor muscle length was measured while participants stood in their relaxed natural posture (Fig. 1B). Following resting measures, pectoralis minor muscle length was measured during actively and passively lengthened conditions, with order randomly determined. Bony landmarks were re-palpated and re-marked for measures taken in the lengthened conditions. The actively lengthened condition required participants to maximally elevate and retract their scapula (Fig. 2). For the passively lengthened condition, participants’ arms were placed in approximately 30° of flexion. While stabilizing the participant's trunk, a clinician used the distal end of the participant's humerus to push their shoulder in a superior/posterior direction until firm tissue resistance was encountered (Fig. 3). Our lengthening techniques were based upon a cadaveric study by Muraki et al. that investigated appropriate stretching techniques for the pectoralis minor muscle.22
 Maximal scapular elevation; (B) maximal scapular adduction.")
 Starting position of 30° humeral flexion; (B) superior/posterior translational force by examiner.")
Inter-rater reliability of pectoralis minor muscle length measures for all three conditions (resting, actively lengthened, and passively lengthened) was determined by independent measures performed by two raters. Once raters were identified, the order in which they took measurements was randomly determined. After the first rater completed their measurements, markings were removed with an alcohol swab and the second rater completed their measurements.
Intra-rater reliability was determined from a random subset of 20 participants. Once again, based upon availability, one rater was asked to take a second set of measures on this subset of participants at the end of the data collection session. As noted above, an alcohol swab was used to remove all markings between the measurements used for establishing intra-rater reliability.
AnalysesRater reliabilityIntraclass correlation coefficients (ICC) were used to determine relative inter- and intra-rater reliability of pectoralis minor muscle length measures for each muscle length condition. Specifically, the ICC(2,2) model was used to determine inter-rater reliability, while the ICC(3,2) model was used to determine intra-rater reliability.23 For the purposes of our study, intra- and inter-rater reliability were defined as excellent (ICC>0.80), good (ICC=0.61–0.80), and fair (ICC=0.41–0.60).23 Absolute reliability, which provides information related to measurement error, was determined by the standard error of the measurement (SEM) and minimal detectable change (MDC95) for inter- and intra-rater and each pectoralis minor muscle length condition.
Construct validityA one-way repeated measure ANOVA determined if differences in pectoralis minor muscle length existed among the resting, actively lengthened, and passively lengthened conditions. Bonferroni post hoc analyses were used to determine specific pairwise differences while controlling for Type I error. The level of significance was set at 0.05.
Pectoralis minor muscle extensibilityPectoralis minor muscle extensibility was determined from the active and passive length conditions as follows: active condition=[(active length−resting length)/resting length]*100, and passive condition=[(passive length−resting length)/resting length]*100.
ResultsThirty-five individuals participated in the study. However, data from one participant was omitted due to a pectoralis minor muscle length recording error. Data from the dominant arm of 34 participants were included in the analysis (mean age=23.9, SD=1.6 years, height=168.9, SD=1.6 8.9cm, weight=68.1, SD=1.6 14.1kg, right hand dominance=30).
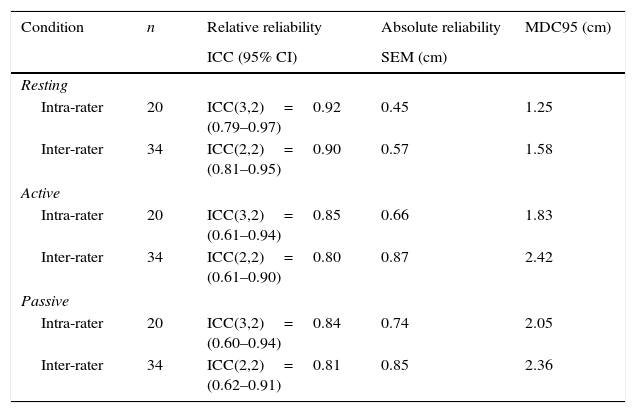
Rater reliabilityThe ICC, SEM, and MDC95 for our intra-rater measurements range from 0.84 to 0.92, 0.45 to 0.74cm, and 1.85 to 2.05cm, respectively. The ICC, SEM, and MDC95 for our inter-rater measurements range from 0.80 to 0.90, 0.57 to 0.87cm, 1.58 to 2.42cm, respectively (Table 1).
Relative and absolute reliability for pectoralis minor muscle length-3 conditions.
| Condition | n | Relative reliability | Absolute reliability | MDC95 (cm) |
|---|---|---|---|---|
| ICC (95% CI) | SEM (cm) | |||
| Resting | ||||
| Intra-rater | 20 | ICC(3,2)=0.92 (0.79–0.97) | 0.45 | 1.25 |
| Inter-rater | 34 | ICC(2,2)=0.90 (0.81–0.95) | 0.57 | 1.58 |
| Active | ||||
| Intra-rater | 20 | ICC(3,2)=0.85 (0.61–0.94) | 0.66 | 1.83 |
| Inter-rater | 34 | ICC(2,2)=0.80 (0.61–0.90) | 0.87 | 2.42 |
| Passive | ||||
| Intra-rater | 20 | ICC(3,2)=0.84 (0.60–0.94) | 0.74 | 2.05 |
| Inter-rater | 34 | ICC(2,2)=0.81 (0.62–0.91) | 0.85 | 2.36 |
Mauchly's test indicated that the assumption of sphericity had been violated [X2(2)=38.5, p<0.001]. Therefore, degrees of freedom were corrected with a Greenhouse–Geisser estimate of sphericity (¿=0.59). Pectoralis minor muscle length was 16.31, SD=1.6 1.64cm for resting, 19.97, SD=1.6 1.92cm for actively lengthened, and 21.03±1.94cm for the passively lengthened condition. Results showed a significant difference among all three length conditions [F(1.2,38.8)=354.2, p<0.001]. Post hoc pairwise comparisons revealed significant differences between rest-active conditions (3.66, SD=1.6 1.36cm, p<0.001), rest-passive conditions (4.72, SD=1.6 1.41cm, p<0.000), and active-passive conditions (1.06, SD=1.6 0.47cm, p<0.001).
DiscussionIn order to make sound clinical decisions, health care providers should know the psychometric properties of the measures they choose to collect on their patients.24 Adequate relative and absolute reliability are two essential psychometric properties of any measurement intended for clinical decision making. The findings from our study demonstrate that our method of measuring pectoralis minor muscle length in a resting position, as well as when the muscle was actively and passively lengthened, has acceptable intra- and inter-rater reliability for use in clinical settings.
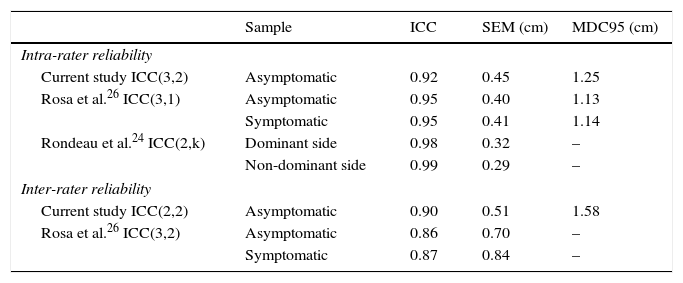
Our intra-rater reliability values for resting pectoralis minor muscle length (ICC(3,2)=0.92, SEM=0.45cm, MDC95=1.25cm) are very similar to those previously reported (Table 2).25,26 As noted in Table 2, our 95% confidence intervals indicate good to excellent reliability for measuring resting pectoralis minor muscle length. Collectively, these findings demonstrate excellent intra- and inter-rater reliability, with small measurement error, when using a caliper or tape measure to measure resting pectoralis minor muscle length. However, a resting measurement of muscle length only provides part of the information needed to determine muscle extensibility.
Comparison of reliability studies for measuring resting pectoralis minor muscle length.
| Sample | ICC | SEM (cm) | MDC95 (cm) | |
|---|---|---|---|---|
| Intra-rater reliability | ||||
| Current study ICC(3,2) | Asymptomatic | 0.92 | 0.45 | 1.25 |
| Rosa et al.26 ICC(3,1) | Asymptomatic | 0.95 | 0.40 | 1.13 |
| Symptomatic | 0.95 | 0.41 | 1.14 | |
| Rondeau et al.24 ICC(2,k) | Dominant side | 0.98 | 0.32 | – |
| Non-dominant side | 0.99 | 0.29 | – | |
| Inter-rater reliability | ||||
| Current study ICC(2,2) | Asymptomatic | 0.90 | 0.51 | 1.58 |
| Rosa et al.26 ICC(3,2) | Asymptomatic | 0.86 | 0.70 | – |
| Symptomatic | 0.87 | 0.84 | – | |
ICC, intraclass correlation coefficient; SEM, standard error of measurement; MDC, minimal detectable change.
To the best of our knowledge, we are the first to report intra- and inter-rater reliability for measures of pectoralis minor muscle length under actively and passively lengthened conditions. The ICC, SEM, and MDC95 for our measurements ranged from 0.80–0.85, 0.66–0.87cm, and 1.83–2.42cm, respectively. As noted in Table 2, our 95% confidence intervals indicate good to excellent intra- and inter-rater reliability for measures of pectoralis minor muscle length under actively lengthened conditions. For measures of pectoralis minor muscle length under passive conditions, our 95% confidence intervals indicate good to excellent inter-rater reliability and fair to excellent intra-rater reliability.
The significant changes in pectoralis minor muscle length across muscle length conditions provides data to support the construct validity of our procedures for actively and passively lengthening the muscle. During the active and passive lengthened conditions, there was an averaged increase in pectoralis minor muscle length, beyond resting length, of 3.66cm and 4.72cm, respectively. Eighty-eight percent (30/34) of measures exceeded our MDC95 values for the active condition (1.83cm) and 97% (33/34) exceeded the passive condition (2.05cm), which indicates a true change in muscle length. Although a significant difference was noted in muscle length between the active and passive conditions, this difference was small (1.06cm) and within our measurement error.
We believe the findings from our study provide clinicians with a reliable procedure for obtaining measures of pectoralis minor muscle length, which can then be used to determine muscle extensibility. While a tight or shortened pectoralis minor muscle has been theorized to play an important role in the development of shoulder pain and dysfunction, information about pectoralis minor muscle extensibility and what constitutes a shortened pectoralis minor muscle is currently unknown.12,16 Although Borstad has provided information about typical resting pectoralis minor muscle length and cut points for defining shorter and longer resting muscle lengths, these values do not provide information about whether or not the pectoralis minor muscle is shortened.11,17 Participants in our study demonstrated, on average, a 22.4% and 29% increase in pectoralis minor muscle length during the actively and passively lengthened conditions when compared to the resting position. This information may be viewed as a starting point for defining normal pectoralis minor muscle extensibility, as well as what constitutes a shortened muscle.
The information provided by the active and passive length conditions may also be useful to clinicians for selecting exercises intended to stretch the pectoralis minor muscle. While the optimal stretch has yet to be defined, Borstad and Ludewig12 reported that the unilateral corner stretch was more effective for elongating the pectoralis minor muscle than a supine manual or sitting manual stretch.12 The mean pectoralis minor muscle length change during the corner stretch for the 50 healthy participants in Borstad and Ludewig's12 study was 2.24cm. The mean muscle length changes for the active and passive conditions in the current study were 3.66cm and 4.72cm, respectively. These findings suggest that the procedures described in this study for actively or passively lengthening the pectoralis minor muscle may be more effective than a unilateral corner stretch. Although a caliper was used in our study to measure pectoralis minor muscle length and an electromagnetic tracking system was used in Borstad and Ludewig's12 study, both studies used the same bony landmarks as a reference for their muscle length measures, and each instrument measured the linear distance between those landmarks.12 While the pectoralis minor muscle is lengthened during the corner stretch, lengthening of the pectoralis major muscle also likely occurs during this stretch.27 This may explain why the muscle length change reported by Borstad and Ludewig12 is smaller than our active and passive muscle length changes. As reported previously, our procedures for lengthening the pectoralis minor muscle were based on a cadaveric study by Muraki et al.22 In their study, displacement sensors were directly attached to the pectoralis minor muscles in nine cadaveric specimens. These sensors measured muscle length changes during three different stretches (scapular retraction at 0° and 30° of flexion and horizontal abduction with the arm in 90° of abduction and external rotation). Findings from their study revealed the greatest change in pectoralis minor muscle length during the scapular retraction at 30° of flexion stretch.22
We are aware of one study that has investigated the immediate effect of pectoralis minor muscle stretching on pectoralis minor muscle length. Williams et al.28 demonstrated a statistically significant increase in resting pectoralis minor muscle length (distance between coracoid process and 4th rib measured via a tape measure) following two repetitions of a horizontal abduction stretch (supine, shoulder in 90° of abduction and external rotation, overpressure applied into horizontal abduction). Their reported average change in resting muscle length of 0.6cm is small and of questionable clinical significance. Although not reported by Williams et al., this small change in resting muscle length falls within our intra-rater resting muscle length measurement error (1.25cm).28 One possible explanation for why larger changes in resting pectoralis minor muscle length were not found in their study is that perhaps none of the participants in their study had a shortened pectoralis minor muscle prior to the stretching. This further supports the construct that measures of resting pectoralis minor muscle length do not provide adequate information for determining if the muscle is shortened.
LimitationsThe fact that all of the participants in the current study were young and not experiencing shoulder pain is a potential limitation of the study. While further studies are needed to investigate the reliability of these measures in individuals with current shoulder pain, we believe our findings provide a foundation upon which further studies can build. Other potential limitations are the use of two examiners to obtain muscle length measures during the passive condition and our criteria for what constituted two acceptable repeated measures (within 0.5cm of one another). While we acknowledge the fact that requiring two examiners to perform the passive assessment may not be practical in a busy clinic setting, this is in line with what has been described for obtaining measures of shoulder internal rotation range of motion measures.29,30 It should be noted that differences in muscle length change between the active and passive conditions were small and insignificant. This would indicate that active measures of pectoralis minor muscle length may provide adequate information that could then be used to determine pectoralis minor muscle extensibility. Obviously, if additional information about pectoralis minor muscle extensibility that may be gathered via the end feel is desired, then a second examiner may be beneficial. Concerning our criteria for two acceptable measures, the maximum number of measures on any participant needed to satisfy our criteria (two measures within 0.5cm of one another) was three. This additional time needed to acquire a third measure would not be a major limitation, even in a busy clinic.
ConclusionsIn conclusion, the procedures described in this study for measuring pectoralis minor muscle length under resting, actively lengthened, and passively lengthened conditions have acceptable reliability for clinical decision making. Additionally, the active and passive lengthening procedures resulted in great changes in pectoralis minor muscle length. Collectively, this information can be used to inform future studies designed to determine an operational definition for shortened pectoralis minor muscle and to establish optimal stretches for restoring pectoralis minor muscle length.
Ethical approvalDrexel University Institutional Review Board, Protocol # 1408003050.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interestThe authors declare no conflicts of interest.



