

Shoulders of elite field hockey players are loaded continuously during play. Frequent high shoulder loading is known to influence certain shoulder variables, such as acromiohumeral distance. However, the influence of elite field hockey play on acromiohumeral distance is not examined yet.
ObjectiveTo examine the acromiohumeral distance in elite male field hockey players compared to a non-athletic control group.
DesignCross-sectional study.
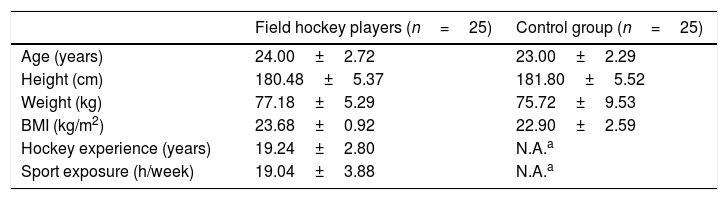
MethodsFifty male participants were included; 25 elite field hockey players (age: 24.0±2.72 years; weight: 77.2±5.29kg; height; 180.5±5.37cm) and 25 age- and gender matched non-athletes (23.0±2.29 years; weight: 75.7±9.53kg; height: 181.8±5.52cm). A Telemed-Colormaster-128 EXT-IZ device was used to bilaterally obtain ultrasound acromiohumeral distance images at 3 different angles of shoulder abduction in the frontal plane.
ResultsField hockey players showed a bilateral larger acromiohumeral distance at 45° (mean difference: 1.46mm [95% CI 0.46; 2.46]; p=0.005) and 60° (mean difference: 1.07mm [95% CI 0.21; 1.93]; p=0.016) compared to controls. In both groups, a significant but clinically less relevant, side difference was established for the acromiohumeral distance at 60° (mean difference: 0.79mm [95% CI 0.21; 1.34]; p=0.009).
ConclusionWith active shoulder abduction, elite field hockey players show a larger acromiohumeral distance in comparison to non-athletic participants. This may be a protective sport-specific adaptation, to better guard the shoulder from injury. Thus, acromiohumeral distance measurement may help physical therapists/coaches decide which athletes could benefit from specific, additional exercises aimed at enlarging the subacromial space.
Field hockey is a high paced and intense team sport1 with an international popularity second only to soccer.2 Playing field hockey is physically demanding and the demands on the shoulder joint and girdle during play cannot be underestimated.3 Although field hockey is not considered an overhead sport, the shoulder is highly loaded during practice and competition.
Rotator cuff pathology is considered to be a principal cause of shoulder pain,4 particularly in athletes with repetitive overhead activities, such as throwing athletes,5 of whom shoulder loading during sport participation is known to be extremely high. Acromiohumeral distance (AHD) is a common investigated variable in these shoulder-loading athletes. It is the quantification of the size of the subacromial space6 and although under debate, is assumed to be clinically relevant since a reduction of this space is linked to possible mechanisms in the etiology of rotator cuff tendinopathy.6–8
Generally, it has been established that AHD varies with shoulder position and is greatest at rest, in a neutral shoulder position. Norm values range from 10 to 15mm in a healthy shoulder,9–11 with no systematic difference between the dominant and non-dominant shoulder in a non-athletic population.12 The source of this wide range may be due to interindividual variability or the variety of measurement protocols used.6 AHD reduces with shoulder elevation or abduction9,10 and is smaller in patients with rotator cuff tendinopathy compared to asymptomatic individuals.11,13–16 An AHD equal to or smaller than 6mm is considered the cut-off for an abnormal AHD, suggesting a clinically significant rotator cuff pathology.12,17 Maintenance of the subacromial space in the shoulder girdle is essential for normal shoulder function.
In shoulder-loading athletes, no uniform conclusions can be made concerning sport-specific adaptations of the AHD. While some studies found a significantly larger AHD on the dominant side compared to the non-dominant side in these athletes,10,18,19 the opposite result9,20,21 as well as no difference between sides22 has been concluded in other studies. Moreover, comparing shoulder-loading athletes to a non-athletic population, a smaller AHD in tennis players compared to controls has been recorded23 while a larger AHD was found in swimmers.24 Comparison of elite shoulder-loading athletes with recreational athletes, proved a larger AHD in the first group compared to the latter.10 Whether sport-specific adaptations in the shoulder joint also occur in field hockey players is yet to be studied. Since field hockey players do not load their shoulders in the exact same way as athletes practicing more conventional overhead sports, such as handball and tennis, the comparison with study results in these overhead athlete populations is not entirely suitable. However, field hockey players are allowed to make plays above shoulder height and thus use their shoulders in a wider range of abduction than conventionally suspected.
In contrast to the extensive shoulder-related research in throwing sports and in spite of the popularity of field hockey, limited research has been done within the population of field hockey players. The scarcity and heterogeneity of the executed research concerning field hockey injuries does not allow for comprehensive statements on this matter.25 According to the limited available research, lower limbs are the most affected in these athletes, with contusions, abrasions and sprains being the most common types of injury.25,26 However, the most severe injuries involve direct trauma to the upper limb and head or face. These upper limb injuries comprise 4.9–39.4% of all hockey injuries.26 Within the upper limb, the shoulder has been suggested to be a vulnerable joint, with a significant risk for traumatic shoulder injury during training and competition.3,27,28
Since susceptibility to shoulder injuries for field hockey players is not far-fetched and the demands of the shoulder are repetitive of nature and extremely high, especially in elite players, a better understanding of the field hockey shoulder is a logical goal to aspire. Therefore, the purpose of this study was to bilaterally examine AHD at different angles of shoulder abduction within a group of elite field hockey players and compare these measurements with an age-and gender matched control group of healthy individuals. It was hypothesized that the AHD would differ between athletes and controls, however, it was uncertain whether to expect this difference in favor of the athletes or the controls: comparing results of similar studies in other shoulder loading, athletic populations does not lead to conclusive conclusions regarding this matter.
MethodsParticipantsThe study sample consisted of 25 elite male field hockey players, all active members of the national field hockey team, and an age and gender-matched control group comprised of 25 non-athletic, healthy individuals who volunteered to participate in the study. The field hockey team was recruited through communication with their head coach and physical therapist, while the control group was recruited through the use of social media and direct communication with possible candidate participants.
Concerning the elite field hockey players, a prior history of shoulder complaints was not an exclusion criteria but no shoulder complaints were allowed at the moment of testing. Control participants were not allowed to practice shoulder loading activities for more than 3h/week. The experience of any shoulder complaints in the past 6 months led to their exclusion as well as having a history regarding any type of shoulder injury (shoulder dislocation, rotator cuff tear, etc.) or shoulder related intervention (shoulder surgery, shoulder rehabilitation, etc.).
All participants completed a questionnaire to gather demographic, sport specific and shoulder specific information. Prior to their participation, all participants read and signed an informed consent form. The study was approved by the Ethical Committee of Ghent University, Ghent, Belgium (approval number: B670201523201).
Testing proceduresBefore the measurements initiated, all participants were informed about the testing procedure which consisted of 3 bilateral AHD measurements. The procedure was based on the protocol used in the study of Maenhout et al.9 All measurements were conducted by the same researcher, who received ultrasound training by the lead author of the article9 on which the procedure of this study was based (AM). A training period of 12 weeks was completed, in which the AHD measurement was practiced and repeated extensively, prior to the start of the testing.
Ultrasound images were collected with a Colormaster 128 EXT-IZ device (Telemed UAB, Vilnius, Lithuania) with a 5–10MHz linear transducer (HL9.0/40/128Z) and the Echo Wave II software (version 1.36; Telemed UAB). The participant was positioned seated on a stool, feet flat on the floor and instructed to not sag lumbarly. If necessary, the sitting position was corrected by the researcher through tactile correction at the lower back to restore the physiological lumbar lordosis. The anterior angle of the acromion was marked before the start of the measurements. Images were taken at 0°, 45° and 60° of shoulder abduction in the frontal plane. During the first measurement at 0° of abduction, the participant's upper arm was relaxed alongside the body in the frontal plane, the elbow was flexed and the hand was positioned on the thigh (ulnar side of the hand resting on the thigh, thumb pointing upwards). Concerning the measurements at 45° and 60° of shoulder abduction, a smartphone application (Plaincode Clinometer 4.3 application) was used to determine the correct angle of shoulder abduction in the frontal plane (upper arm in line with the plane of the trunk). This arm position was actively maintained and controlled by applying minimal tension against a fixation belt (without pulling at it), which was wrapped around the participant's proximal forearm.
The ultrasound probe was positioned on the anterior acromial angle (marked previously) with the long axis of the probe in the scapular plane. The acromion and humeral head were visualized and slight changes in probe position (slight dorsal shift/tilting of probe) were made until a clear image appeared. In each position 2 images were captured, resulting in a total of 12 images per participant. The actual measurement of the AHD at each image was done afterwards, when testing of all participants was completed.
Data analysisThe images made during the AHD measurement were saved for processing at a later stage, for which the EchoMaster 3.5.1 software was used. The AHD was defined as the tangential distance from the most lateral part of the acromion to the humeral head9 (Fig. 1). These measurements were independently performed twice by 2 different researchers. All images were anonymized and randomized before analysis. Analyzing the images, measuring the effective AHD, was done in a blinded fashion. The researchers did not know to which of the 2 groups the participants belonged to. Previous studies show that AHD measured with ultrasonography has a good inter-rater reliability, ranging from 0.86 to 0.9229 as well as a good test-retest reliability, ranging from 0.88 to 0.92.10 In this study, AHD was measured twice at each angle of abduction (Image 1 and 2) and afterwards, each image was also analyzed twice on different occasions. Therefore, intraclass correlation coefficients (ICC) could be calculated to indicate the reliability of the measurement. These ICCs show an excellent correlation between the first and the second AHD measurement (ICC2,1=.876). Additionally, the Minimal Detectable Change (MDC) with 95% confidence bounds was calculated as well.
Statistical analysis
Descriptive statistics were used to summarize the demographic characteristics and are represented in terms of means and standard deviations (SD). The AHD was expressed in millimeters.
Data control was performed and all dependent variables were controlled for normal distribution using the Shapiro–Wilk test and visual control of the related histograms. Parametric statistics were performed since the data were normally distributed. An independent t-test was used to analyze group differences concerning age, height, weight and body mass index (BMI).
For statistical analysis, a general linear model 2-way analysis of variance (ANOVA) with repeated-measures design was performed for each abduction angle. The within-subjects factor was side (2 levels: dominant side and non-dominant side) and the between-subjects factor was group (2 levels: hockey players and control group). Interaction effects of group x side, as well as main group and side effects, were of interest. In the presence of an interaction effect, group differences and side differences were tested post hoc at each level of the interacting variable using a Bonferroni adjustment. In the absence of interactions, main effects of group and side were analyzed. The α level was set at 0.05 for all analysis. All statistical analyses were performed with the statistical package for social sciences (Version 24.0, SPSS, Inc., Chicago, IL).
ResultsParticipant characteristicsDemographic and sports-related characteristics are displayed in Table 1. Independent t-tests showed no significant differences between groups with respect to age, weight, height and BMI. In both the elite field hockey group and the control group, all participants were right handed.
Demographic characteristics of the participants (mean±SD).
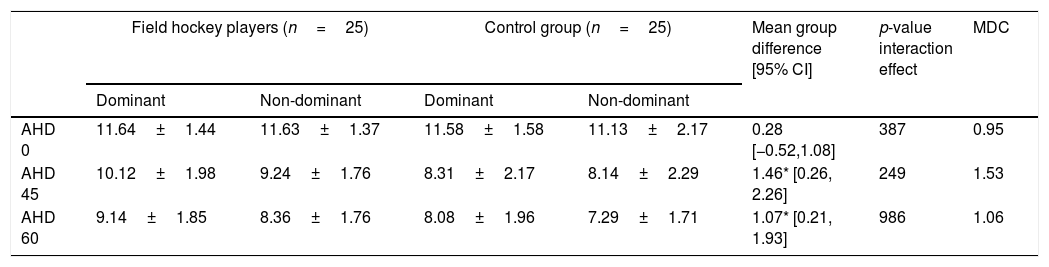
Table 2 summarizes the descriptive data for the comparison of the AHD between field hockey players and control participants. AHD is expressed in millimeters and mean value with standard deviation is presented for each side within each group. The p-values for main group, main side and group x side interaction effect are also indicated in this table, as well as the MDC values, calculated for each degree of shoulder abduction at which AHD was measured.
Results of the AHD (mm) measurement (mean±SD), group differences (mean and 95% CI), MDC values (mm) and statistical analysis.
| Field hockey players (n=25) | Control group (n=25) | Mean group difference [95% CI] | p-value interaction effect | MDC | |||
|---|---|---|---|---|---|---|---|
| Dominant | Non-dominant | Dominant | Non-dominant | ||||
| AHD 0 | 11.64±1.44 | 11.63±1.37 | 11.58±1.58 | 11.13±2.17 | 0.28 [−0.52,1.08] | 387 | 0.95 |
| AHD 45 | 10.12±1.98 | 9.24±1.76 | 8.31±2.17 | 8.14±2.29 | 1.46* [0.26, 2.26] | 249 | 1.53 |
| AHD 60 | 9.14±1.85 | 8.36±1.76 | 8.08±1.96 | 7.29±1.71 | 1.07* [0.21, 1.93] | 986 | 1.06 |
The general linear model 2-way ANOVA with repeated-measures design revealed no significant interaction effects for none of the AHD measurements. However, significant main group and side effects were established in 2 of the 3 studied shoulder positions, namely in 45° and 60° of shoulder abduction. Concerning the AHD measurement at 0° of abduction, no significant differences were noted.
Statistical analysis revealed a significant main group effect for both the AHD measurement at 45° and 60° of shoulder abduction. In both cases, the AHD of the field hockey players was significantly larger compared to the AHD of the control participants, for the dominant side (mean group difference at 45° and 60°, respectively: 1.81mm and 1.06mm) and the non-dominant side (mean group difference at 45° and 60°, respectively: 1.10mm and 1.07mm).
For the AHD at 60°, a significant main side effect was established. The dominant shoulder showed a significant larger AHD in comparison to the non-dominant shoulder, in both groups (mean side difference hockey players: 0.78mm; mean side difference control participants: 0.79mm).
DiscussionThe purpose of this study was to investigate the AHD in elite field hockey shoulders and to determine whether sport-specific adaptations concerning this variable occur. To this end, the complete national male field hockey team was tested bilaterally and compared to an age- and gender matched control group of non-athletic healthy participants. In total, 50 participants (25 athletes and 25 controls) were included. This is the first study addressing AHD in field hockey players.
A first finding was a significant difference between both groups for AHD at 45° and 60° of shoulder abduction in the frontal plane. At both these degrees of abduction, the AHD was larger in field hockey players compared to their matched controls, in the dominant as well as in the non-dominant shoulder. At 0° of abduction, no group difference was found. A second finding implies a side difference established in both groups: at 60° of shoulder abduction, a significant larger AHD was noted in the dominant shoulder compared to the non-dominant shoulder. At 0° and 45° of abduction, no significant differences between sides were found in either group.
A significant AHD group difference was established at 45° and 60° abduction, while no significant difference was found at 0°. This may be explained through the difference in muscle activity in both situations. The AHD measurements at 45° and 60° required active shoulder abduction of the participant, whereas the measurement at 0° of abduction was a passive measurement, with the participant's upper arm hanging alongside the body and the hand resting on the thigh.
It is well established that, when actively moving the shoulder, both glenohumeral and scapular muscle balances are of upmost importance to retain normal shoulder function. A good balance between the trapezius muscles and serratus anterior is necessary to assure optimal scapular orientation, thus optimizing the glenoid cavity positioning. Good co-activation of, as well as proper muscle balance within, the deltoid and rotator cuff couple are necessary to maintain a sufficient AHD, thereby avoiding compression in the subacromial space. The rotator cuff is responsible for maintaining normal humeral head position in the glenoid during shoulder elevation movements. The compressive forces of the cuff stabilize the humerus against the glenoid, thereby providing dynamic stabilization of the glenohumeral joint and counteracting the upwardly directed force of the deltoid.30 When these dynamic stabilizing forces are insufficient, an increase in superior and anterior migration of the humeral head occurs, narrowing the subacromial space, which may lead to impingement or could make the shoulder more susceptible to pathology.31,32 Changed scapular biomechanics (e.g. diminished upward rotation and reduction of posterior tilt) are associated with mechanical impingement.33 A more efficient working of, and cooperation between, rotator cuff and scapular muscles, results in better biomechanics and larger AHD and prevents tendon overload in the subacromial space. From a biomechanical point of view, stronger rotator cuff and scapular muscles could be associated with a larger AHD. Leong et al.14 confirmed this relationship between the subacromial space and scapular muscle strength by showing the correlation between decreased strength of the middle and lower trapezius and a reduction in subacromial space.14 As confirmed in a recent study, elite field hockey players have stronger rotator cuff muscles than non-athletes.34 This could explain the larger AHD in field hockey players at 45° and 60° of (active) shoulder abduction, with no group difference for the AHD at 0° (measured in a resting shoulder position). Since an insufficient AHD can be associated with shoulder pathology (e.g. subacromial pain syndrome, rotator cuff tendinopathy),11,13–16 an increased AHD with active shoulder movements may contribute to a better resistance against shoulder injuries. The larger AHD in field hockey players compared to controls may be a sport specific adaptation. This adaptation may also, contribute to the protection of these athletes against rotator cuff related injury. However, this type of shoulder injury does not seem to be common among these athletes.
The established group differences are quite small, ranging from 1.07mm to 1.81mm. Nevertheless, they are larger than the calculated minimal detectable change (MDC) for AHD, with exception of the group difference concerning AHD measured at 45° of abduction in the non-dominant arm. Three out of 4 group differences are thus larger than the MDC.
The finding of a larger AHD in elite field hockey players compared to controls is contrary to the findings of Silva et al.,23 who demonstrated a significant smaller AHD in junior elite tennis players, compared to control participants. Hibberd et al. compared the AHD of competitive adolescent swimmers with a control group of non-overhead athletes and found a bilaterally larger AHD in the swimmers group. These findings are in line with the results of this study, implying a sport-specific adaptation in these athletes, resulting in a larger AHD.23
One significant side difference was found in both groups at 60° of shoulder abduction, with a larger AHD at the dominant side compared to the non-dominant side. This difference between both shoulders was almost exactly the same for both groups: 0.78mm in the athlete group, 0.79mm in the control group. These side differences are smaller than the MDC and therefore of less clinical relevance. At 0° and 45°, no significant AHD side differences were found. Previous studies have stated different, compatible as well as incompatible, conclusions concerning whether or not side differences are present for AHD. In some studies involving shoulder-loading athletes a side difference is noted. However, direction of this difference differs across studies with some revealing a larger AHD on the dominant side, while others note a smaller AHD on this side compared to the non-dominant one.9,20,21 In the study of Thomas et al.22 in college baseball players, AHD was measured at 0° and 90° of abduction and in this study no side difference was found.22 No side differences were also concluded by Petersson et al.,12 who studied the AHD in a general, non-athletic population.12 Putting together these results with the result of this study, no uniform conclusion can be made concerning the presence of side differences in AHD.
Limitations and strengthsThe relatively limited study sample could be considered a limitation of this study. The sample size would preferably be larger but testing of the national team in isolation preserves the inclusion of elite players only. Expanding the sample size to include sub-elite players diminishes one of the strengths of this study, namely the investigating the shoulder of one of the best field hockey teams in the world.
An obvious strength of this study is the fact that this is the first study addressing AHD in field hockey players. In this aspect, this study can contribute to a better understanding of the shoulder of these not yet widely studied athletes. Secure and consistent reporting was of upmost importance in describing the measurement procedure, since key components of the protocol must be clearly stated to support consistent standardization of the measurement method (e.g. probe positioning, AHD definition). Additionally, excellent ICC values assure a good test–retest reliability of the measurements. Reliability of the AHD measurement through ultrasound has been previously investigated and found to be good to excellent.6
A limitation of the study concerns the current debate regarding the clinical relevance of AHD measurements. Inconsistent AHD changes in rotator cuff tendinopathy patients compared with pain-free shoulders have for example been reported in a recent review by McCreesh et al.6 However, the latest studies by Navarro et al. did show an association between AHD and shoulder pain and function in chronic shoulder pain patients.7,8
The clinical implications of this study may be found in the results themselves. With active shoulder abduction, the AHD in the shoulders of elite field hockey players was found to be larger compared to non-athletic participants. This may be a protective sport-specific adaptation, to better guard the highly loaded joint from injury. In light of injury prevention, AHD measurement may help physical therapists and coaches decide which athletes could benefit from specific, additional exercises aimed at enlarging the subacromial space. Adding appropriate exercises to the training program of athletes with smaller AHD values compared to their colleagues could contribute to the tenability of the shoulder. Since optimal functioning athletes are a necessity in any team sport, injury prevention should be a distinct priority. Prospective research should however further clarify the relationship between AHD and shoulder injury risk.
SuggestionsExpanding the study sample would be an appropriate step in further research. Recruiting more elite field hockey players add to the current study sample would be interesting, as well as repeating the same study with a sample of sub-elite and/or recreational field hockey players to investigate if the same observations can be made in lower level field hockey players. Second, instead of the cross-sectional design operated in this study, a prospective study design would be suitable to examine whether AHD could be predictive for shoulder complaints in these athletes. The set-up of a prospective study would therefore be greatly encouraged to contribute to the understanding of the influence of this variable. Specific research focusing on pinpointing the explanation for this difference in AHD between field hockey players and non-athletes would also favorably add to this understanding. Lastly, uniformity in AHD measurement protocols should be pursued, with clear and unambiguous reporting of the measurement procedure.
ConclusionsIn both shoulders, elite field hockey players have a statistically significant and clinically relevant larger AHD than their matched controls, when actively abducting their shoulder to 45° and 60° in the frontal plane. This may be a protective sport-specific adaptation to shield these athletes from certain shoulder problems and may be linked to superior shoulder girdle strength in the field hockey players. At 60° of abduction, a statistically significant larger AHD in the dominant side compared to the non-dominant side was noted in both groups. However, this difference was not clinically relevant. Further research should focus on expanding the study sample and investigating AHD in a prospective manner.
Conflicts of interestThe authors declare no conflicts of interest.
The authors thank Annelien Claeys, Axelle Delobelle, Siemen Tas, Aran Tulkens and Martijn van den Biggelaar for their help in the acquisition of the data. The authors’ gratitude also goes out to all the members of the male national field hockey team, the Red Lions, as well as to the volunteers of the control group, for their participation in this study.



