

Physical activity (PA) has many health benefits. However, more research is needed to understand its effects on mortality risk in older adults.
ObjectiveTo verify the hypothetical effects of replacing sedentary behavior (SB) and PA domains on the risk of mortality in the older adults.
MethodsA population-based prospective cohort study was conducted using exploratory survey methods, involving 332 participants of both sexes aged ≥ 60 years monitored over five years. PA and SB were assessed using the International Physical Activity Questionnaire, with the domains assessed including leisure, occupational, transport, and domestic. Isotemporal replacement modeling was applied to examine the hypothesized effects of replacing the PA and SB domains on mortality risk, using Cox proportional hazards regression with Hazard Ratio estimates and 95 % confidence intervals.
ResultsAt all time points tested in the model, replacing SB exposure time with leisure-time PA proved to be protective against mortality risk, while the opposite substitution of leisure-time PA with SB was associated with higher mortality risk among participants.
ConclusionThis study suggests implementing strategies, highlighting the importance of promoting leisure activities among the older adult population.
The practice of physical activity (PA) is essential for promoting health and well-being, as it is associated with numerous benefits, including reduced risk of chronic diseases like cancer and cardiovascular disease, improved cognitive function, decreased depressive symptoms, and lower mortality.1–4 These health benefits are widely recognized by global health organizations, which have established guidelines to encourage physically active lifestyles.5,6
However, despite evidence of the benefits of PA and ongoing efforts to promote its regular practice, it has been observed that the Brazilian population between 55 and 64 years of age has a prevalence of physical inactivity of ∼49 % and for those over 65 years of age of ∼63 %,7 opting for a more sedentary lifestyle.8 Sedentary behavior (SB), characterized by activities such as sitting or reclining with energy expenditure ≤1.5 METs,9 is associated with adverse health outcomes,10 including increased mortality risk and reduced life expectancy.11,12
Addressing the challenge of promoting behavior change in older adults requires exploring strategies that effectively enhance health and well-being. In this sense, isotemporal modeling11,13,14 emerges as a promising approach that, through a widely used mathematical model, provides insights into how the reallocation of time devoted to SB to different domains of PA15–19 can influence health and longevity, through a widely used mathematical model, test the most effective way to reduce harmful health risks, and help to develop more insightful strategies to improve health and longevity.20–23 Behaviors are known to be synergistic, and increasing or decreasing one behavior can directly affect the exposure time of the other.11,24
Recent scientific literature shows an association between the practice of PA, especially that performed during leisure time, and the health of the older adult population.15,16,18 However, the relationship between PA in the occupational context and health outcomes is still the subject of debate, with studies indicating both beneficial and harmful effects depending on the intensity and duration of the activity,16,25–27 while in other contexts and domains it is still unclear, but worse, a certain positive influence on mortality risk between the transport and domestic domains. This ambiguity highlights the need for more in-depth research that can elucidate the nuances of the relationships between the different domains of PA and their specific impacts on health and mortality in older adults.
Therefore, the aim of this study was to examine the potential effects of replacing time spent on SB with PA in different domains on mortality risk in Brazilian older adults. We hypothesized that such a substitution could lead to a significant reduction in mortality risk, thus reinforcing the importance of PA as a key determinant of health and longevity in old age. This study will not only contribute to the understanding of the relationship between PA, SB, and health in the older adult population, but will also provide valuable evidence for the development of public policies and interventions aimed at promoting active and healthy lifestyles among older adults.
MethodsStudy designThis study is characterized as a population-based prospective cohort, part of the Estudo Longitudinal de Saúde do Idoso de Alcobaça–BA (ELSIA), using exploratory survey methods.
Ethical proceduresThe study protocols and procedures were conducted in accordance with the Declaration of Helsinki. Prior approval was obtained from the Ethics Committee for Human Research of the Federal University of Triângulo Mineiro (ordinance 966.983/2015) and the State University of Bahia (ordinance 3.471.114/2020). All participants provided signed informed consent.
ParticipantsInitially, the study population consisted of 743 older adults, aged 60 years or older, registered with the Family Health Strategy (FHS) in the municipality of Alcobaça, located in the extreme south of the state of Bahia, Brazil. Following home visits based on information provided by the FHS team, the older adults were invited to participate in the study, and details of the study procedures and objectives were provided.
Participants with severe cognitive impairment on the Mini-Mental State Examination (≤ 11 points), adapted for the Brazilian population,28 were excluded, as were those with severe difficulty in visual and/or other sensory functions, those using wheelchairs, with severe sequelae of cerebrovascular accident (CVA) with localized loss of strength, and those with terminal illness. The final sample of the first wave, conducted between June and September 2015, consisted of a total of 473 older adults aged 60 years or older (297 women and 176 men).
Of the participants included in the first wave of the study, 105 could not be located and 36 changed cities, for a total of 141 segment losses. Of the 332 returns received, 59 were deceased and 273 were alive. The second wave took place from January to February 2020. More information is available elsewhere,3,11 and in Fig. 1. In our study, we tested the assumption that the participants were lost to follow-up as if they were still alive and observed no change in the estimates (data not shown).
Mortality
Vital status was determined through telephone follow-up, information obtained from family members presenting the death certificate, data retrieved from the Municipal Registry Office (Registry Office of the RCPN of Alcobaça), and/or public consultation of the website of the Court of Justice of the State of Bahia. To calculate the survival time, the follow-up time from the beginning of the survey until death, censoring, or the end of the second wave (February 29, 2020) was used.
Physical activity and sedentary behaviorLevels of PA and duration of SB were assessed using the International Physical Activity Questionnaire (IPAQ), which has been validated in Brazilian older adults.29,30 PA was assessed on the basis of moderate-to-vigorous intensity activities (MVPA) performed for at least 10 consecutive minutes, assessed in the domains of leisure, work, transportation, and household activities, with presenting a reproducibility of 0.77 for women and 0.95 for men, both by Spearman’s correlation. Compared with the pedometer, the Kappa index values are 0.27 and 0.19 and Spearman’s correlation values are 0.27 and 0.24, respectively, for women and men. Likewise, compared with the PA Diary, the Kappa index values are 0.34 and 0.04 and Spearman’s correlation scores are 0.54 and 0.38, respectively, for women and men.29,30
SB was determined by time spent sitting, as assessed by questions about time spent in a seated position. Total sedentary time in minutes per day was calculated as the weighted average of sedentary time on a weekday and a weekend day: [(sitting time on a weekday x 5+sitting time on a weekend day x 2)/7], determined at Baseline.
Sleep assessmentNighttime sleep duration was measured using a specific question from the Pittsburgh Sleep Quality Index, validated for Brazilians (PSQI-BR).31 The question asked was: "During the last month, how many hours of sleep did you get each night?" The obtained time value was included in the total duration of activities during the day without replacement in the model, determined at Baseline. Showing significant correlations (r = 0.881; CCI=0.878; p < 0.001) between scores of the PSQI-BR and of the original PSQI, indicating a good linguistic interchangeability between the translation and the original questionnaire and an overall reliability coefficient (Cronbach’s α) of 0.82, indicating a high degree of internal consistency.31
CovariablesThe covariates included in the model were sex (male and female), occupation (retired and working, retired, homemaker, pensioner, paid work), age, income, and the number of diseases (absolute numbers). The number of diseases was obtained through self-reporting, based on the sum of various diseases identified from a list according to CID-10, including: heart problems, high blood pressure, stroke, asthma/bronchitis, rheumatism/arthritis/arthrosis, back/low back pain, osteoporosis, type 2 diabetes mellitus, cancer and kidney problems (kidney stones and urinary tract infections),32 determined at Baseline.
Data analysisThe creation of the database underwent a double data entry process, utilizing the Epidata program (Epidata Association, Odense, DK/Fiona, Denmark), version 3.1b The analyses were conducted using the IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, N.Y., USA).
Descriptive statistical techniques were used to examine the sample, including measures of dispersion (standard deviation and interquartile range), absolute and relative frequency calculations, and measures of central tendency (mean and median). Normality was assessed using the Kolmogorov-Smirnov test. The chi-squared test and the Mann-Whitney U test were used to compare vital status with respect to covariates. In addition, the Mann-Whitney U test was used to compare daily activity times by vital status.
The isotemporal substitution model was employed to explore the theoretical implications of substituting one behavior for another. In this analysis, the time spent on the observed activities was divided by a constant (unit of time) to examine the effect. Subsequently, a new variable was created, encompassing the sum of the time spent on all activities. The activity intended for observation regarding the consequences of replacement was excluded from the model, while all other activities, including the total discretionary time constant, remained in the model.13 This is presented in the equation below, with the removal of the time spent on SB from the model:
To examine the hypothetical consequences of replacing the domains of PA, SB, and sleep (kept constant in the model) on the risk of mortality, Cox proportional hazards regression was utilized, with estimates of Hazard Ratio (HR) and corresponding confidence intervals (95 %CI). The model was adjusted for sex, age, income, and the number of diseases. Replacement times of 10, 20, 30, 40, 50, and 60 min were tested. Prior to the isotemporal analysis, all proportional hazards assumptions were evaluated, and no violations were observed. The proportional hazards assumption for each prognostic factor was assessed visually under each model using log-log plots, and tested analytically using Schoenfeld residuals. A significance level of 5 % was adopted.
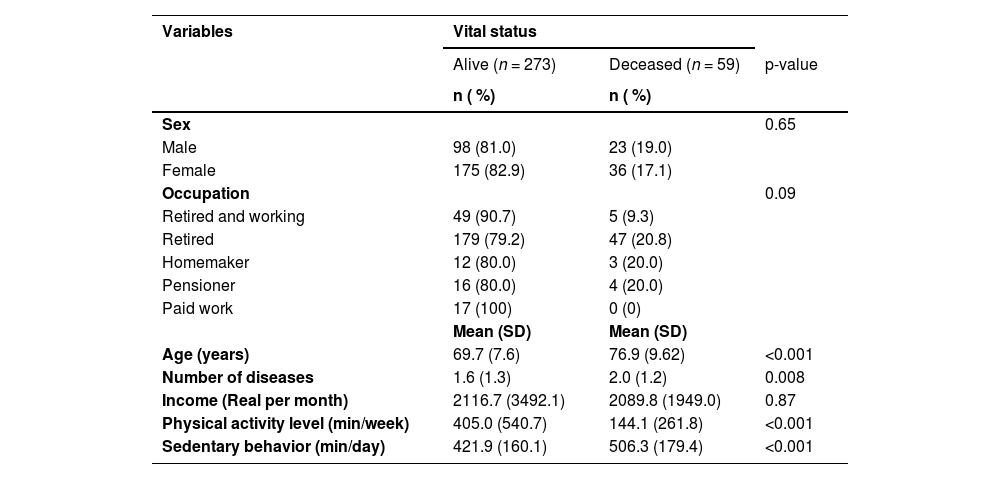
ResultsOf the 332 study participants, the majority were female (63.6 %) and retired (68.1 %), the average age was 71.0 years (SD 8.5 years), the total loss in the segment was ∼30 %, other descriptive information is described in Table 1.
Characteristics of participants according to vital status.
SD: Standard deviation.
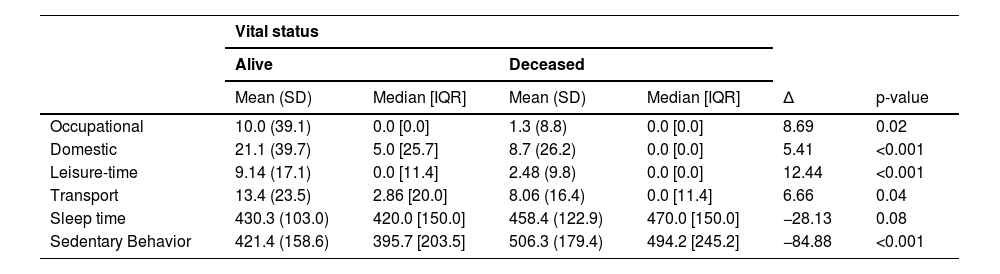
The daily average times of the activities included in the Isotemporal model were 8.47 min/day (SD 1.96 min/day) of occupational PA, 18.94 min/day (SD 2.08 min/day) of domestic PA, 7.95 min/day (SD 0.89 min/day) of leisure-time PA, 435.00 min/day (SD 107.00 min/day) of sleep, and 436.50 min/day (SD 9.08 min/day) of SB. Table 2 presents the mean times, median, standard deviation, interquartile range, and deltas according to vital status.
Daily time in minutes of activities included in the isotemporal model.
SD: Standard Deviation; IQR: Interquartile range; ∆: Average difference.
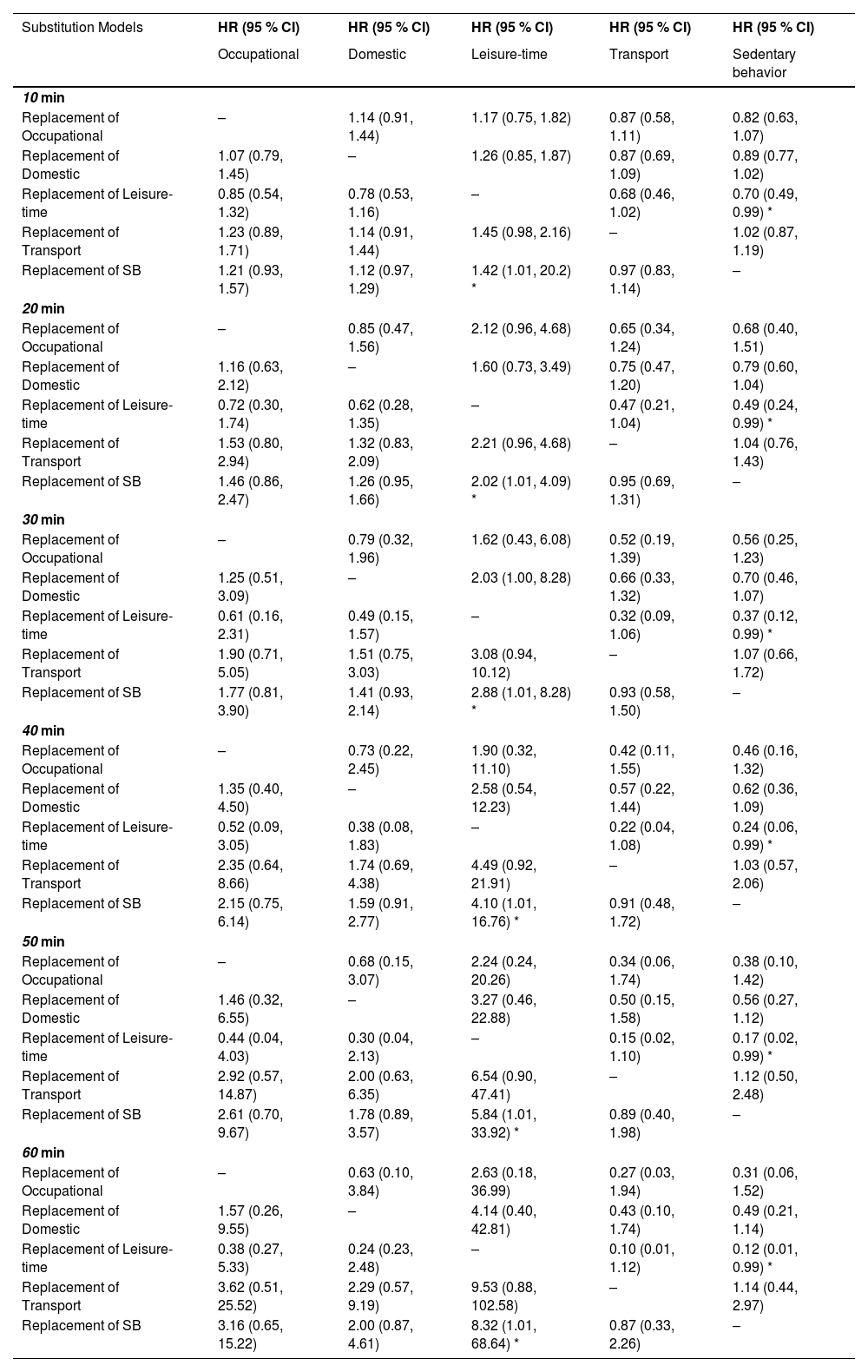
The isotemporal substitution model is presented in Table 3. At all times tested in the model, replacing the time of exposure to SB with PA in the leisure domain proved to be a protective factor for the risk of mortality among participants. Conversely, the inverse replacement was demonstrated to be a risk factor for mortality, with risks varying between HR=1.42 (95 %CI: 1.01, 20.2) for 10 min and HR=8.32 (95 %CI: 1.01, 68.64) for 60 min, suggesting an increase in mortality risk with increasing time.
Isotemporal substitution model of the association between time reallocation in sleep, sedentary behavior, and physical activity domains, and mortality risk in older adults.
CI, confidence interval; HR, Hazard Ratio; SB, sedentary behavior. Adjusted for sex, age, income, and number of diseases. *p < 0.05.
Our main objective in this study was to verify the hypothetical effects of replacing SB exposure time and PA domains on the risk of mortality in older adults. We observed that reallocating sedentary time to an equivalent duration of PA in the leisure domain reduced the risk of mortality in older adults by 30 % to 78 % for reductions of 10 min and 60 min, respectively. Conversely, opposite substitutions, reducing leisure time and increasing sedentary time, increased the risk of mortality. Therefore, although we did not observe a reduction in mortality risk when substituting sedentary time across all domains of PA, we can confirm our study hypothesis.
The implications of our results are manifold and echo existing literature highlighting the health benefits of regular PA for older adults in reducing mortality risk.3,4,33,34 In addition, the model's emphasis on isotemporal substitution provides a new perspective for examining the relationship between different types of activity and health outcomes. It suggests that not only increasing PA, but also reducing sedentary time, is critical for health, particularly among older adults. This dual approach is consistent with the World Health Organization guidelines, which advocate both increasing PA and reducing sedentary time to improve health outcomes.5
In our study, replacing SB time with leisure-time PA was shown to reduce the risk of mortality in older adults, as demonstrated in other studies.15,16,18 Arem et al.15 compared mortality risk in relation to leisure-time PA and found that meeting the proposed PA recommendations (7.5 to <15 MET h/week) reduced mortality risk by ∼31 %. However, increasing this time in search of additional benefits showed a ceiling effect when performing between 3 and 10 times the recommended amount (22.5 to <75 MET h/week), resulting in a 39 % reduction in mortality risk. In other words, leisure time appears to contribute to a reduction in mortality risk, thereby increasing population survival.
Although our study did not show an association between the duration of occupational PA and mortality risk, other studies have shown trends in these variables.16,25–27 They suggest that longer duration or higher intensity of occupational PA may increase mortality risk.26,27 In addition, longer periods of occupational PA are associated with a higher risk of disability leave.35 However, some studies have failed to find an association with mortality, possibly due to factors such as intensity and sex.17,36
Possible mechanisms explaining the associations between health outcomes and the domains of occupational and leisure-time PA are discussed by Holtermann et al.37 The authors note that leisure-time PA typically involves high-intensity, short-duration, dynamic activities with ample recovery time, whereas occupational PA tends to be moderate to low-intensity, prolonged, and involves static movements with limited recovery. However, the lack of association in our study may be due to the low participation in occupational PA among the older adult participants, as the majority are retired or not in paid employment.
Furthermore, it is important to emphasize that leisure-time PA is not only more intense, but also often associated with a greater sense of enjoyment, satisfaction, and subjective well-being. This makes the transition from time spent on SB to leisure-time PA potentially easier compared to other domains of PA.38,39 This observation is particularly relevant in the occupational context, where interventions and promotion of PA may be more effective if specifically targeted at the leisure domain. Therefore, understanding and mastering intervention strategies that promote participation in leisure-time PAs may be a valuable tool for health and disease prevention professionals.
Because work is an inescapable aspect of human life, a recently published systematic review sought to investigate whether leisure-time PA might have beneficial effects in workers with different levels of leisure-time PA.40 The review observed that in individuals with low levels of occupational PA, increased leisure-time PA conferred protective effects. However, these effects were not observed in workers with moderate or high levels of occupational PA.40
In contrast to PA, SB is consistently associated with health risks, including a higher risk of mortality.3,11,34 Our study revealed that replacing leisure-time PA with sedentary time increased the risk of mortality. Galvão et al.11 observed a 35 % increased risk of mortality when replacing 30 min/day of moderate-to-vigorous PA with the same amount of sedentary time, with this risk potentially increasing to 82 % when replacing 60 min/day. Reducing sedentary time in favor of PA, regardless of intensity, may reduce mortality risk.34
In addition to total sedentary time, several specific domains of SB have been associated with increased mortality risk.41,42 For example, each additional 30 min of screen time per day is associated with a 1 % increased risk of mortality.41 These findings underscore the significance of not only assessing the total sedentary time but also investigating different SB and their individual consequences on health and longevity.
Although we did not include sleep duration in our analyses because we consider this to be adequate in the older adults studied, we recognize its importance in mortality risk. Currently, the ideal amount of sleep is approximately seven hours per night.43,44 Studies have shown that individuals with chronic diseases who sleep less than seven hours or >10 h have an increased risk of cardiovascular events, with risks increased by 42 % and 85 %, respectively.43 In another cohort of Asian participants, also using the seven-hour sleep reference point, the risk of mortality was increased in participants with less than five and more than eight hours of sleep per night.44 Therefore, individuals with irregular sleep patterns are at increased risk of mortality.
Given that the day is limited to 24 h, behaviors must be directed to maximize efficiency and obtain the greatest benefit, with the ultimate goal of increasing longevity and reducing the risk of mortality. This notion is supported by an accelerometer-based cohort study of >92,000 participants with an average age of 62 years.45 The results show that regular PA reduces the risk of mortality associated with sleep patterns that are considered detrimental to health.45
PA practice in the transport domain may be associated with a lower risk of mortality, as shown in a cohort study of 10,853 individuals with a mean age of 47.9 years and non-alcoholic fatty liver disease. However, these benefits seem to be more pronounced in individuals who practice more activity in this domain (>299 min/day), as well as in the leisure domain. On the other hand, practicing activity in the occupational domain seems to have no effect on mortality risk.21
This finding corroborates a cohort study carried out on the population of Peru, which included 3601 people with an average age of 55.8 years. The participants were divided into two groups according to their PA in transport: a group with less PA and a group with more PA. It was found that participants who were physically active in this area had a 42 % lower risk of death than those who were less active.46 Although we didn't observe reduction in mortality risk in this transport domain in our older participants, this difference could be due to our subjective assessment method, the sample size or the short period of practice in this domain.
The practice of PA in the domestic sphere can be confused in some cases with the practice in the work sphere, to the extent that in many cases it becomes something obligatory rather than enjoyable. In addition, a certain level of effort in this practice may reduce the risk of mortality.22,23 When evaluating the Italian population, mortality risks were only reduced among men with moderate PA practice in the domestic domain, compared to those who do not practice, and no associations were observed between those with low or high practice time in this domain, nor among female participants.23 This is supported by another study involving the Taiwanese population, which found only positive associations with moderate PA practice in the domestic domain.22 However, PA in the home domain appears to be associated with a lower risk of accelerated aging although it does not always reduce the risk of all-cause respiratory or cardiovascular mortality in participants with chronic obstructive pulmonary disease over 40 years of age.22,23,47
Our study has limitations, including the use of self-reported measures, which may introduce recall bias. However, we mitigated this issue through prior training of the data collection team. Additionally, we experienced a segment loss of ∼30 % of the sample. Furthermore, while the isotemporal substitution model is widely accepted and disseminated, it remains a hypothetical mathematical model, and its findings may not fully reflect real-world consequences of substitutions. Moreover, the low distribution of PA across specific domains may compromise interpretations. Small number of events and limited sample size. Therefore, future studies should address these evidence gaps and explore relationships between specific SB, such as screen time on TV, computer, or mobile phone, to elucidate more complex associations between behavioral substitutions.
As strengths, we highlight the use of a representative sample with a five-year follow-up period, located in a city with a low human development index within a developing country. In addition, our study used specific domains of PA practice, recognizing that each domain may have different effects on outcomes. For example, leisure-time PA has been shown to reduce mortality risk.
Public policy should prioritize the promotion of regular PA, particularly among older adults, with a focus on leisure-time activities. The large body of evidence supporting the benefits of leisure-time PA in reducing the risk of mortality and adverse outcomes underscores the importance of such initiatives. Specific activities such as tennis, soccer, and cycling have been shown to increase life expectancy by 9.7, 6.2, and 3.7 years, respectively.48
In our isotemporal replacement model, a significant reduction in mortality risk was observed in older adults during a five-year follow-up period when sedentary time was replaced for the same amount of leisure-time physical activity. Conversely, the opposite substitution, reducing leisure time and increasing sedentary time, increased the risk of mortality.
Declaration of generative AI and AI-assisted technologies in the writing processDuring the preparation of this work the author(s) used ChatGPT from OpenAI to assist in translating this article. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
The authors declare that they have no competing interests.
We would like to thank all the participants who made their time available to take part in the study. This study was partly funded by the National Council for Scientific and Technological Development (MCTI/CNPQ/Universal 14/2014, grant number: 448184/2014–1) and supported by the Coordination for the Improvement of Higher Education Personnel - Brazil (CAPES).



