


Dyspnea is a relevant outcome to be taken into consideration during stroke rehabilitation. Prevalence, severity, and effects of this condition on individuals with stroke remain uncertain. This study investigated the prevalence and severity of dyspnea after a stroke, as well the associations between dyspnea, activity limitations, and participation restrictions.
MethodsA telephone-based survey was conducted with 285 individuals with stroke. The survey included information regarding the onset and severity of the dyspnea, activity limitations, and participation restrictions. Prevalence of dyspnea was reported as percentage of individuals who had the symptom. Chi-square tests were used to investigate the associations between dyspnea, activity limitations, and participation restrictions. Relative risks and respective 95% confidence intervals were calculated.
ResultsOut of the 285 participants, 124 (44%) reported having dyspnea after stroke. Severe symptoms were reported by 51% of the participants with dyspnea. In addition, dyspnea limited activity and restricted social participation in 85% and 49% of the participants, respectively. Dyspnea was significantly correlated with activity limitations (r=0.87; 95% CI 0.82–0.92; p<0.01) and participation restrictions (r=0.53; 95% CI 0.46–0.62; p<0.01). The analyses indicated that individuals with dyspnea were more likely to report that it limited their activities (RR: 6.5; 95% CI 4.3–9.9) and restricted social participation (RR: 1.7; 95% CI 1.5–2.0).
ConclusionsDyspnea is an important symptom after stroke and showed to be associated with activity limitations and restrictions in community participation. Earlier detection of dyspnea in people with stroke, followed by appropriate management, is strongly recommended and has the potential to improve activity and social participation.
Stroke is the second leading global cause of death and the main cause of disability worldwide.1 This condition affects not only the muscles of the upper and lower limbs, but also those of the respiratory system.2–4 Patients with stroke typically demonstrate atypical breathing patterns,4,5 decreased ventilatory function,6,7 weakness of the respiratory muscles,2,8 and reduced diaphragmatic activity.9,10 This abnormal respiratory function may lead to dyspnea in conditions of high and even under low effort demands, which in turn, may interfere with the performance of daily activities and community participation.2–4,8,11
Although dyspnea is seldom the predominant complaint in patients with primary neuromuscular diseases,12 it may be a significant symptom in patients, who show generalized muscle weakness, such as people who suffered a stroke. Weakness of the respiratory muscles, associated with sedentary lifestyles and deconditioning, may increase dyspnea after stroke, increase the risk of hospital admissions due to respiratory complications, which are the leading causes of non-vascular deaths after stroke.13,14
Multiple aspects related to dyspnea, such as the prevalence, severity, and frequency have been investigated in the general community and in several health conditions, such as lung diseases and heart failure.15–18 Quoted prevalence rates for dyspnea vary widely for the general community (1–32%),15 lung diseases (55%),16 chronic obstructive pulmonary disease (82%),17 and heart failure (47%).18 This variability suggests that dyspnea may be influenced by characteristics, such as age, clinical diagnosis, comorbidities, levels of physical activity, and, therefore, investigation of this relevant symptom should be, at least, disease-specific. It is also known that dyspnea negatively interferes with the ability to perform everyday activities and reduces the perceived quality of life of older individuals and people with respiratory diseases.15,19,20 Although dyspnea seems to be a clinically relevant outcome to be taken into consideration during rehabilitation,21–23 its prevalence, severity, and effects on the stroke population remain unclear. This information is required to help planning effective interventions, which could help minimizing the effects of dyspnea on daily activity and social participation. Due to the respiratory muscle weakness and sedentary lifestyles adopted by most individuals with stroke,13 it was expected that the prevalence of dyspnea would be high in individuals with stroke, compared to those of the general population.
Therefore, the aims of the present study were to investigate the prevalence and severity of dyspnea after stroke, as well the associations between dyspnea, activity limitations, and participation restrictions. The specific research questions were:
- 1.
What is the prevalence and level of severity of dyspnea in people, who suffered a stroke?
- 2.
Is dyspnea associated with activity limitations and/or participation restrictions?
For this cross-sectional, observational study, a telephone-based survey was conducted with individuals with stroke. Participants were recruited from the admission lists of stroke care units of two major public hospitals, from March 2016 to June 2017 and were included if they were ≥20 years of age and at least three months after the onset of the stroke. Individuals, who were screened to participate in a randomized clinical trial on the effects of respiratory muscle training after stroke,24 were also recruited and interviewed by telephone. The participants, who were unable to answer simple questions via telephone, such as their names and ages, were excluded. This study was approved by the Institutional Research Ethical Committee Review Board Universidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil (CAAE: 40290114.8.0000.5149) and all participants provided written consent.
InterviewA telephone-based survey was developed by the research team. Two researchers (M.T.M.A. and P.R.A) were trained to conduct the telephone interviews from a script, and practiced with 10 healthy individuals, to ensure consistency, since dyspnea is often thought of as a sensation similar to pain, which avoids an objective definition assessment.25 The survey consisted of questions regarding demographics, characteristics of the stroke, dyspnea and its relation with activity performance and social participation (Table 1). For the presence of dyspnea, individuals were questioned if they began to have the symptom after the stroke. Specific questions included the severity of dyspnea, which was measured using the Medical Research Council scale. The Medical Research Council is a five-point rating scale, simple to administer, based upon the patient's perceptions of dyspnea, while walking distances on level or climbing stairs,26 which is significantly correlated with other dyspnea scales.27 Participants answers were categorized as mild (score=1), moderate (scores 2 and 3), and severe (scores 4 and 5).28 Additional questions included the frequency, use of medications, and number of hospital admissions. Lastly, participants were asked to inform whether dyspnea limited their activity performance and/or social participation (Yes/No).
Statistical analyses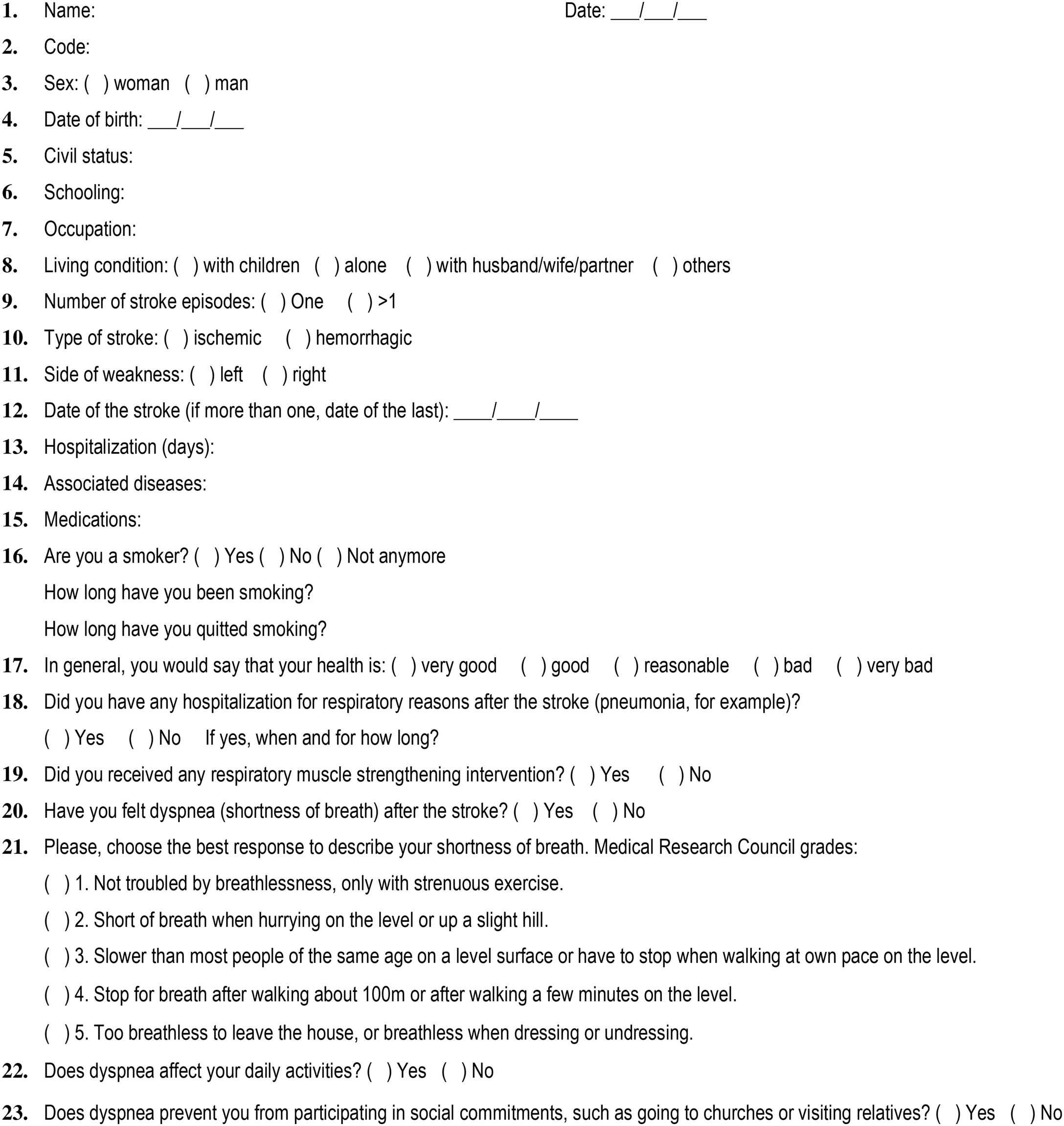
Descriptive statistics, tests for normality (Kolmogorov–Smirnov), and homogeneity of variance (Levene) were carried out for all outcomes. The prevalence of dyspnea was calculated as the percentage of individuals, who reported having dyspnea after the stroke. Dyspnea, activity limitations, and participation restrictions were dichotomized (Yes/No). Chi-square tests were used to investigate the directions and magnitudes of the correlations, as well as the relative risks, along with respective 95% confidence intervals. All analyses were performed with the SPSS statistical software 23.0 for Windows.
ResultsParticipant's characteristicsOut of 523 contacts, a total of 285 individuals (55%), 155 men, participated. The main reasons for non-participation were not answering the phone, wrong telephone number, refusals, or deaths. The characteristics of all participants, as well as those who had and not had dyspnea, are reported in Table 2. The mean age of the participants was 65 years (SD 14) and the mean time since the onset of the stroke was 15 months (SD 12). The majority had ischemic stroke (81%) and reported more than one episode of stroke (70%).
Characteristics of the participants.
| With dyspnean=124 | Without dyspnean=161 | Overalln=285 | |
|---|---|---|---|
| Age (years), mean (SD) | 66 (13) | 65 (14) | 65 (14) |
| Sex, men, number (%) | 57 (46) | 98 (61) | 155 (54) |
| Time since stroke (months), mean (SD) | 17 (14) | 14 (10) | 15 (12) |
| Number of episodes, number (%) | |||
| 1 | 78 (63) | 123 (76) | 82 (29) |
| >1 | 45 (36) | 37 (23) | 201 (70) |
| Unknown | 1 (1) | 1 (1) | 2 (1) |
| Type of stroke, number (%) | |||
| Ischemic | 96 (77) | 136 (85) | 232 (81) |
| Hemorrhagic | 13 (11) | 8 (5) | 21 (8) |
| Unknown | 15 (12) | 17 (10) | 32 (11) |
| Side of weakness, number (%) | |||
| Right | 52 (42) | 57 (35) | 109 (38) |
| Left | 46 (37) | 72 (45) | 118 (42) |
| Both | 2 (2) | 1 (1) | 3 (1) |
| Unknown | 24 (19) | 31 (19) | 55 (19) |
| Associated diseases, number (%)a | |||
| Hypertension | 105 (85) | 124 (77) | 229 (80) |
| Diabetes | 43 (35) | 48 (30) | 91 (32) |
| Hypercholesterolemia | 34 (27) | 35 (22) | 69 (24) |
| Asthma/Bronchitis/COPD | 6 (5) | 5 (3) | 11 (4) |
| Others | 37 (30) | 32 (20) | 69 (24) |
| Number of medications, mean (SD) | 4 (3) | 3 (3) | 4 (3) |
| Smoking, yes, number (%) | 10 (8) | 18 (11) | 28 (10) |
| Smoking time (years), mean (SD) | 27 (15) | 43 (17) | 38 (18) |
| No longer smoking, number (%) | 60 (48) | 70 (44) | 130 (46) |
| Quitted smoking (years), mean (SD) | 15 (16) | 19 (17) | 17 (16) |
Out of the 285 participants, 124 (44%) reported having dyspnea after the stroke. Out of the 124 participants, who had dyspnea, 16 (13%) reported mild, 45 (36%) moderate, and 63 (51%) severe dyspnea. In addition, 105 participants (85%) informed that dyspnea limited their daily activities, whereas 51 (49%) informed that dyspnea restricted their social participation.
Associations between dyspnea, activity limitations, and participation restrictionsDyspnea was significantly correlated with activity limitations (r=0.87; 95% CI 0.82–0.92; p<0.01) and participation restrictions (r=0.53; 95% CI 0.46–0.62; p<0.01). The analyses indicated that individuals, who had dyspnea, were more likely to report activity limitations (RR: 6.5; 95% CI 4.3–9.9) and restricted social participation (RR: 1.7; 95% CI 1.5–2.0).
DiscussionThis study aimed at investigating the prevalence and severity of dyspnea, as well as the associations between dyspnea, activity limitations, and participation restrictions in people, who had a stroke, through a telephone-based survey. The prevalence of dyspnea was 44%. The majority of the respondents reported having moderate to severe dyspnea, which was associated with activity limitations and participation restrictions.
The present results indicated that almost half of the individuals reported some degree of dyspnea after the stroke. Furthermore, over half of the respondents reported severe dyspnea, which indicates the need to stop for breathing after few minutes of walking or breathless sensation during usual everyday activities, such as dressing.26 The high prevalence of dyspnea in people with stroke is worrying, since dyspnea has been shown to be a predictor of mortality related to heart attacks and stroke.29,30 Moreover, the high percentage of respondents with severe dyspnea turns on a warning signal, as the risk of deaths significantly increases in people, who have dyspnea of moderate and severe intensities.29,30 The results suggested that earlier detection and management of dyspnea in people with stroke requires attention and should not be under looked.
It is well known that stroke survivors have reduced cardiorespiratory fitness, and mobility.31,32 The present results also demonstrated that the majority of the participants, who had dyspnea, informed that it limited their activities and restricted their social participation. Participants, who had dyspnea, were six times more likely to report activity limitation and two times more likely to report restrictions in social participation. This vicious cycle, i.e., reduced activity and deconditioning, may result in increased dyspnea, which is recognized as a key contributor to functional decline, since dyspneic patients are frequently unable to perform daily life activities, such as walking, due to the discomfort associated with breathing.33 Furthermore, this reduced cardiovascular fitness associated with the biological changes in respiratory muscle may propagate components of the metabolic syndrome, conferring added morbidity and mortality risks.34
As dyspnea interferes with many everyday activities involving both the lower and upper limbs, it is not a surprise that perceived community-participation is restricted. For instance, if walking ability is poor (particularly walking speed, walking capacity, and ability to manage stairs) after stroke, community participation, which includes leisure activities and social interactions, is expected to be limited, and people may become housebound and isolated from society.35,36 Therefore, an early detection of dyspnea in people with stroke, and the application of effective interventions in the treatment of this symptom,8 has the potential to improve daily activities and social participation, and reduce the risk of recurrent stroke and deaths.29,30,34,37
The major strength of the present study is the innovation, since is the first to investigate dyspnea after stroke in a large sample. However, this study is not without limitations. Although the sample was broad and drawn from various settings, it was not randomly selected and may not, therefore, be fully representative of the stroke population. Since the recruitment was conducted on a volunteer basis, the participants who agreed to participate, may differ from those of the general community. In addition, a telephone-based survey may also hold some sources of bias. However, amongst numerous technological advances in medical care, the use of telephone for health care management has increased in scope and application,28 being the telephone-based surveys appropriate for many chronic disorders, including stroke.38 Furthermore, the Medical Research Council proved to be highly suitable for telephone-based surveys.28 Finally, information regarding levels of motor impairments and physical activity, use of assistive devices for walking, and participation in rehabilitation programs, which could better characterize the sample, was not collected.
ConclusionsIn conclusion, the prevalence of dyspnea after stroke was 44% and severe symptoms were reported by 51% of the participants, who had dyspnea. The presence of dyspnea was associated with activity limitations and restrictions in community participation. Earlier detection of dyspnea in people with stroke, followed by appropriate management, is strongly recommended and has the potential to improve daily activities and social participation.
Authors’ contributionsAll the authors contributed with the literature search, analysis of data, manuscript preparation, and review of manuscript.
FundingConselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq – grant number 304434/2014-0), Fundação de Amparo à Pesquisa de Minas Gerais (FAPEMIG – PPM 00006-14) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) – Brazil (código 001).
Conflicts of interestThe authors declare no conflicts of interest.



