




Overuse injuries result from the cumulative process of repetitive microtrauma and overload on the musculoskeletal system, which causes tissue damage. Therefore, these injuries may have long-term negative consequences that decrease an athlete's performance.
ObjectiveTo estimate the prevalence of overuse injuries in individual and team sports.
MethodsSearches on MEDLINE, EMBASE, SPORTDiscus, and CINAHL from the first registration to February 2021 and hand-searching identified studies investigating the prevalence of overuse injuries in athletes from individual and team sports. Meta-analysis was conducted and the GRADE system summarized the overall quality of evidence. This review was registered in PROSPERO (CRD42019135665).
ResultsSeventeen studies were included and pooling of 24 704 participants (22 748 of individual sports and 1.956 of team sports). Data from point- and period-prevalence of overuse injuries in individual and team sports were obtained. Pooled period-prevalence of overuse injuries in individual and team sports was 42.0% (95% CI: 30.0, 55.0) and 33.0% (95% CI: 21.0, 49.0), respectively. Another four studies investigated point-prevalence. The overall quality of evidence for the period-prevalence was of moderate quality. Sensitivity analyses suggested that different joints based in individual and team sports tended to increase the estimated prevalence of overuse injuries.
ConclusionAthletes, clinicians, sport teams, and policymakers should be aware of the high prevalence of overuse injuries in athletes, especially, in athletes from individual sports. Current moderate-quality evidence shows that future high-quality studies are likely to impact on the estimated prevalence.
Sports injuries may have different definitions.1–3 However, a commonly accepted definition is “any physical complaint sustained by a player that result from a match or training, irrespective of the need for medical attention or time loss from activities”.2,3 Overuse injury is an injury without a specific and identifiable event associated with its onset.2 It results from the cumulative process of tissue damage rather than instantaneous energy transfer,4,5 which causes a repetitive microtrauma and overload in the musculoskeletal system that would not result in injury if the affected tissue had sufficient time to recover.6,7 Thus, overuse injuries can cause long-term negative consequences that decrease an athlete's performance,8,9 causing pain and dysfunction, and in some cases, could end an athlete's career. Considering that athletes often do not have proper time to recover between training sessions and competitions, overuse injuries might be highly prevalent in sports.
Prevalence of overuse injuries might be different in individual and team sports. For example, Lemoyne et al.10 showed higher prevalence of overuse injuries in individual sports (24%) in comparison to team sports (8%). This may be explained by the fact that, in individual sports, all demand is concentrated in an individual athlete, while in team sports demand is shared between different athletes.10,11 In addition, the prevalence of overuse injuries is probably related to the sports demand. Aasheim et al.12 reported prevalence of 39% of overuse injuries in handball players, with the shoulder (17%), knee (14%), and lumbar spine(12%) as the most frequently affected regions. In sports where the shoulder is exposed to repeated overhead motion at high speeds, like handball, overuse injuries are commonly reported.13,14 Prevalence data of overuse injuries in individual and team sports may help clinicians decide the level of effort required for surveillance methods and also on preventive and rehabilitation strategies for this type of injury. In addition, it can also promote the development of future studies about the efficacy of different strategies to prevent and/or reduce the severity levels of this type of injury.
Previous systematic reviews15,16 that investigated the prevalence of overuse injuries in different sports did not perform meta-analysis of the data to estimate the prevalence of overuse injuries in the investigated sports. The strength of the evidence was not investigated as well. Therefore, the purpose of this systematic review with meta-analysis was to investigate the prevalence of overuse injuries in individual and team sports. We also assessed the quality of the evidence and the strength of the recommendation.
MethodsThe review protocol was prospectively registered at PROSPERO (CRD42019135665) and the methods followed recommendations from the Joanna Briggs Institute Reviewers Manual (Systematic Review of Prevalence and Incidence Data),17 the Cochrane Collaboration,18 and PRISMA reporting guidelines.19
Inclusion criteriaInclusion criteria of the studies included in this review were as follows: (1) studies should state a clear and similar definition of overuse injuries (e.g. injuries without a specific identifiable event, or gradual onset, or resulting from repetitive microtrauma); (2) studies should specifically report the prevalence of overuse injuries, and; (3) the population included should be athletes of any sport, regardless of professional or amateur level and age group.
SearchElectronic database searches were performed from the earliest record to February 2021 using MEDLINE and EMBASE (via OvidSP), SPORTDiscus, and CINAHL (via EBSCO), without language or date restriction. Additional hand searching was conducted by reviewing articles published in relevant sports journals and the reference list of all eligible studies. The terms used in the search strategy were related to 'prevalence', 'overuse injury', 'athletes', 'sports'. The complete search strategy is presented in the Supplemental online material.
Study selection and appraisalFor studies selection, after removing duplicates, two independent reviewers (MFF and TMN) screened all titles and abstracts identified by the search strategy for eligibility. Then, full texts for all potential eligible studies were retrieved. The same two reviewers independently evaluated all full texts, and studies fulfilling the inclusion criteria were included. Any disagreements were resolved by a third reviewer (FOM).
Data extractionFor data extraction, two reviewers (MFF and TMN) independently extracted the characteristics of all included studies (e.g. study design, setting, study population, overuse injuries definition, how overuse injuries were measured and their point- or period-prevalence), with a third reviewer (FOM) resolving any discrepancies. Point-prevalence is defined as the number of people with a current overuse injuries at a specific point in time and period-prevalence is defined as the number of people with overuse injuries over a specified period of time.20 For prevalence data, we extracted the total proportion of overuse injury and, when available, the proportion of overuse injury for individual and team sports and for each anatomical area. Moreover, when available, we reported prevalence of substantial overuse injuries, which is defined as injuries leading to moderate or severe reduction in training volume or performance, or complete inability to participate in sports.
Assessment of risk of biasTwo independent reviewers (MFF and TMN) assessed risk of bias for each included study, using The Joanna Briggs Institute Prevalence Critical Appraisal Tool.21 This tool consists of 9 items specifically designed to assess the methodological quality of prevalence studies. Each item is rated as ‘yes’, ‘no’, or ‘unclear’ according to information available in each study, with a maximum score of 9 points, one point for each “yes” answer. The higher the score, the better the methodological quality. A third reviewer (FOM) solved potential disagreements. To assess if sample size of each included study was appropriate (e.g. item 3), we used the equation provided in a previous study,22 where p was the expected prevalence (29.3%), which was defined based on the results of a previous study,23 Z was the confidence level (1.96), and d was the precision (5.0%). Sample size estimation resulted in an appropriate sample size of 318 participants. A fourth reviewer (RAR) solved potential disagreements regarding risk of bias assessment.
Data analysis and data quality assessmentThe I² statistics was used to assess among-study heterogeneity and pooling estimated prevalence of overuse injuries in athletes of different sports, separated in individual and team sports, following the Cochrane recommendations.18 For pooling, random-effects model was used when I² ≥ 50.0%. Findings from pooling and individual studies were presented in forest plots with 95% confidence interval (CI). We planned to analyze separately the point- and period-prevalence.
Sensitivity analysis was performed to compare whether prevalence of overuse injuries in specific body regions (i.e. shoulder, lower back, knee, and hip/groin/thigh) differ between individual and team sports. All analyses were performed using Comprehensive Meta-Analysis, version 2.2.04 (Biostat, Inc.©, Englewood, New Jersey).
The GRADE (Grading of Recommendations Assessment, Development and Evaluation) system was used to summarize the overall quality of the evidence. This tool provides four levels ranging from high-quality evidence to very low-quality evidence.24 Scoring of evidence started at high-quality evidence, which was downgraded one level for each of the following pre-specified criteria: (1) poor methodological quality (average risk of bias ≤ 5 points out of 9); (2) imprecision (when ≥ 50% of studies did not present appropriate sample size – minimum of 318 participants); (3) indirectness (when more than 25% of studies used non-standard measurements of overuse injuries); and (4) inconsistency (if I² ≥ 50.0%).25,26 Single studies (n < 318 participants) were considered inconsistent and imprecise (that is, sparse data) and provided low quality evidence. This could be further downgraded to very low quality evidence if studies were assessed as having high risk of bias. Due to the small number of studies (n=3) reporting point-prevalence of overuse injuries in individual and team sports, our meta-analysis and sensitivity analysis focused on period-prevalence. Two independent reviewers (MFF and TMN) assessed the quality of evidence using GRADE and between-reviewer discrepancies were resolved by a third reviewer (FOM).
ResultsStudy selectionSearches retrieved 4807 titles and, after excluding duplicates, we identified 2069 references that had the title analyzed. Following the title, abstracts, and full-texts screening, 17 studies were included in this review. Included studies were published between the years of 2007 and 2021. The main reasons for excluding potential full texts (n = 63) were non-athlete participants (n = 4), no reporting of prevalence estimates (n = 53), and no adequate definition of overuse injuries (n= 6) (Fig. 1). Table 1

Characteristics of the included studies (n = 17).
| Study, Year | Design | Setting | Study Population | Overuse Injuries definition | Overuse Injuries measurement | Prevalence of overuse injuries |
|---|---|---|---|---|---|---|
| Aasheim et al.,12 2018 | Prospective cohort study | Location: NorwaySample selection: Expedience | n* = 145Range age: 16.0-18.0 yearsSex: MaleSport: HandballPractice duration: 14 hours per week | Type of injuries that are caused by cumulative tissue overload without any clear onset | The Oslo Sports Trauma Research Center (OSTRC) Overuse Injury Questionnaire | 34-week period prevalence of overuse injuries: 39.0%Shoulder (25)*: 17.0%,Knee (20)* : 14.0%,Lower back (17)*: 12.0%,Elbow (13)*: 9.0%Substantial overuse problems** (22)*: 15.0%Shoulder (10)*: 7.0%,Knee (7)*: 5.0%,Lower back (4)*: 3.0%,Elbow (1)*: 1.0% |
| Andersen et al.27 2013 | Prospective cohort study | Location: NorwaySample selection: Expedience | n* = 174Average age: 38.0 ± 9 yearsSex: Male and femaleSport: TriathlonPractice duration: 276 hours in training during the 26 weeks | Injuries that could not be linked to a specific event | The OSTRC Overuse Injury Questionnaire | 26-week period prevalence of overuse injuries: 56.0%Knee (43)*: 25.0%,Lower leg (40)*: 23.0%,Lower back (40)*: 23.0%,Shoulder (35)*: 20.0%,Thigh (21)*: 12.0%Substantial overuse problems** (35): 20.0%Knee (12%)*: 7.0%,Lower leg (12)*: 7.0%,Shoulder (7)*: 4.0%,Lower back (7)*: 4.0%,Thigh (5)*: 3.0% |
| Clarsen et al.,28 2015 | Prospective cohort study | Location: NorwaySample selection: Expedience | n* = 313 (cross-country skiing = 45; road cycling = 98; floorball = 50; handball = 55; volleyball = 65)Range age: 14.0-32.0 years for boys and 14.0-33.0 years for girlsPractice duration: On average 4 to 25 years (boys) and 3 to 18 years (girls) | The result of a cumulative process of tissue damage rather than instantaneous energy transfer | The OSTRC Overuse Injury Questionnaire | 13-week period prevalence of overuse injuries: N/ACross-country skiing*: N/AKnee (25)*: 8.0%,Lower back (16)*: 5.0%,Anterior thigh (37)*: 12.0%,Shoulder (3)*: 1.0%Road cycling*: N/AKnee (72)*: 23.0%,Lower back (50)*: 16.0%,Anterior thigh (25)*: 8.0%,Shoulder (22)*: 7.0%Floorball*: N/ALower back (91)*: 29.0%,Knee (84)*: 27.0%,Shoulder (47)*: 15.0%Handball*: N/AShoulder (69)*: 22.0%,Knee (63)*: 20.0%,Lower back (37)*: 12.0%Volleyball*: N/AKnee (112)*: 36.0%,Shoulder (50)*: 16.0%,Lower back (44)*: 14.0%Substantial overuse problems**: N/ACross-country skiing*: N/AAnterior thigh (22)*: 7.0%,Knee (3)*: 1.0%,Lower back (3)*: 1.0%,Shoulder (3)*: 1.0%Road cycling*: N/AKnee (25)*: 8.0%,Lower back (19)*: 6.0%,Anterior thigh (12)*: 4.0%,Shoulder (3)*: 1.0%Floorball*: N/AKnee (12)*: 4.0%,Lower back (9)*: 3.0%,Shoulder (3)*: 1.0%Handball*: N/AKnee (25)*: 8.0%,Shoulder (19)*: 6.0%,Lower back (6)*: 2.0%Volleyball*: N/AKnee (47)*: 15.0%,Shoulder (16)*: 5.0%,Lower back (3)*: 1.0% |
| Delfino Barboza et al.,29 2018 | Prospective cohort study | Location: NetherlandsSample selection: Expedience | n* = 80Average age: 23.2 yearsSex: Male and femaleSport: Field hockeyPractice duration: 8.8 hours | Overuse injury was considered if onset could not be linked to a clearly identifiable event | Dutch version of the Oslo Sports Trauma Research Centre questionnaire on health problems (OSTRC-H) | 2-week point prevalence of overuse injuries: 55.0%Thigh (10)*: 13.0%,Knee (8)*: 10.0%,Lower leg (6)*: 8.0%,Lower back (6)*: 7.0%,Hip/groin/pelvis (5)*: 6.0%,Foot/toe (4)*: 5.0%,Shoulder/upper arm (4)*: 5.0%,Ankle (2)*: 3.0%,Upper back/thorax/chest (2)*: 2.0%,Finger/wrist/hand (1)*:1.0%,Head/face/neck (1)*: 1.0% |
| Docking et al.,36 2018Du Toit et al.,34 2020Fröhlich et al.,40 2020Gram et al.,41 2020 | Prospective cohort studyCross-sectional studyProspective cohort studyProspective cohort study | Location: AustraliaSample selection: ExpedienceLocation: South AfricaSample selection: ExpedienceLocation: Switzerland Sample selection: ExpedienceLocation:NorwaySample selection: Expedience | n* = 441Average age: 24.8 yearsSex: MaleSport: FootballPractice duration: N/An* = 21824Average age: N/ASex: Male and femaleSport: Road cyclistsPractice duration: N/An* = 26Average age: 20.91 ± 2.67 yearsSex: FemaleSport: Alpine SkiingPractice Duration: 19.4±5.0 hours per weekn*= 107Average age: 14.5 ± 1.6 yearsSex: FemaleSport: Rhythmic gymnasticsPractice Duration: 4.3 ± 1.5 years | Gradual development of signs and symptomsGradual onset injuriesAny physical complaint caused by repeated microtrauma without a link to a single, clearly identifiable eventInjury caused by multiple accumulative bouts of energy transfer without a single, clearly identifiable event | The OSTRC Overuse Injury QuestionnaireOnline medical questionnaireThe OSTRC Overuse Injury QuestionnaireThe Oslo SportsTrauma Research Center Questionnaire on HealthProblems (OSTRC-H2) | 9-month period prevalence of overuse injuries: 39.4%Knee (111)*: 25.2%,Ankle (95)*: 21.5%Substantial overuse problems** (62)*: 14.2%Knee (35)*: 7.9%,Ankle (28)*: 6.3%Point-prevalence of overuse injuries: 1.1%Neck (938)*: 4.3%Shoulder (2837)*: 13.0%Wrist (545)*: 2.5%Elbow (502)*: 2.3%Finger (371)*: 1.7%Lower Back (2509)*: 11.5%Hip (1091)*: 5.0%Groin (371)*: 1.7%Knee (5739)*: 26.3%Foot (611)*: 2.8%Ankle (567)*: 2.6%Point-prevalence of overuse injuries: N/AKnee (52)*: 28.7%,Lower back (37)*: 20.5%,Hip/groin (19)*: 10.5%Substantial overuse problems**(x):Knee (52)*: 4.4%,Lower back (37)*: 0.0%,Hip/groin (19)*: 2.7%15-week period prevalence of overuse injuries: 37%Ankle (7)*: 1.87%Ribs/upper back (4)*: 1.07%Foot (14)*: 3.75%Hip/groin (23)*: 6.16%Knee (33)*: 8.84%Lower back (27)*: 7.23%Lower leg (11)*: 2.94%Neck (2)*: 0.53%Pelvis (7)*: 1.87%Shoulder (5)*: 1.34%Thigh (4)*: 1.07%Wrist (1)*: 0.26% |
| Lemoyne et al.,10 2017 | Cross-sectional study | Location: CanadaSample selection: Expedience | n* = 81(team sports = 61; individual sports = 20)Average age: 24.0 ±1.9 yearsSex: Male and femaleSport: Cross-country running, cheerleading, ice hockey, soccer, swimming and volleyballPractice duration: 12.3 ± 5.4 hours per week | Gradual-onset injuries caused by repeated trauma | Online questionnaire | 3-Month period prevalence of overuse injuries: 13.0%Individual sports (20)*: 24.0%,Team sports (6)*: 8.0% |
| Leppänen, et al.,30 2018 | Prospective cohort study | Location: FinlandSample selection: Expedience | n* = 733Average age: 11.7 ± 1.1 years for boys and 11.8 ± 1.1 years for girlsSex: Male and femaleSport: FootballPractice duration: 6.3 ± 1.7 years for boys and 5.1 ± 1.7 years for girls | Injuries that do not have a specific identifiable event | The OSTRC Overuse Injury Questionnaire | 20-week period prevalence of overuse injuries: 12.8%Knee (42)*: 5.7%,Heel (19)*: 2.6%,Hip/groin (8)*: 1.1%,Lower back (6)*: 0.8%Substantial overuse problems** (44): 6.0%Knee (17)*: 2.4%,Heel (8)*: 1.1%,Hip/groin (4)*: 0.5%,Lower back (4)*: 0.5% |
| Magno et al.,31 2013 | Descriptive, observational, analytic epidemiologicalstudy | Location: BrazilSample selection: Expedience | n* = 40Average age: N/ASex: Male and femaleSport: Paralympic Track and FieldPractice duration: N/A | Repeated microtrauma without a single, identifiable event responsible for the injury | A standardized injury report form | Point-prevalence of overuse injuries: 82.0% |
| Nagano et al.,39 2019Nordstrom et al.,37 2020 | Prospective studyProspective cohort study | Location: JapanSample selection: ExpedienceLocation: NorwaySample selection:Expedience | n* = 29Average age: N/ASex: FemaleSport: SwimmingPractice duration: 7.7 ± 1.2 yearsn* = 225Range age: 17.0-41.0 yearsSex: MaleSport: Ice hockeyPractice duration: N/A | Injuries which are not associated with a specific, clearly identifiable injury event, regardless of whether their onset was gradual or rapidOveruse injury is a specific unidentifiable event responsible for its occurrence | Japan version of the OSTRC Overuse Injury QuestionnaireOslo Sports Trauma Research Center Questionnaire on Health Problems (OSTRC-H) | 24-week period prevalence of overuse injuries: 49.1%Lower back (8)*: 27.6%,Shoulder (5)*: 16.0%,Knee (3)*: 9.9%,Ankle (3)*: 9.0%,Hip/thigh (2)*: 5.2%,Pelvis/glute (1)*: 3.1%,Foot (1)*: 2.8%,Elbow/upper arm (0)*: 2.2%,Wrist/forearm (0.4)*: 1.3%,Finger (0)*: 0.3%Substantial overuse problems** (3)**: 10.9%Lower back (1)*: 4.3%,Knee (0)*: 2.8%,Ankle (0)*: 1.2%,Shoulder (0)*: 0.6%Hip/thigh (0)*: 0.4%,Pelvis/glute (0)*: 0.2%,Elbow/upper arm (0)*: 0.2%,31-week period prevalence of overuse injuries: 15.0%Substantial overuse injuries** (13)*: 6.0% |
| Rejeb et al.,38 2017Schoeb et al.,35 2020 | Prospective studyProspective cohort study | Location: Middle EasternSample selection: ExpedienceLocation: Switzerland Sample selection: Expedience | n* = 166Average age: 12.0 ± 18.0 yearsSex: MaleSport: Track and field, squash, table tennis, fencing, gymnastics, swimming, golf and shootingPractice duration: 16 hours per week and 120 minutes per sessionn* = 155Average age: 13.89 ± 0.60 yearsSex: Male and FemaleSport: Alpine SkiingPractice duration: N/A | Injuries resulting from insidious onset without a recognizable mechanismNo such inciting event was identifiable. | Data from medical records were used to documentall sports-related injuriesOslo Sports Trauma Research Center Questionnaire on Health Problems (OSTRC-H) | 6-Year period prevalence of overuse injuries: 50.3%12-month period prevalence of overuse injuries: 13.6%Head/face (1)*: 0.07%Neck/cervical spine (5)*: 0.39%Shoulder/clavicle (1)*: 0.07%Elbow (2)*: 0.15%Wrist (1)*: 0.07%Hand/finger (2)*: 0.15%Abdomen (1)*: 0.07%Thoracic spine (5)*: 0.39%Lumbar spine (36)*: 2.81%Pelvis/sacrum (4)*: 0.31%Hip/groin (16)*: 1.25%Thigh (7)*: 0.54%Knee (59)*: 4.61%Tibia (12)*: 0.93%Ankle (5)*: 0.39%Foot/toe (16)*: 1.25%Other (1)*: 0.07%Substantial overuse problems**(77)*: 5%Neck/cervical spine (1)*: 0.06%Shoulder/clavicle (1)*: 0.06%Elbow (1)*: 0.06%Wrist (1)*: 0.06%Hand/finger (1)*: 0.06%Abdomen (1)*: 0.06% Thoracic spine (4)*: 0.25%Lumbar spine (15)*: 0.97%Pelvis/sacrum (2)*: 0.12%Hip/groin (6)*: 0.38%Thigh (3)*: 0.19%Knee (22)*: 1.4%Tibia (6)*: 0.38%Ankle (3)*: 0.19%Foot/toe (10)*: 0.64% |
| Von Rosen et al.,32 2016 | Prospective cohort study | Location: SwedenSample selection: Expedience | n* = 64Average age: 17.0 ± 1.0 yearsSex: Male and FemaleSport: RunningPractice duration: 6.8 hours per week | Injuries not caused by a specific identifiable event | The OSTRC Overuse Injury Questionnaire | 26-week period prevalence of overuse injuries: 76.6%Foot/lower leg (14)*: 22.2%,Knee (6)*: 10.0%,Hip (3)*: 5.4%,Lower back (1)*: 1.6,Other anatomical areas (0)*: 0.5%Substantial overuse problems** (35): 54.7%Foot/lower leg (7)*: 10.8%,Knee (3)*: 4.4%,Hip (2)*: 3.3%,Lower back (0)*: 0.2% |
| Worner et al.,33 2019 | Descriptive epidemiology study. | Location: SwedenSample selection: Expedience | n* = 101Average age: 22.0 ± 4.9 years for boys and 21.0 ± 3.9 years for girlsSex: Male and femaleSport: Ice hockey (goalkeepers)Practice duration: N/A | Gradual onset injuries | The OSTRC Overuse Injury Questionnaire | 34-week period prevalence of overuse injuries: 28.1%Substantial overuse problems**(10)*: 10.0% |
n, sample size; SD, standard deviation; N/A, not applicable
Most of the included studies (n = 10) included data from both sex,10,27–35 four included only male athletes,12,36–38 three included only females participants.39–41 Regarding the study design, thirteen were prospective cohort studies,12,27–30,32,35–41 two studies were descriptive epidemiological studies,31,33 and two were cross-sectional studies.10,34 For overuse injuries measurement, nine studies used the Oslo Sports Trauma Research Center questionnaire (OSTRC),12,27,28,30,32,33,36,39,40 four used the Oslo Sports Trauma Research Center questionnaire on health problems (OSTRC-H),29,35,37,41 one used an injury record form,31 two used a questionnaire on injuries originally developed by the authors,10,34 one used medical record data.38 Thirteen studies reported period prevalence,10,12,27,28,30,32,33,35–39,41 among them, three studies reported pre-competition prevalence,27,40,41 two studies reported pre- and during the season prevalence,35,36 four studies reported prevalence during the season,12,32,33,37 and five studies did not specify when the prevalence measure was taken.10,28,30,38,39 In addition, four studies reported point-prevalence.29,31,34,40 Twelve studies reported prevalence of overuse injuries separated by anatomical areas,12,27,28,30,32,33,35–37,39–41 one study reported separated team and individual sports,10 and twelve studies reported the prevalence of substantial overuse injuries.12,27–30,32,34–36,39–41
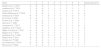
Methodological qualityMean ± standard deviation methodological quality of the included studies was 5.8 ± 1.3 of 9 (ranging from 0 to 9). Seven studies scored ≤5 of 9.10,31,32,34,36–38 Methodological quality items for each included study are reported in Table 2. Of seventeen studies, nine did not use sample frame appropriate to address the target population,12,31,32,34–36,38,40,41 seventeen did not sample study participants in an appropriate way,10,12,27–41 fourteen did not have appropriate sample size,10,12,27–29,31–33,35,37–41 five did not describe subjects and the setting in detail, 32,34-37 one did not analyze data with sufficient coverage of the identified sample,31 four did not use valid methods for the identification of overuse injuries,10,31,34,38 no study present measures in a standard and reliable way for all participants, three did not have appropriate statistical analysis,34,36,37 and three did not reach appropriate response rate.10,29,31
Methodological quality of the included studies (n =17).
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Overall score (0-9) |
|---|---|---|---|---|---|---|---|---|---|---|
| Aasheim et al.,12 2018 | N | N | N | Y | Y | Y | Y | Y | Y | 6 |
| Andersen et al.,27 2013 | Y | N | N | Y | Y | Y | Y | Y | Y | 7 |
| Clarsen et al.,28 2015 | Y | N | N | Y | Y | Y | Y | Y | Y | 7 |
| Delfino Barboza et al.,29 2018 | Y | N | N | Y | Y | Y | Y | Y | N | 6 |
| Docking et al.,36 2018 | N | N | Y | N | Y | Y | Y | U | Y | 5 |
| du Toit et al.,34 2020 | N | N | Y | U | Y | N | Y | U | Y | 4 |
| Fröhlich et al.,40 2020 | Y | N | N | Y | Y | Y | Y | Y | Y | 7 |
| Gram et al.,41 2020 | Y | N | N | Y | Y | Y | Y | Y | Y | 7 |
| Lemoyne et al.,10 2017 | Y | N | N | Y | Y | N | Y | Y | N | 5 |
| Leppänen, et al.,30 2019 | Y | N | Y | Y | Y | Y | Y | Y | Y | 8 |
| Magno e Silva et al.,31 2013 | N | N | N | Y | U | U | Y | Y | U | 3 |
| Nagano et al.,39 2019 | Y | N | N | Y | Y | Y | Y | Y | Y | 7 |
| Nordstrom et al.,37 2020 | Y | N | N | N | Y | Y | Y | U | Y | 5 |
| Rejeb A et al.,38 2017 | N | N | N | Y | Y | N | Y | Y | Y | 5 |
| Schoeb et al.,35 2020 | Y | N | N | U | Y | Y | Y | Y | Y | 6 |
| Von Rosen et al.,32 2016 | N | N | N | U | Y | Y | Y | Y | Y | 5 |
| Worner et.al.,33 2020 | Y | N | N | Y | Y | Y | Y | Y | Y | 7 |
1. Was the sample frame appropriate to address the target population?
2. Were study participants sampled in an appropriate way?
3. Was the sample size adequate?
4. Were the study participants and the setting described in detail?
5. Was the data analysis conducted with sufficient coverage of the identified sample?
6. Were valid methods used for the identification of the condition?
7. Was the condition measured in a standard, reliable way for all participants?
8. Was there appropriate statistical analysis?
9. Was the response rate adequate, and if not, was the low response rate managed appropriately?
Y, yes; N, no; U, unclear; N/A, not applicable.
Pooling of 24 704 participants, 22 748 from individual sports and 1956 from team sports, from the 17 included studies was done to estimate the prevalence of overuse injury in individual and team sports separately (Fig. 2). According to the GRADE system, pooling of thirteen period-prevalence studies provided low-quality evidence that the prevalence of overuse injuries in individual sports was 42.0% (95% CI: 30.0, 55.0) and team sports was 33.0% (95% CI: 21.0, 49.0). The evidence was downgrade from high- to low-quality because of imprecision and inconsistency. Due to the small number of studies (n=3) reporting point-prevalence of overuse injuries in individual and team sports, we were not able to conduct a meta-analysis to estimate the point-prevalence.
Sensitivity analysis
Sensitivity analysis showed that the period-prevalence estimates for individual and team sports did not significantly differ across body regions. The lack of statistically significant difference is evidenced by the overlap of 95% CIs between the period-prevalence estimates between individual and team sports. Further details can be seen in Fig. 3.
Discussion
This systematic review with meta-analysis investigated the prevalence of overuse injuries in athletes in individual and team sports, separately. The prevalence of overuse injuries was 42.0% (95% CI: 30.0, 55.0) in individual sports and 33.0% (95% CI: 21.0, 49.0) in team sports. These results demonstrate that overuse injuries are highly prevalent in athletes and suggest that athletes from individual sports have higher prevalence of overuse injuries than athletes from team sports. According to the GRADE system, we found low-quality of evidence in period-prevalence which suggests that estimated prevalence of overuse injuries in athletes will probably change with future high-quality studies.
Findings from previous studies suggested that athletes from individual sports are exposed to more risk factors for the development of overuse injuries than athletes from team sports.11,42,43 For example, athletes from individual sports may have reduced sleep time and quality,43 earlier specialization,11 and higher demand due to a highly repetitive training regime.42 Therefore, considering the high prevalence of overuse injuries in team but especially in individual sports, future studies should investigate the effects of different strategies to reduce the occurrence and severity of overuse injuries in different types of sports.
Previous systematic reviews investigating prevalence of overuse injuries in athletes had methodological limitations, such as restricted language of publications,15,44,45 lack of protocol registration,15,45,46 and non-assessment of the strength of evidence.44 Moreover, no meta-analysis was performed with the purpose of estimating the prevalence of overuse injuries in individual and team sports, separately. The current systematic review with meta-analysis had its protocol prospectively registered in PROSPERO and the strength of the evidence evaluated using the GRADE system. The prevalence of overuse injuries in individual and team sports found in the present study differs from the prevalence reported in previous reviews,15,44 partially due to the different purposes of each review. For example, Kox et al.15 reviewed the studies about the prevalence of overuse injuries on the wrist of young athletes from different sports (e.g. gymnastics, field hockey, judo), and found prevalence rates varying from 10 to 28% in the different sports. On the other hand, Smith et al.44 reviewed studies reporting the prevalence of musculoskeletal injuries in amateur ballet dancers and found prevalence of 75% of overuse injuries. In addition, differences in overuse injury definition, inclusion criteria, and in procedures used to extract data might also explain the different number of studies included in each review. Therefore, considering the different focus and/or limitations demonstrated by previous systematic reviews on the topic, this review provides information on the prevalence of overuse injuries in individual and team sports.
Low-quality evidence of overuse injuries in individual and team sports suggests that future high-quality studies with clear and reliable definition and measurement of overuse injuries are likely to impact on the estimated prevalence. The strength of the current evidence was downgraded due to imprecision and inconsistency for period-prevalence. In addition, the sensitivity analysis performed in this review was not able to show that the prevalence of overuse injuries in specific body regions differ between individual and team sports.
This review has some limitations. First, we were not able to perform the meta-analysis and the sensitivity analysis pooling by sex and type of sport due to insufficient data in the included studies. Second, the methods used by the included studies to measure overuse injuries were heterogenous, because some studies used non-standard tools to collect overuse injuries prevalence data, which can under- or overestimate the prevalence of this type of injury. Future studies should use standard definitions of overuse injuries and also adopt standard tools to extract data on prevalence of overuse injuries to improve the quality of data. The results of this systematic review associated with the findings from studies about injury mechanisms can contribute to the development of injury prevention and rehabilitation programs and hopefully reduce the detrimental effects of overuse injuries on athletes’ participation and performance. Finally, caution must be taken with the generalization of the results to the modalities that were not covered by this systematic review. Therefore, future studies about the prevalence of overuse injuries in different individual and team sports might significantly influence on the estimated prevalence of overuse injuries.
ConclusionThis systematic review with meta-analysis showed that period-prevalence of overuse injuries was 42.0% in individual sports and 33.0% in team sports. Current low-quality evidence on period-prevalence suggests that the prevalence is likely to change with future high-quality studies.
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES - Finance Code 001). We are also thankful to the Fundação de Amparo á Pesquisa do Estado de Minas Gerais (FAPEMIG) and to the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPQ) (428735/2018-5).



