

To investigate knee pain prevalence, associated factors, and functional impairment among adolescents.
MethodThis was a cross-sectional study conducted between May and June 2014 with a random sample of 619 adolescents aged between 10 and 17 years. Knee pain prevalence was investigated using the Nordic Questionnaire for Osteomuscular Symptoms and a number of independent variables (demographic data, nutritional status, form of carrying backpacks, and pain during and after walking) obtained by self-report questionnaires. Physical impairment of the knee was assessed using the Brazilian version of the Knee injury and Osteoarthritis Outcome Score questionnaire. Poisson regression analysis was used to estimate the ratios of crude and adjusted knee pain association with the investigated factors. ANOVA and Kruskal–Wallis tests were used to compare median functional impairment.
ResultsKnee pain prevalence over the last 7 days was 22.6%. Factors having significant association with the outcome were: being between 12 and 14 years old (PR: 1.67; 95% CI: 1.07–2.58; p<0.01), being between 15 and 17 years old (PR: 2.44; 95% CI: 1.51–3.94; p=0.01), and not doing physical education at school (PR: 0.54; 95% CI: 0.35–0.82; p=0.01). Total functional capacity among adolescents with pain was significantly lower among girls (68.7 points; PD±15.1) when compared with boys (74.3 points; PD±12.7) (p=0.02). The mean value of disabling pain was lower (55.1 points; PD±12.3) among adolescents who were physically active in their leisure time compared to those who were insufficiently active (60.4 points; PD±12.4) (p=0.02).
ConclusionThe results of this study show that knee pain among adolescents with no previous history should be investigated, particularly among older adolescents who do not have physical education at school, since it is highly prevalent and can result in functional impairment. Regarding functionality, more attention should be given to girls and adolescents who were physically active in their leisure time.
Knee pain is a common clinical symptom in the adult population and affects half of the population aged over 50.1 Knee pain results in substantial costs for the health system given that one in every six individuals with knee pain will have at least one medical appointment per year and one third of them will have disability.2,3 Although knee pain prevalence is lower among adolescents, it does provide reason for concern and can be a precursor of this type of pain in adult life.3 Between 19% and 31% of adolescents report knee pain and this complaint may arise from traumatic injuries or may be insidious.4–6
The literature has shown that knee pain does not always have a favorable prognosis. About 50% of adolescents continue to report pain after a year of investigation and this is significantly harmful to their quality of life.7 After following up a group of women with insidious onset of knee pain during a 20-year period, Nimon et al.8 found that 78% continued to report having knee pain at the end of the study. In addition, knee pain can cause functional impairment in adolescents, limiting or interrupting everyday activities and consequently reducing academic performance.9
The main factors associated with unspecified knee pain among adolescents are being female, doing sports activities, being obese, and being older.7,10,11 Rathleff et al.7 report that girls have four times higher probability of having knee pain. In addition, doing physical activities during leisure time more than twice a week is also associated with increased probability of knee pain. Greater knee pain prevalence among obese people is associated with reduced joint space and increased Q angle, thus compromising the kinematics of this joint.12 One study reported that greater knee pain problems occur in older adolescents as a result of puberty and greater exposure time to associated factors.13 Some external factors have also been considered as predictors of knee pain. These include physical exertion related to improper use of backpacks and remaining in a sitting position for long periods of time while using videogames or computers.11
However, the majority of the studies cited are of clinical trial design and assess individuals diagnosed as having orthopedic knee conditions. There are few national studies that have an epidemiological approach to musculoskeletal knee pain among adolescents and that assess their functional impairment.
Therefore, it is relevant to conduct a study that provides more information about adolescent musculoskeletal health, with emphasis on knee pain, thus increasing knowledge about associated factors underlying the emergence of knee pain. The objective of this study was to investigate knee pain prevalence, associated factors, and resulting functional impairment among adolescents attending municipal schools in a city in southern Brazil.
MethodThis is a cross-sectional study with adolescents enrolled at schools in the city of Rio Grande, Brazil. This city is located in the south of Brazil and has a population of approximately 206,161 inhabitants, with 57,563 students attending public schools.14
All five institutions that took part in the study were distributed in different neighborhoods of the city and were randomly selected from a list of public elementary schools involved in projects conducted by Universidade Federal do Rio Grande (UFRG), Rio Grande, RS, Brazil.
The sample size was calculated using the following parameters: 19% knee pain prevalence, 5% alpha error, and 3.5% precision. Controlling for gender, this resulted in a sample of 482 subjects. After adding 10% for losses and 15% for confounding factors, the total sample size needed was 610 adolescents.
Students aged 10–17 were selected randomly from each 5th to 9th grade class register. The adolescents were selected randomly from the class register, ensuring proportionality in relation to the number of enrolled students, the number of classes, and the size of the school. Proportionality was calculated taking into consideration the size of the school and the number of adolescents of eligible age for the study.
Students who were not able to understand and answer the data collection instrument and those who used walking aids were excluded from the study. These students were identified prior to data collection based on information provided by the school administration.
The study was conducted between May and June 2014. Data collection took place at the schools during normal class time in an especially reserved place defined beforehand by the school administration. Three trained interviewers collected data. The interviewers were final-year physical therapy degree students with previous research experience during their undergraduate studies. They also received 20h of theoretical and practical training from the first author of this study. The last stage of the interviewers’ training was the application of the pilot study under the continuous supervision of the researcher in charge.
The first stage of data collection consisted of measuring body weight and height and the weight of the students’ backpacks. 150kg mechanical anthropometric scales with an attached anthropometer were used. The adolescents were weighed without shoes and with the minimum amount of clothing. The same equipment was used to weigh their backpacks.
A simplified version of the Nordic Questionnaire for Osteomuscular Symptoms (NQOS) adapted to exclude variables relating to occupational status was used to assess the presence of knee pain.15 The outcome was assessed based on the answer to the following question: “At any time during the last 7 days, have you had problems with your knee (such as pain and discomfort)?” NQOS is a quantitative instrument that identifies the presence, location, and magnitude of osteomuscular symptoms. The original version of the instrument assesses the presence of musculoskeletal pain during 12 months and 7 days prior to the interview. However, only symptoms occurring during the last 7 days were considered in this study.
Body mass index (BMI) normalized by age – BMI/age (based on the adolescents’ gender, age, weight, and height) and level of physical activity during leisure (assessed using the long version of the International Physical Activity Questionnaire – IPAQ) were also calculated.16,17
The independent variables analyzed were: gender (boys and girls); age (10–11 years; 12–14 years; 15–17 years); skin color (white; black/brown); BMI/age (normal; overweight; obese); doing or not doing physical education at school in the last week; physical activity during leisure time (physically active: more than 300min a week doing physical activities during leisure time, or insufficiently active); backpack weight (≤10% and >10% of body weight); and the way they carried their backpacks (on their backs; using arms/hands).
Knee functional impairment was also investigated by applying the Brazilian version of the Knee injury and Osteoarthritis Outcome Score (KOOS) questionnaire.18 This instrument assesses knee functional impairment during the week prior to the interview in relation to the following items: symptoms (edema, crepitation, difficulty in bending, straightening, and stiffness), pain (pain frequency and intensity when twisting, straightening, bending, when walking, remaining seated, standing upright, lying, and when going up or down stairs), daily living activities, sports activities, leisure activities, and quality of life. The score for each of the items was calculated, as was the total score for the instrument. The scores were calculated as recommended by the instrument, whereby a score of 100 indicates no loss of functional impairment and a score of zero indicates extreme loss (www.koos.nu). We opted for the use of KOOS for adults because this is validated for the Portuguese language and has already been used in previous research on populations and outcomes similar to this study.13 Furthermore, there is little difference between the instrument for adults and children.
For the purposes of multivariate analysis, the exposure variables were selected after reviewing the literature and were organized according to the following hierarchical model: 1st level – Demographic characteristics (age, gender, skin color); 2nd level – Biological determinants (nutritional status – BMI/age); School-associated factors (how they carried their backpack, backpack weight); 3rd level – Lifestyle (doing physical education at school, doing physical activities during leisure time).
EpiData 3.1 was used to create the database and STATA 10.0 was used to analyze the data. First, variable frequency distribution was assessed. The magnitude of the association between knee pain and the independent variables was estimated by calculating the ratio of crude and adjusted prevalence and respective confidence intervals (95%) using the Poisson regression method and robust variance estimates. At each level, the variables were adjusted both between each other and also for the variables on the lower levels using backward selection, taking a p value of <0.20 for the inclusion of variables during adjusted analysis, level by level. Values of p<0.05 were considered to be significant. Concerning the analysis of functional impairment, first variance heterogeneity and homogeneity were assessed. Based on the result of this assessment, ANOVA was used for parametric variables, and Kruskal–Wallis was used for non-parametric variables.
The study was approved by the UFRG Health Research Ethics Committee, Rio Grande, RS, Brazil (CEPAS-UFRG), report number 174/2013. Parents and/or legal guardians signed an informed consent form. The adolescents took part voluntarily and signed an agreement form.
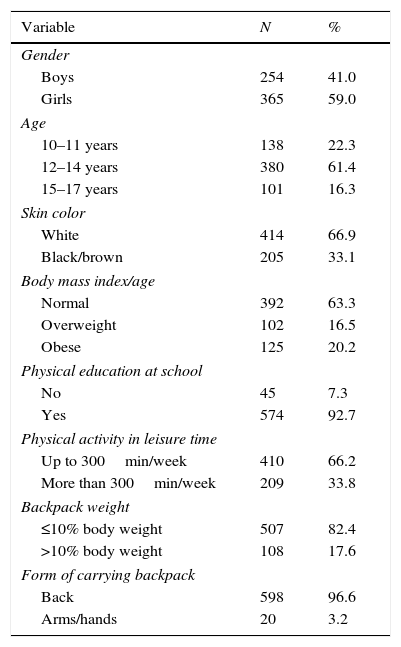
Results650 adolescents were invited to take part in the study and 619 were interviewed, totaling 4.8% losses and refusals. 59.0% were girls, 61.4% were aged between 12 and 14, and 66.9% had white skin color.
63.3% of the participants had normal BMI/age ratings, the majority (92.7%) did physical education at school, and 33.8% were considered to be active with regards of being physically active in their leisure time. 17.6% carried more than 10% of their body weight in their backpacks, and 96.6% carried their backpacks on their backs (Table 1).
Characterization of the sample of adolescents attending municipal schools in the city of Rio Grande, RS, Brazil, 2014 (n=619).
| Variable | N | % |
|---|---|---|
| Gender | ||
| Boys | 254 | 41.0 |
| Girls | 365 | 59.0 |
| Age | ||
| 10–11 years | 138 | 22.3 |
| 12–14 years | 380 | 61.4 |
| 15–17 years | 101 | 16.3 |
| Skin color | ||
| White | 414 | 66.9 |
| Black/brown | 205 | 33.1 |
| Body mass index/age | ||
| Normal | 392 | 63.3 |
| Overweight | 102 | 16.5 |
| Obese | 125 | 20.2 |
| Physical education at school | ||
| No | 45 | 7.3 |
| Yes | 574 | 92.7 |
| Physical activity in leisure time | ||
| Up to 300min/week | 410 | 66.2 |
| More than 300min/week | 209 | 33.8 |
| Backpack weight | ||
| ≤10% body weight | 507 | 82.4 |
| >10% body weight | 108 | 17.6 |
| Form of carrying backpack | ||
| Back | 598 | 96.6 |
| Arms/hands | 20 | 3.2 |
Knee pain prevalence among the adolescents assessed was 22.6% (n=140), with no difference between boys and girls. Pain prevalence was found to increase as age increased, varying between 14.5% in those aged 10 and 11 and 34.7% in those aged 15 and 17 (Table 2).
Knee pain prevalence, crude and adjusted analysis of the association between the outcome and selected variables among adolescents (n=619) attending municipal schools in the city of Rio Grande, RS, Brazil, 2014.
| Variable | Knee pain | Crude analysis | p-value | Adjusted analysis | p-value | |||
|---|---|---|---|---|---|---|---|---|
| Yes | No | PR (95% CI) | PR (95% CI) | |||||
| N | % | n | % | |||||
| Gender | 0.63 | 0.74 | ||||||
| Boys | 55 | 21.6 | 199 | 78.4 | 1 | 1 | ||
| Girls | 85 | 23.3 | 280 | 76.7 | 1.08 (0.79–1.45) | 1.05 (0.78–1.41) | ||
| Age | <0.01a | <0.01a | ||||||
| 10–11 years | 20 | 14.5 | 118 | 85.5 | 1 | 1 | ||
| 12–14 years | 85 | 22.4 | 295 | 77.6 | 1.54 (0.99–2.41) | 1.67 (1.07–2.58) | ||
| 15–17 years | 35 | 34.7 | 66 | 65.3 | 2.39 (1.47–3.88) | 2.44 (1.51–3.94) | ||
| Skin color | 0.12 | 0.29 | ||||||
| White | 86 | 20.8 | 328 | 79.2 | 1 | 1 | ||
| Black/brown | 54 | 26.3 | 151 | 73.7 | 1.26 (0.94–1.70) | 1.17 (0.87–1.58) | ||
| Body mass index/age | 0.6 | 0.54 | ||||||
| Normal | 92 | 23.5 | 300 | 76.5 | 1 | 1 | ||
| Overweight | 20 | 19.6 | 82 | 80.4 | 0.83 (0.59–1.28) | 0.88 (0.57–1.37) | ||
| Obese | 28 | 22.4 | 97 | 77.6 | 0.95 (0.65–1.38) | 1.12 (0.76–1.66) | ||
| Physical education at school | 0.01a | 0.01a | ||||||
| No | 17 | 37.8 | 28 | 62.2 | 1 | 1 | ||
| Yes | 123 | 21.4 | 451 | 78.6 | 0.57 (0.37–0.85) | 0.54 (0.35–0.82) | ||
| Physical activity in leisure time | 0.72 | 0.65 | ||||||
| Insufficiently active | 91 | 22.2 | 319 | 77.8 | 1 | 1 | ||
| Active | 49 | 23.4 | 160 | 76.6 | 1.05 (0.77–1.43) | 1.07 (0.79–1.45) | ||
| Backpack weight | 0.72 | 0.31 | ||||||
| ≤10% body weight | 114 | 22.5 | 393 | 77.5 | 1 | 1 | ||
| >10% body weight | 26 | 24.1 | 82 | 75.9 | 1.07 (0.73–1.55) | 1.21 (0.83–1.77) | ||
| Form of carrying backpack | 0.77 | 0.91 | ||||||
| Back | 136 | 22.7 | 462 | 77.3 | 1 | 1 | ||
| Arms/hands | 4 | 20.0 | 16 | 80.0 | 0.88 (0.36–2.14) | 1.05 (0.44–2.48) | ||
PR (95% CI), prevalence ratio (95% CI). Multivariate analysis: 1st level – Demographic characteristics (age, gender, skin color); 2nd level – Biological determinants (nutritional status – BMI/age); School-associated factors (form of carrying backpack, backpack weight); 3rd level – Lifestyles (doing physical education at school, doing physical activities during leisure time).
Adolescents who did not take part in physical education at school reported more pain (37.8%; 95% CI: 0.37–0.85; p=0.01) than those who did. No significant differences were found in the other variable categories investigated (Table 2).
Age and doing physical education at school remained associated with the outcome in the adjusted analysis. Students aged between 12 and 14 were 67% more likely to have knee pain when compared to those aged under 12 (95% CI: 1.07–2.58; p<0.01). This probability was more than two times greater (95% CI: 1.51–3.94; p<0.01) among those aged 15–17. Furthermore, those who did physical education at school were less likely to have knee pain than those who did not take part in this activity (95% CI: 0.35–0.82; p=0.01). The remaining variables did not have significant association with the outcome studied (Table 2).
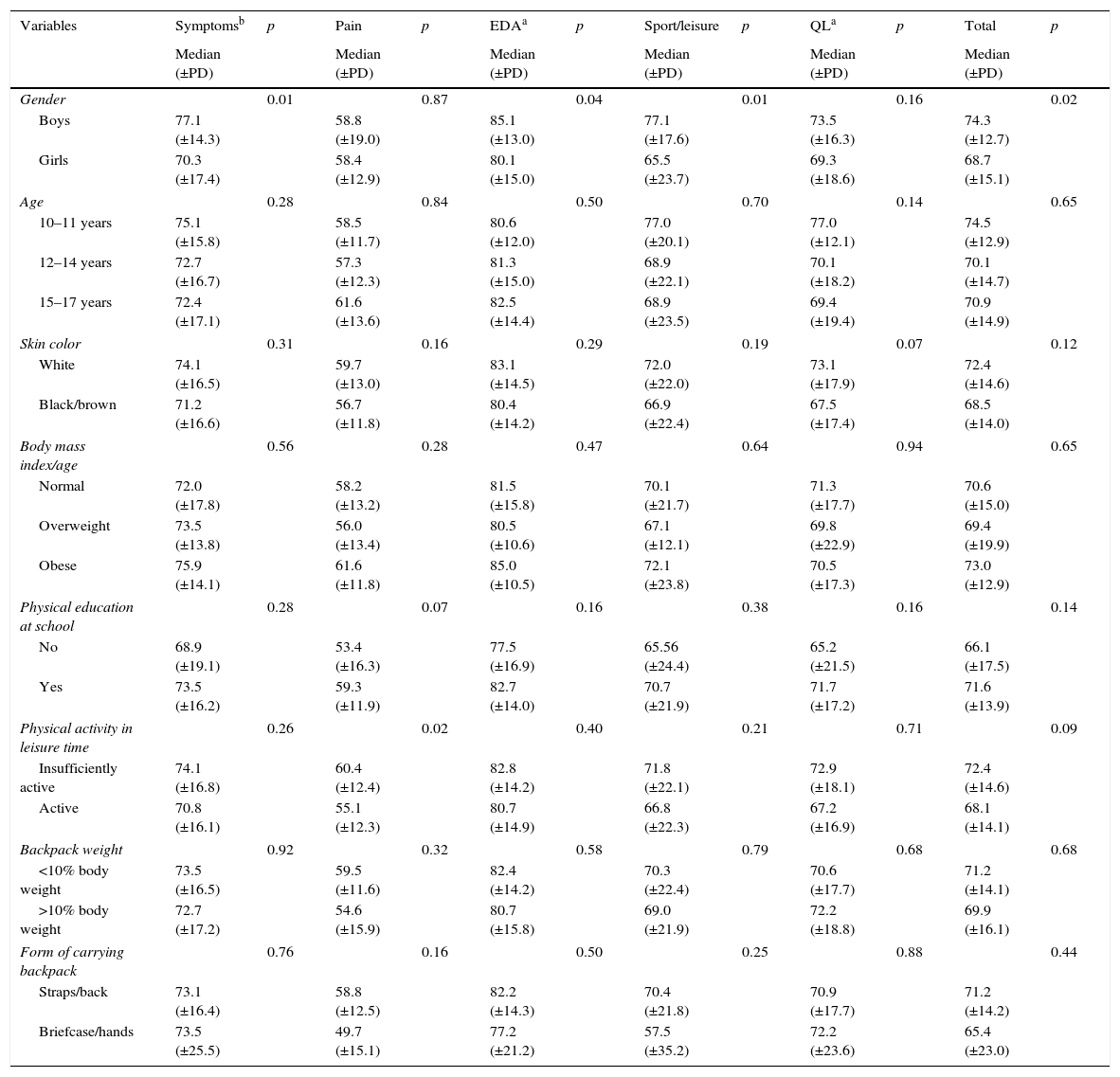
An assessment of functional impairment was performed on those adolescents who reported having knee pain (n=140). The results showed greater functional impairment in adolescent girls (p=0.02). When evaluating separately each of the items of the instrument used to assess knee functional impairment, we found significantly lower mean pain in the following items: symptoms, such as edema, crepitation, difficulty in bending, straightening, and stiffness (p=0.01); disability in daily life activities (p=0.04) and in sports and leisure activities (p=0.01) among adolescent girls. In addition, the analysis of functional impairment revealed a significantly lower mean level of painful symptoms during twisting, straightening, bending, when walking, remaining seated, standing upright, lying and when going up or down stairs among adolescents who were active in their leisure time (p=0.02). The remaining variables did not show statistically significant differences (Table 3).
Functional impairment of the knee in adolescents evaluated by KOOS (n=140), attending municipal schools in the city of Rio Grande, RS, Brazil, 2014.
| Variables | Symptomsb | p | Pain | p | EDAa | p | Sport/leisure | p | QLa | p | Total | p |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median (±PD) | Median (±PD) | Median (±PD) | Median (±PD) | Median (±PD) | Median (±PD) | |||||||
| Gender | 0.01 | 0.87 | 0.04 | 0.01 | 0.16 | 0.02 | ||||||
| Boys | 77.1 (±14.3) | 58.8 (±19.0) | 85.1 (±13.0) | 77.1 (±17.6) | 73.5 (±16.3) | 74.3 (±12.7) | ||||||
| Girls | 70.3 (±17.4) | 58.4 (±12.9) | 80.1 (±15.0) | 65.5 (±23.7) | 69.3 (±18.6) | 68.7 (±15.1) | ||||||
| Age | 0.28 | 0.84 | 0.50 | 0.70 | 0.14 | 0.65 | ||||||
| 10–11 years | 75.1 (±15.8) | 58.5 (±11.7) | 80.6 (±12.0) | 77.0 (±20.1) | 77.0 (±12.1) | 74.5 (±12.9) | ||||||
| 12–14 years | 72.7 (±16.7) | 57.3 (±12.3) | 81.3 (±15.0) | 68.9 (±22.1) | 70.1 (±18.2) | 70.1 (±14.7) | ||||||
| 15–17 years | 72.4 (±17.1) | 61.6 (±13.6) | 82.5 (±14.4) | 68.9 (±23.5) | 69.4 (±19.4) | 70.9 (±14.9) | ||||||
| Skin color | 0.31 | 0.16 | 0.29 | 0.19 | 0.07 | 0.12 | ||||||
| White | 74.1 (±16.5) | 59.7 (±13.0) | 83.1 (±14.5) | 72.0 (±22.0) | 73.1 (±17.9) | 72.4 (±14.6) | ||||||
| Black/brown | 71.2 (±16.6) | 56.7 (±11.8) | 80.4 (±14.2) | 66.9 (±22.4) | 67.5 (±17.4) | 68.5 (±14.0) | ||||||
| Body mass index/age | 0.56 | 0.28 | 0.47 | 0.64 | 0.94 | 0.65 | ||||||
| Normal | 72.0 (±17.8) | 58.2 (±13.2) | 81.5 (±15.8) | 70.1 (±21.7) | 71.3 (±17.7) | 70.6 (±15.0) | ||||||
| Overweight | 73.5 (±13.8) | 56.0 (±13.4) | 80.5 (±10.6) | 67.1 (±12.1) | 69.8 (±22.9) | 69.4 (±19.9) | ||||||
| Obese | 75.9 (±14.1) | 61.6 (±11.8) | 85.0 (±10.5) | 72.1 (±23.8) | 70.5 (±17.3) | 73.0 (±12.9) | ||||||
| Physical education at school | 0.28 | 0.07 | 0.16 | 0.38 | 0.16 | 0.14 | ||||||
| No | 68.9 (±19.1) | 53.4 (±16.3) | 77.5 (±16.9) | 65.56 (±24.4) | 65.2 (±21.5) | 66.1 (±17.5) | ||||||
| Yes | 73.5 (±16.2) | 59.3 (±11.9) | 82.7 (±14.0) | 70.7 (±21.9) | 71.7 (±17.2) | 71.6 (±13.9) | ||||||
| Physical activity in leisure time | 0.26 | 0.02 | 0.40 | 0.21 | 0.71 | 0.09 | ||||||
| Insufficiently active | 74.1 (±16.8) | 60.4 (±12.4) | 82.8 (±14.2) | 71.8 (±22.1) | 72.9 (±18.1) | 72.4 (±14.6) | ||||||
| Active | 70.8 (±16.1) | 55.1 (±12.3) | 80.7 (±14.9) | 66.8 (±22.3) | 67.2 (±16.9) | 68.1 (±14.1) | ||||||
| Backpack weight | 0.92 | 0.32 | 0.58 | 0.79 | 0.68 | 0.68 | ||||||
| <10% body weight | 73.5 (±16.5) | 59.5 (±11.6) | 82.4 (±14.2) | 70.3 (±22.4) | 70.6 (±17.7) | 71.2 (±14.1) | ||||||
| >10% body weight | 72.7 (±17.2) | 54.6 (±15.9) | 80.7 (±15.8) | 69.0 (±21.9) | 72.2 (±18.8) | 69.9 (±16.1) | ||||||
| Form of carrying backpack | 0.76 | 0.16 | 0.50 | 0.25 | 0.88 | 0.44 | ||||||
| Straps/back | 73.1 (±16.4) | 58.8 (±12.5) | 82.2 (±14.3) | 70.4 (±21.8) | 70.9 (±17.7) | 71.2 (±14.2) | ||||||
| Briefcase/hands | 73.5 (±25.5) | 49.7 (±15.1) | 77.2 (±21.2) | 57.5 (±35.2) | 72.2 (±23.6) | 65.4 (±23.0) | ||||||
The results show knee pain prevalence over the last 7 days was 22.6%. This finding is similar to the levels reported in the literature, which ranges between 18.5% and 31%.8,10,13,18 Musculoskeletal pain, including knee pain, is one of the reasons why people seek primary health care services, whereby 18% of those seeking these services are adolescents.5
This study did not find any associations between the outcome and gender in the multivariate analysis. Nevertheless, the results relating to functional impairment indicate that girls have statistically greater functional impairment when compared to boys. We believe that this discrepancy between the lack of association with the outcome and the presence of association in the assessment of functional impairment may be explained by the higher prevalence of symptoms such as edema, crepitation, difficulty in bending, straightening and stiffness, greater difficulty in doing daily living activities, sports, and leisure activities in adolescent girls with knee pain. When investigating knee pain prevalence among 2368 German adolescents, Spahn et al.19 also did not find an association with gender. Nevertheless, knee pain in women may not be a benign condition. A study conducted by Nimon et al.8 reported that 25% of women with knee pain diagnosed when they were adolescents continued to have painful symptoms 15 years later. 45% believed that this pain affected their daily lives and 36% reported that it restricted their daily activities. However, as yet there is no consensus in the literature as to the reasons for gender differences regarding knee pain. It has been suggested that hormone differences, as well as differences in body composition, psychosocial aspects, knee structure, and neural processing may explain greater prevalence of knee pain and knee incapacity among women.20–22
Our results show a progressive increase in knee pain prevalence as the age of the adolescents studied increased. These findings are corroborated by a study conducted in Finland by Vähäsarja10 with 967 adolescents, which found that older adolescents had significantly more knee pain (p<0.001) than children (aged 9–10). The same study found 18.5% knee pain prevalence at the time of assessment among adolescents and 3.9% among children. There was no difference between genders. Confirming the hypotheses raised in the literature, we believe that this association is due to older adolescents spending more time exposed to associated factors, thus resulting in greater knee pain prevalence in this population.22
When comparing the presence of musculoskeletal pain among children and adolescents with and without excess body weight, Stovitz et al.9 found significantly higher knee pain prevalence in those with excess weight. Conversely, our results did not find an association between the presence of knee pain and increased body weight among adolescents. We believe that the absence of association may be explained by the lower exposure of overweight/obese adolescents to the associated factors reported in the literature, such as reduced participation in physical education at school and during leisure time. However, the literature reports that obesity is an associated factor for osteoarthritis, and that the association between osteoarthritis of the knee and obesity can result in high levels of pain and functional difficulties, highlighting the need for studies that address this interface.23,24
The literature reports that in general musculoskeletal pain is greater among individuals with black/brown skin color.25 However, in our study, no association was found between knee pain and the adolescents’ skin color.
Doing physical education at school showed itself to be a factor of protection against the onset of knee pain. Similarly, adolescents with knee pain who did not do physical education had greater functional impairment of the knee joint in all of the items assessed, although no significant difference was found in these items. Some studies report associations between physical inactivity and chronic musculoskeletal pain.26 In contrast to this, a study conducted with 624 Brazilian school students did not find an association with doing physical education when assessing diffuse musculoskeletal pain.27 Taking into consideration that there is no consensus regarding the association between doing physical activity and the presence of knee pain, investment needs to be made in studies with different designs capable of ascertaining whether pain is a cause or a consequence of inactivity.
Our study did not find associations between excessive backpack weight, the way backpacks were carried, and presence of knee pain. However, there was also a tendency for greater functional impairment among adolescents with knee pain who carried more weight in their backpacks and carried them with their arms/hands, although there was no significant difference between the median values of these items. The literature diverges as to the possibility of excessive backpack weight being a predisposing factor for knee joint pain.10,28 Some studies report that carrying excessive loads affects lower limb joints, altering gait kinematics, causing greater knee flexion and anterior-posterior rotation, quadriceps muscle fatigue, increased ground contact stress, and inability to absorb impact when walking.29,30
Although the multivariate analysis did not find an association between the outcome and doing more than 300min of physical activity during leisure time, nevertheless among adolescents who had knee pain, disabling pain was significantly greater in those considered to be physically active in their leisure time. Doing regular physical activity has been considered an associated factor for patellofemoral syndrome, this being a condition that affects the knees of approximately 25% of youths.31 Nevertheless, this condition can be prevented through the early inclusion of exercises to strengthen lower limb muscles as part of routine physical activities.31
It is important to mention some of the limitations of this study. The outcome assessed is knee pain reported by adolescents without using examinations to validate the data with objective observations. Nevertheless, it should be stressed that care was taken to ask if there had been painful symptoms in the last 7 days, and this undoubtedly provides more reliable information regarding the pain/discomfort felt by the study participants, as well as minimizing memory recall bias. Secondly, the respondents themselves reported their pain, thus not allowing an assessment of the chronicity of the pain investigated, and we therefore cannot exclude the possibility of complaints of pain being overestimated or underestimated.
ConclusionThe results of this study reveal high knee pain prevalence, especially among older adolescents who do not have physical education at school. This can lead to functional impairment among this population. This study contributes to the national literature, which is still scarce on this subject. We conclude that the need exists to concentrate efforts in order to undertake new studies aimed at obtaining better understanding of knee pain, its associated factors, and its prognosis for adult life, thus achieving early diagnosis and preventing possible problems in this joint.
Conflicts of interestThe authors declare no conflicts of interest.



