


This observational research study analyses the uptake of physical therapies treatments in the Polyclinic during the Rio 2016 Olympic Games.
ObjectiveTo describe the usage of physical therapies services – physical therapy, osteopath, chiropractic, and sports massage – by athletes and non-athletes and across different sports.
MethodsThe multidisciplinary team of physical therapies recorded treatment modalities, information on provider discipline and reason for attendance, in an Electronic Medical Record system throughout the 32 days of operation of the Olympic Polyclinic. Cold-therapy total immersion ice baths (TIIB) were provided as part of the services, but were reported and analysed separately.
ResultsThere were 4993 encounters (4038 athletes, 955 non-athlete encounters). 1395 athletes (12.4% of all athletes) and 393 non-athletes sought treatment. For all four provider disciplines, in addition to TIIB, the primary reason for athlete attendance was for recovery (52% of all encounters), followed by injury treatment (30%), and maintenance (16%). Athletes reported “injury” as the main reason for physical therapy (92% of all encounters, 2.8 encounters per athlete), chiropractic (94%, 1.9) and osteopathy (91%, 1.8) visits. Almost all TIIB visits were used for recovery (98% of all TIIB encounters; 2.1 encounters per athlete). Athletes from handball (37% of all handball athletes), followed by judo (22%), and athletics (21%), presented the largest user groups.
ConclusionThis Olympic Polyclinic study evaluates the physical therapies’ activity, and athlete's reason for use of the multidisciplinary physical therapies team, including total immersion ice bath provision. These results emphasise the importance of a multidisciplinary approach.
The protection of the health of the athlete is the core objective of the International Olympic Committee (IOC) Medical and Scientific Commission.1 During Olympic Games, the combined group of physical therapists from the National Olympic Committees (NOCs) and the hosts’ Organising Committee of the Olympic Games and Paralympic Games (OCOG) form the single largest professional group working for athlete health protection.2,3
While the role of a sports physical therapist traditionally has been to provide treatment and rehabilitation of injuries,4 the advancing role of the physical therapy profession is to also provide interventions on injury prevention, athlete recovery, and to support athlete performance.5 Also, physical therapy and the other disciplines osteopathy, chiropractic, and sports massage, have become a greater integral part of the sports medicine team, and thereby essentially contribute to an holistic approach for the care of the athlete.5
The physical therapies disciplines, including physical therapy, osteopaths, chiropractors, and sports massage practitioners, now provide a multidisciplinary approach providing a comprehensive spectrum of skill mix.5–8 A multidisciplinary team approach makes use of knowledge and expertise of different disciplines to provide better healthcare for the athlete, compared with disciplines working in isolation.5–11
In the Rio 2016 Olympic Games, 11238 athletes from 207 National Olympic Committees were competing in 28 sports, encompassing 306 events. Over the 32-day period of the Games, including the pre- and post-competition period, a total of 1101 injuries and 651 illnesses were recorded among the participating athletes.12 Many of these athletes availed of multidisciplinary interventions provided by the Polyclinic services.
To date, there have been few studies describing the use of physical therapy services at major multisport events, Pan-American Games,13 Africa Games,14 and the World Student Games.15 There have only been two studies published, evaluating the use of physical therapy services delivered from the polyclinic during Olympic Games,2,16 in addition to a brief report about the British Headquarters physical therapy activities during the Seoul 1988 Olympic Games,17 which discussed the services provided to one National Olympic Team. The role of the multidisciplinary team approach, providing physical therapy, osteopathy, chiropractic, and sports massage, and the use of total immersion ice baths (TIIB), for athletes from all competing National Olympic Teams has not been previously documented in an Olympic polyclinic setting.
We therefore aimed to (1) provide an analysis of the use of the physical therapies services – physical therapy, osteopath, chiropractic, and sports massage – by athletes and non-athletes, (2) gain an understanding of which disciplines and interventions were utilised the most across different sport, and (3) understand the reasons why athletes used these services.
MethodsDuring the Rio 2016 Olympic Games, the core of OCOG provided physical therapy and physical therapies services were delivered from the Polyclinic in the athlete Olympic Village.
In addition to NOCs providing their own dedicated physician and physical therapy services, the polyclinic OCOG services were available to all 11274 competing athletes from 207 NOCs. This also included care for accompanying NOC-accredited coaches, trainers, team managers, and members of the OCOG-workforce and the Olympic (IOC-accredited) family.
The polyclinic was open for a total of 32 days from the ‘pre-competition period’ (23rd July to the 5th August, 14 days), the ‘duration of Olympic competitions’ (5th to the 21st August, 16 days) and two days of ‘post-competition’ until the 23rd August.
Staffing of the multidisciplinary teamThe physical therapy services in an Olympic setting consists of multidisciplinary team, fulfilling the requirements of appropriate education, skills, and experience.18
The multidisciplinary physical therapies team at the Rio Olympic Games included 250 physical therapists, 190 sports massage practitioners, 30 osteopaths, and 30 chiropractors, all of whom were certified and licenced to practice in accordance with Olympic health care requirements. Each member of the physical therapies team for Rio 2016 was required to volunteer for 10 days, all members were required to work 8h a day on average, there were two daily shifts: 7 AM to 3 PM and 2 PM to 11 PM.
The protocol for the physical therapies services structure and organisation is specific for service of athletes at the time of an Olympic Games. Hence the organisational requirements may deviate from other parts of the world, as for example in Brazil, where physical therapists can deliver a variety of treatment modalities based on additional certificates in different skills. In Rio, all OCOG physical therapists were members of the Brazilian Physiotherapy Association and international volunteers had international qualifications recognised by the World Confederation for Physical Therapy. The 30 osteopaths and 30 chiropractors were recognised by COFFITO/ABFO (Brazilian osteopath physiotherapist association). International chiropractors and osteopaths were required to have internationally recognised qualifications by the general osteopathic council (GOC) and by the general chiropractic council (GCC), respectively. The 250 sports massage practitioners met the requirements of validated certification in sports massage. Acupuncture was solely provided by sports medicine physicians and administered in the facilities of the physical therapy department in accordance with the OCOG protocols. While it is acknowledged that many physical therapists are qualified to deliver acupuncture, the delivery of acupuncture was specific to the OCOG for the Rio Games. The international team members were only authorised to practice inside the Polyclinic, and for the 32-day period of the Olympic Games. All polyclinic treatments were referred directly via either an NOC physical therapist, or NOC or OCOG physician.
Clinical encounter form, Electronic Medical Records and definitionsAll treatment modalities and interventions and provider disciplines and reason for attendance were recorded on an Electronic Medical Record (EMR) (GE-IOC Electronic Medical Records System, GE Centricity Practice Solution, USA) at the Rio Olympic Games. The definition of injury, adapted from the IOC's injury and illness studies, was: any injury incurred in competition or training, receiving medical attention, regardless of the consequences with respect to absence from competition or training.19–21
An ‘encounter’ described an individual polyclinic visit, which could comprise of a single or multiple treatment modalities provided within the same encounter. A ‘treatment modality’ described the type of intervention or treatment provided by a particular discipline (e.g. soft tissue techniques, electrotherapy, manipulation, taping, etc.). A ‘provider discipline’ described a professional group with specific qualifications and who are recognised to practice in that field, such as physical therapy, osteopathy, chiropractor, and sports massage. Different disciplines could administer the same modality, such as manipulation techniques, which could be provided by a physical therapist, osteopath, or chiropractor, however each of these disciplines has their own treatment approach with variation in the application of the technique, providing skill mix and a multidisciplinary approach.
Cold-therapy TIIB (standard protocol at 10°C for a treatment duration of 10min)22–24 was provided as part of the services, but has been reported and analysed separately. As a new addition to previous Games,2,16 the EMR-system also required the reason for attendance to be recorded at the clinic's registration desk: (1) advice, (2) injury, (3) injury prevention, (4) maintenance, and (5) recovery. ‘Maintenance’, for instance, described an intervention that was aimed at supporting performance (excluding injury, recovery, advice, or prevention).
Information for all encounters were manually entered in Portuguese on a paper form, as required by Brazilian law.25 Encounters were then entered into the EMR-system using anonymised classification codes for each parameter. Only OCOG polyclinic encounters were recorded and analysed in the present study.
Confidentiality and ethical approvalIn accordance with the IOC Olympic Movement Medical Code1 the voluntary and informed consent was obtained from athletes for any medical intervention (inclusive of physical therapies) and the anonymisation of data to be used for research purposes.
The data collection system and recording criteria were approved by the OCOG Medical Advisory Group. The IOC Medical Code on athlete confidentiality was strictly observed.1
We used the athlete accreditation number to query the IOC athlete database for the age, sex, and nationality of the injured or ill athlete. We treated all information confidentially and deidentified our database after the Games. The study was approved by the Medical Research Ethics Committee of the South-Eastern Norway Regional Health Authority (2011/388), and OCOG medical advisory group.
Data analysis and statisticsData analysis was completed on OCOG physical therapy and physical therapies activities at the Olympic polyclinic only. Encounters were categorised by their accreditation status: athlete and non-athletes, sport, discipline visited (or provider), reason for visit, and treatment modalities received. Data are presented descriptively only, with frequencies and proportions (%).
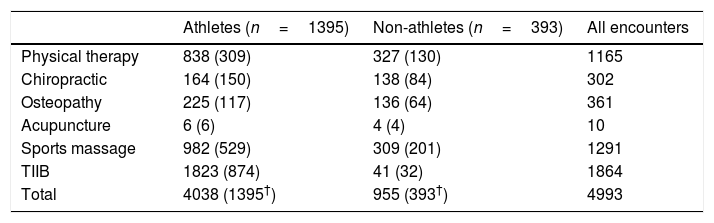
ResultsDuring the Rio 2016 Olympic Games, and across all services, there were 4993 encounters (4038 athlete and 955 non-athlete encounters) by 1788 accredited individuals (1395 athletes, 393 non-athletes). Of all encounters, 40% were for sports massage (982 athlete-encounters and 309 non-athlete encounters), followed by physical therapy (36%), chiropractic (12%), osteopathy (11%), acupuncture (0.5%). For 24 encounters, the provider discipline was unknown (Table 1). Overall, this equated to 12.4% of all competing athletes at the Olympic Games seeking treatment. The non-athlete group was comprised of NOC team officials (n=251, 63.9%), OCOG workforce volunteers (n=84, 21.4%), Olympic family members (n=38, 9.7%), press (n=10, 2.5%), and technical officials (n=8, 2.0%) (unknown n=2, 0.5%).
Frequency of encounters (and number of individuals) by provider's discipline for athletes and non-athletes.
During the Games, there was a gradual 2 peak build-up of athlete and non-athlete encounters: the first from the time of the opening of the Olympic Village to the start of the first day of competition ‘pre-competitionperiod’, and the second during the first week and a half of the ‘Olympic competitionsperiod’ (Fig. 1).

During the pre-competition period, there were on average 71 encounters per day. During the first week and a half of the competition, the busiest days were those from the 12th to the 16th August with an average of 162 encounters per day.
Distribution of cold-therapy TIIB encountersThere were a total of 1864 TIIB encounters reported between 28th Jul and 21st August, equating 1823 encounters (98%) in 874 athletes and 41 encounters (2%) in 32 non-athletes. The usage of TIIB peaked in the first week of the competition period.
Athlete encounters by discipline provider, sport, and treatment modalitiesThe 4032 treatments (excluding 6 acupuncture encounters) were administered during 1395 athlete encounters, illustrating that the majority of encounters were comprised of several different treatment modalities, administered in the same visit. This equated on average 2.9 treatments per athlete encounter. Physical therapy was the most utilised service, administrating 838 treatments in 309 athletes, equalling 2.7 encounters per athlete. Equivalent numbers for sports massage were 1.9 encounters per athlete, followed by osteopathy (1.9) and chiropractic with (1.1) encounters per athlete (Table 1).
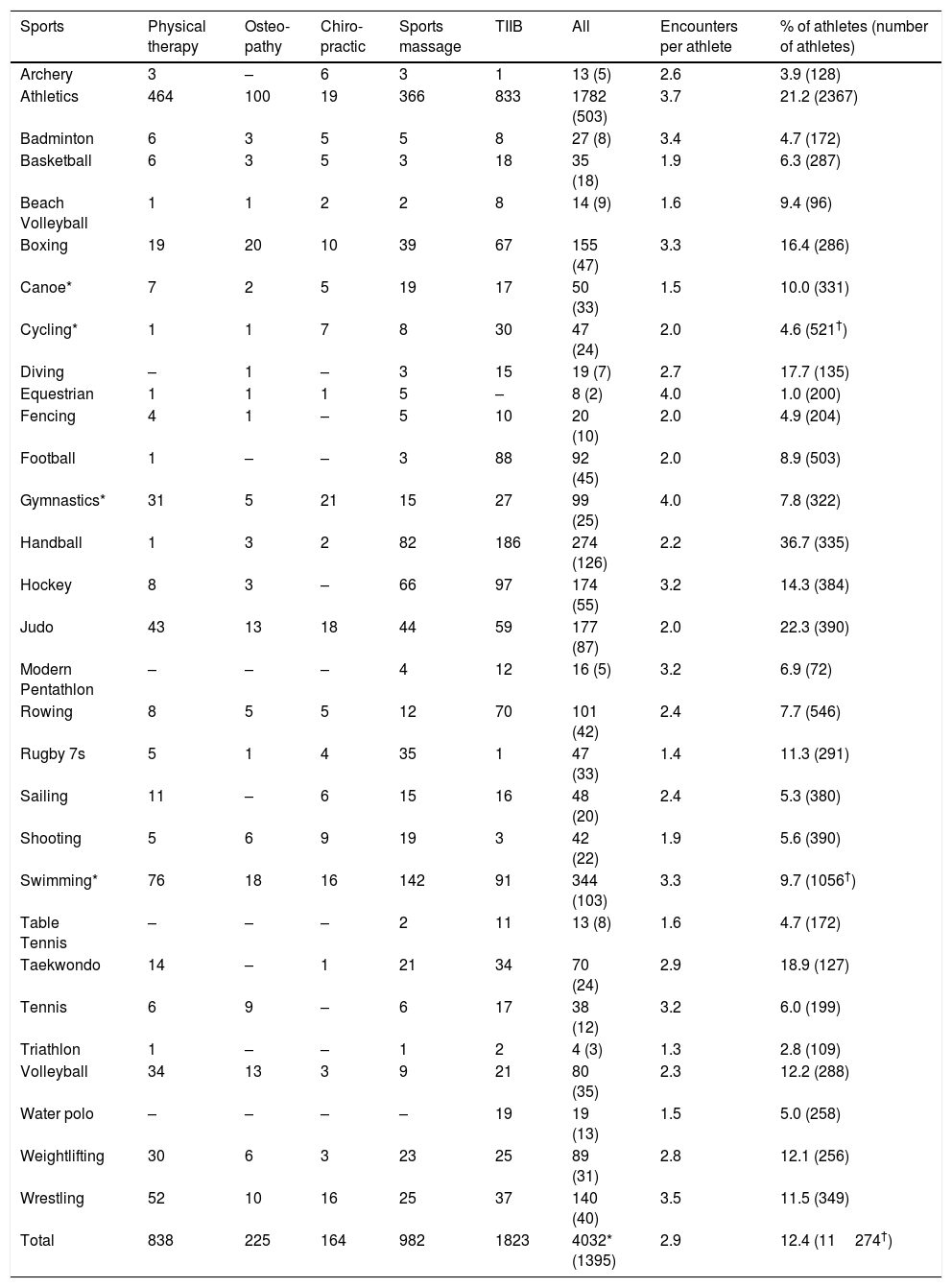
The sports using physical therapy, physical therapies, and multidisciplinary services most frequently were athletics (n=1782 encounters, accounting for 46% of all encounters) followed by swimming (including synchronised and marathon) (344, 8%), and handball (274, 7%). Comparing service use as a percentage of all athletes in their sport, handball (n=355 handball players, 37% of all handball players), followed by judo (390, 22% of all judo athletes), and athletics (2367, 21% of all track and field athletes) recorded the greatest usage. Sports recording the greatest use of sports massage services were primarily athletics followed by swimming and handball, and for TIIBs, athletics followed by handball and swimming (Table 2).
Frequency of athlete encounters (and number of athletes) by sport.
| Sports | Physical therapy | Osteo-pathy | Chiro-practic | Sports massage | TIIB | All | Encounters per athlete | % of athletes (number of athletes) |
|---|---|---|---|---|---|---|---|---|
| Archery | 3 | – | 6 | 3 | 1 | 13 (5) | 2.6 | 3.9 (128) |
| Athletics | 464 | 100 | 19 | 366 | 833 | 1782 (503) | 3.7 | 21.2 (2367) |
| Badminton | 6 | 3 | 5 | 5 | 8 | 27 (8) | 3.4 | 4.7 (172) |
| Basketball | 6 | 3 | 5 | 3 | 18 | 35 (18) | 1.9 | 6.3 (287) |
| Beach Volleyball | 1 | 1 | 2 | 2 | 8 | 14 (9) | 1.6 | 9.4 (96) |
| Boxing | 19 | 20 | 10 | 39 | 67 | 155 (47) | 3.3 | 16.4 (286) |
| Canoe* | 7 | 2 | 5 | 19 | 17 | 50 (33) | 1.5 | 10.0 (331) |
| Cycling* | 1 | 1 | 7 | 8 | 30 | 47 (24) | 2.0 | 4.6 (521†) |
| Diving | – | 1 | – | 3 | 15 | 19 (7) | 2.7 | 17.7 (135) |
| Equestrian | 1 | 1 | 1 | 5 | – | 8 (2) | 4.0 | 1.0 (200) |
| Fencing | 4 | 1 | – | 5 | 10 | 20 (10) | 2.0 | 4.9 (204) |
| Football | 1 | – | – | 3 | 88 | 92 (45) | 2.0 | 8.9 (503) |
| Gymnastics* | 31 | 5 | 21 | 15 | 27 | 99 (25) | 4.0 | 7.8 (322) |
| Handball | 1 | 3 | 2 | 82 | 186 | 274 (126) | 2.2 | 36.7 (335) |
| Hockey | 8 | 3 | – | 66 | 97 | 174 (55) | 3.2 | 14.3 (384) |
| Judo | 43 | 13 | 18 | 44 | 59 | 177 (87) | 2.0 | 22.3 (390) |
| Modern Pentathlon | – | – | – | 4 | 12 | 16 (5) | 3.2 | 6.9 (72) |
| Rowing | 8 | 5 | 5 | 12 | 70 | 101 (42) | 2.4 | 7.7 (546) |
| Rugby 7s | 5 | 1 | 4 | 35 | 1 | 47 (33) | 1.4 | 11.3 (291) |
| Sailing | 11 | – | 6 | 15 | 16 | 48 (20) | 2.4 | 5.3 (380) |
| Shooting | 5 | 6 | 9 | 19 | 3 | 42 (22) | 1.9 | 5.6 (390) |
| Swimming* | 76 | 18 | 16 | 142 | 91 | 344 (103) | 3.3 | 9.7 (1056†) |
| Table Tennis | – | – | – | 2 | 11 | 13 (8) | 1.6 | 4.7 (172) |
| Taekwondo | 14 | – | 1 | 21 | 34 | 70 (24) | 2.9 | 18.9 (127) |
| Tennis | 6 | 9 | – | 6 | 17 | 38 (12) | 3.2 | 6.0 (199) |
| Triathlon | 1 | – | – | 1 | 2 | 4 (3) | 1.3 | 2.8 (109) |
| Volleyball | 34 | 13 | 3 | 9 | 21 | 80 (35) | 2.3 | 12.2 (288) |
| Water polo | – | – | – | – | 19 | 19 (13) | 1.5 | 5.0 (258) |
| Weightlifting | 30 | 6 | 3 | 23 | 25 | 89 (31) | 2.8 | 12.1 (256) |
| Wrestling | 52 | 10 | 16 | 25 | 37 | 140 (40) | 3.5 | 11.5 (349) |
| Total | 838 | 225 | 164 | 982 | 1823 | 4032* (1395) | 2.9 | 12.4 (11274†) |
Data on acupuncture data (n=6 athletes) not included. TIIB, total immersion ice baths.
Soft tissue and electrotherapy treatment modalities were most frequently used, accounting for 1015 (31%) and 923 (28%) administered treatments, respectively, followed by manipulation and mobilisation techniques (n=685, 21%). While electrotherapy and soft tissue therapy were the most administered treatment modalities for physical therapists, manipulation techniques and soft tissue therapies were most commonly administered for chiropractors and osteopaths (Fig. 2).
Athlete reason for polyclinic attendance
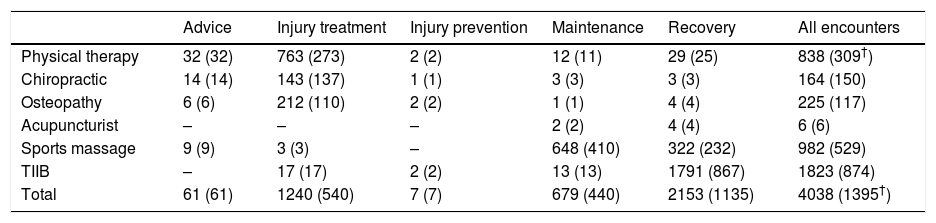
For all four provider disciplines, as well as for TIIB, the primary reason for athlete attendance was recovery (52% of all encounters), followed by injury treatment (30%), maintenance (16%), advice and evaluation (1.5%), and injury prevention (0.5%) (Table 3).
Frequency of athlete encounters (and number of athletes) by reason for encounter and provider discipline.
| Advice | Injury treatment | Injury prevention | Maintenance | Recovery | All encounters | |
|---|---|---|---|---|---|---|
| Physical therapy | 32 (32) | 763 (273) | 2 (2) | 12 (11) | 29 (25) | 838 (309†) |
| Chiropractic | 14 (14) | 143 (137) | 1 (1) | 3 (3) | 3 (3) | 164 (150) |
| Osteopathy | 6 (6) | 212 (110) | 2 (2) | 1 (1) | 4 (4) | 225 (117) |
| Acupuncturist | – | – | – | 2 (2) | 4 (4) | 6 (6) |
| Sports massage | 9 (9) | 3 (3) | – | 648 (410) | 322 (232) | 982 (529) |
| TIIB | – | 17 (17) | 2 (2) | 13 (13) | 1791 (867) | 1823 (874) |
| Total | 61 (61) | 1240 (540) | 7 (7) | 679 (440) | 2153 (1135) | 4038 (1395†) |
Athletes reported injury as the main reason for physical therapy visits (92% of all encounters and 2.8 encounters per athlete), chiropractic (94% and 1.9), and osteopathy (91% and 1.8) treatment. Conversely, the majority of TIIB visits were made by athletes for recovery purposes (98% of all TIIB encounters; 2.1 encounters per athlete). For sports massage, the primary reason for attendance was maintenance (66% of all massage encounters, 1.6 encounters per athlete), followed by recovery (33%, 1.4 encounters per athlete).
DiscussionThe present study is the first to our knowledge to evaluate the activity of the entire multidisciplinary physical therapies team and to provide a more in-depth understanding of athlete reliance on each discipline provider, including their reasons for seeking treatment during a major sporting event. In addition, this study provides a more in-depth understating of the usage of total immersion cold baths during an Olympic competition. Over the 32 opening days, 1 in 8 athletes (12.4%) utilised the polyclinic services, mostly from athletics, swimming, handball, and judo. Of all disciplines, physical therapy and sports massage were most frequently used. Physical therapy, chiropractic, and osteopathy were primarily requested for injury treatment, with cold-therapy TIIB most frequently used for recovery.
Distribution of physical therapies encounters, including TIIBSimilar to previous Games,2,16 there was a bi-modal distribution of service use with a gradual build-up of all encounters from the time of the opening of the Olympic Village to the first days of competition, and again during the first week and a half of competition. These patterns of activity are important to understand to optimally plan and coordinate staffing and facilities for future Games.
Athlete utilisation of the Olympic polyclinic services has grown significantly over the past decade,2,6,25–30 and utilisation at the Rio 2016 Games was higher than that reported in any previous Olympic Games,25,28,29 with a total of 4993 individual encounters for all therapies recorded (4038 athlete encounters, 81%). For physical therapy and multidisciplinary therapies (only), 72% of all encounters in Rio were by athletes, and 28% by non-athletes. The Athens Olympics16 recorded that 75% of the 457 physical therapy and sports massage encounters were for athletes, while in London2 there was a total of 1778 physical therapy encounters with 1219 of those (69%) for athletes. Hence, while athletes continue to predominate Polyclinic usage, it is necessary to allow for approximately 20–30% of physical therapy and physical therapies service provision for non-athletes.
In Rio, a total of 11 ice baths were available in the main treatment area of the polyclinic and their use accounted for 43.8% of all athlete encounters. In London in 2012,2 ice-baths accounted for only 10% of all athlete treatments, similar to in Athens in 2004 (9%).16 Recent literature31 suggests total immersion ice baths are more beneficial than passive recovery in the management of post exercise muscle soreness,32 and there has been an increase in demand for TIIB.32–36 The Rio Olympic Games service provision aimed to meet this demand, and this was positively reflected by increased uptake.
Encounters by discipline providerFor physical therapies services only, overall sports massage (40% of all encounters), followed by physical therapy (36%) were the most utilised discipline providers during the Rio Games for both athletes and non-athletes.
Previous publications on multisport events have reported solely on physical therapy and massage activities.2,13–17 Considering physical therapy encounters only, there was a slight decrease in utilisation during the Rio Games compared with London in 2012.2 While a significant reliance remains on physical therapy,2,16 increases in overall uptake of all physical therapies were possibly due to a greater dedicated level of service provision (e.g. TIIB), and the access to disciplines such as chiropractic, osteopathy, and sports massage. These results illustrate the inclusion of a multidisciplinary service offering a greater skill-mix to the athletes requirements.7,9–11,36
Athlete encounters by sportOf the 41 sports represented in the 2016 Rio Games, athletes from 30 sports used the multidisciplinary service. Athletes from handball (37% of all handball athletes), followed by judo (22%), athletics (21%), and taekwondo (19%) presented the largest user group. These numbers mirrored injury incidence data from the Rio 2016 Injury and Illness Surveillance study with these sports being in the top 20% of reported injuries.12
Athlete treatment modalitiesSoft tissue manual therapy and electrotherapy treatments were most commonly used by all disciplines followed by manipulation and mobilisation techniques, frequently used in the treatment of soft tissue and joint related injuries.37–42 Compared with other disciplines, physical therapists administered most electrotherapy and soft tissue modalities. In addition, physical therapists provided the broadest spectrum of skills in terms of delivery of different types of treatment modalities. Demonstrated by the number of treatment modalities administered per encounter (2.7 treatments per physical therapy encounter), using more than one modality was considered to be a preferred treatment approach.43–45
Compared with the London 2012 Olympic Summer Games,2 there was higher usage of electrotherapy in Rio 2016, but conversely, lower compared to Athens in 2004.16 These trends perhaps reflect a change in treatment approach as the scientific evidence evolves, as well as host nation philosophies towards treatment. Hence the question that continues to be debated in the literature remains, which modalities are the most effective.36,37,40,42,45
Athlete reason for attendanceRecovery and ‘treatment of injury’ were the most common reasons for polyclinic attendance by athletes in Rio 2016. While earlier studies have reported injury treatment as the only reason for athlete attendance,2,8,12–17,28–30 the present study provides more detailed previously unreported information on the athletes’ diverse needs of the multidisciplinary services. Here, injury treatment represented 30% of athletes’ primary reason to enter the polyclinic, second to recovery (52% of all encounters). This analysis demonstrates the evolving and expanding role of physical therapies as part of the healthcare team who care for the athlete.
There was a strong reliance on TIIBs to support the recovery process by athletes in the present study, similar to previous studies where it has been used as a primary recovery intervention.32–36 The facilitation of TIIBs is an area that should be included in athlete service provision at future major Games events.
Methodological considerations, strengths, and limitationsAs an advancement from previous Olympic Games,2,16,17 the present study included recording of the integration of a multi-skillset team for athlete (and non-athlete) treatments, and athlete‘s reason for clinic attendance. It has been recognised in recent years that athletes do not always seek physical therapies for treatment of injuries, but also for assistance with sports performance, and more increasingly for recovery during the time of peak competition.2–5,36 This is further supported by data presented in this study.
Compared to previous Games, the EMR-system allowed for recording up to four separate treatment modalities in one encounter. The expanded functionality additionally supported the entries of more detailed information on the multifaceted and multidisciplinary nature of athlete treatments. In light of no previous studies documenting the multidisciplinary services, incorporating physical therapists, osteopaths, chiropractors, and sports massage practitioners working as a team, the Rio Olympic physical therapies services suggest that a multidisciplinary team incorporating several disciplines increases the level of care offered to the athlete.
As a limitation, data on athlete injury (anatomical area, diagnoses, onset, and cause) were unavailable due to logistical challenges with Polyclinic data entry. While these data were available for the Rio 2016 Injury and Illness surveillance study,12 mandating these data in physical therapies records in the future may provide additional information on athlete treatment requirements.
Also, only OCOG polyclinic encounters were collected in the present study. Hence, it is important to consider and further understand the treatment needs of athletes at medical stations at competition venues and on the field of play. Finally, it may also be interesting to know if the athletes’ needs and requests are similar to those needs provided within the athlete's NOC clinical team.
ConclusionDuring the Rio 2016 Olympics, over the 32 opening days, 1 in 8 athletes (12.4%), mostly from athletics, swimming, handball, and judo, utilised the polyclinic services. Of all disciplines, physical therapy and sports massage services were most frequently used by athletes and were primarily requested for injury treatment, while cold-therapy TIIBs was most frequently used for recovery. These results provide new insights on athlete needs and can help to inform physical therapy and physical therapies service provision planning for future major sporting events.
Conflicts of interestThe authors declare no conflicts of interest.
We would like to acknowledge the contribution and support of the Rio 2016 Physiotherapy and Physical Therapies multidisciplinary for contributing to the data collection: in particular our thanks to Mr. Felipe Tadiello (lead physical therapist Rio 2016) and his senior physical therapy team: Christiane Macedo-Londriana, Leonardo Medeiras, Lucina De Nichelis, Márcio Costa Antonelo, and Marco Antonio Ferreira Alves.



