







Office workers have the highest incidence of neck pain of all occupations. However, the relationship between symptoms and the risk factors is unclear.
ObjectiveTo examine the relationship between self-reported neck pain with a comprehensive range of individual and work-related risk factors.
MethodsThis study utilised a cross-sectional study design. Office workers with and without neck pain (n=763) were recruited. Participants completed a survey which included a Pain Numerical Rating Scale (dependent variable), and measures of independent variables including demographic, individual, work-related factors, neck/shoulder muscle strength, endurance, and range of motion (ROM). The relationships between the independent and dependent variables were analysed in a logistic regression model.
ResultsNeck pain was significantly associated with more senior occupational categories, working more than six hours per day on the computer, female sex, greater fear avoidance beliefs for work, greater psychological distress, and reduced cervical flexion ROM. The low severity of neck pain of the participants in this study may limit a robust determination of their association with the risk factor variables, but the studied sample is a realistic representation of the office worker population.
ConclusionSeveral potentially modifiable individual and work-related factors were identified to be associated with the presence of self-reported neck pain in office workers. Future studies will be needed to investigate whether strategies to alter these modifiable risk factors translate to changes in neck pain.
Trial registration: ACTRN12612001154897 (https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=363209)
Neck pain is a prevalent and chronic condition.1 In the Global Burden of Disease 2010 study, neck pain was ranked fourth highest for years lived with disability, and 21st for overall burden of disease.2 Neck pain is also a recurrent disorder with 60–80% of the working population experiencing another episode one year after the initial episode.3 As such, the cost of neck pain is substantial to society4 and to industry, where between 3 and 11% of lost-time claims were related to neck pain.5 Within industry, office workers have the highest incidence of neck disorders at 34–49% a year.1,6–8 There is also evidence that while the majority of workers who experience low severity neck pain may choose to remain at work rather than take sick leave,1,9 they may be less productive at work.10,11
The risk factors associated with neck pain are multifactorial, and may be broadly categorised into individual (e.g. health behaviour, psychological distress) and work-related factors (e.g. computer hours per day at work, physical demand at work, job control).1 Most studies have focused on the associations between a select number of risk factors and neck pain, rather than comprehensively including the individual and work-related factors.7,12–15 Furthermore, when physical risk factors (such as neck/shoulder muscle strength/endurance and range of motion) were measured, the sample sizes were small and not specific to office workers.16–20
The purpose of this study was to explore the relationships between a comprehensive list of individual and work-related factors, and self-reported neck pain in a large population of office workers. We hypothesise that the presence of neck pain will have significant relationships with the individual and work-related factors. It is anticipated that the findings of this study will clarify our understanding of potentially modifiable risk factors that contribute to self-reported neck pain in office workers.
MethodsStudy design and ethicsThis study utilised the baseline data of a two-arm parallel prospective clustered randomised trial (ACTRN12612001154897) and followed the STROBE guidelines for reporting observational data.21 All participants provided informed consent, and ethical approval was granted by the University of Queensland's Human Medical Research Ethics Committee (2012001318), Brisbane, Australia.
ParticipantsParticipants (n=763) were recruited from 14 private and public organisations in Brisbane, Queensland, Australia from May 2013 to July 2015. The organisations were involved in various industries including mining, medical appliances, government, legal, and engineering. The sample size was based on the original randomised trial in which this study is nested.22 Eligible participants were 18 years of age or older, and worked more than 30h/week in predominantly sedentary office work (i.e. computer work). Participants were excluded if they were pregnant, suffered from specific pathologies (e.g. congenital cervical abnormalities, stenosis), inflammatory conditions (e.g. rheumatoid arthritis), or had a history of cervical spine surgery. Office workers with and without neck pain and neck disability were included to enable comparison.
Outcome measuresThe dependent variable, neck pain intensity, was evaluated with a ten-point Pain Numerical Rating Scale ranging from 0 (no pain) to nine (worst possible pain) during the last three months (on average).23 A body map based on the Nordic questionnaire was used to identify the neck region.23 Participants’ age, sex and Body Mass Index (BMI) were included as covariates.
A series of physical measures were collected from all participants at the workplace. The order of testing of these measures was randomised between participants to avoid order effects. Inter and intra-rater reliability for the different assessors was determined with the order of testing of all reliability tests randomised.
Cervical range of motion (ROM) was assessed with a Cervical ROM (CROM) device (CROM 3 from Performance Attainment Associates) and included active cervical flexion, extension (Fig. 1A), and bilateral rotation (Fig. 1B). Participants were instructed to perform the ROM tests as far as they could and not past discomfort or pain. Each movement was repeated until three subsequent results of the same value were obtained and the mean recorded as the final score. This is a valid and reliable method for assessing CROM.24–27
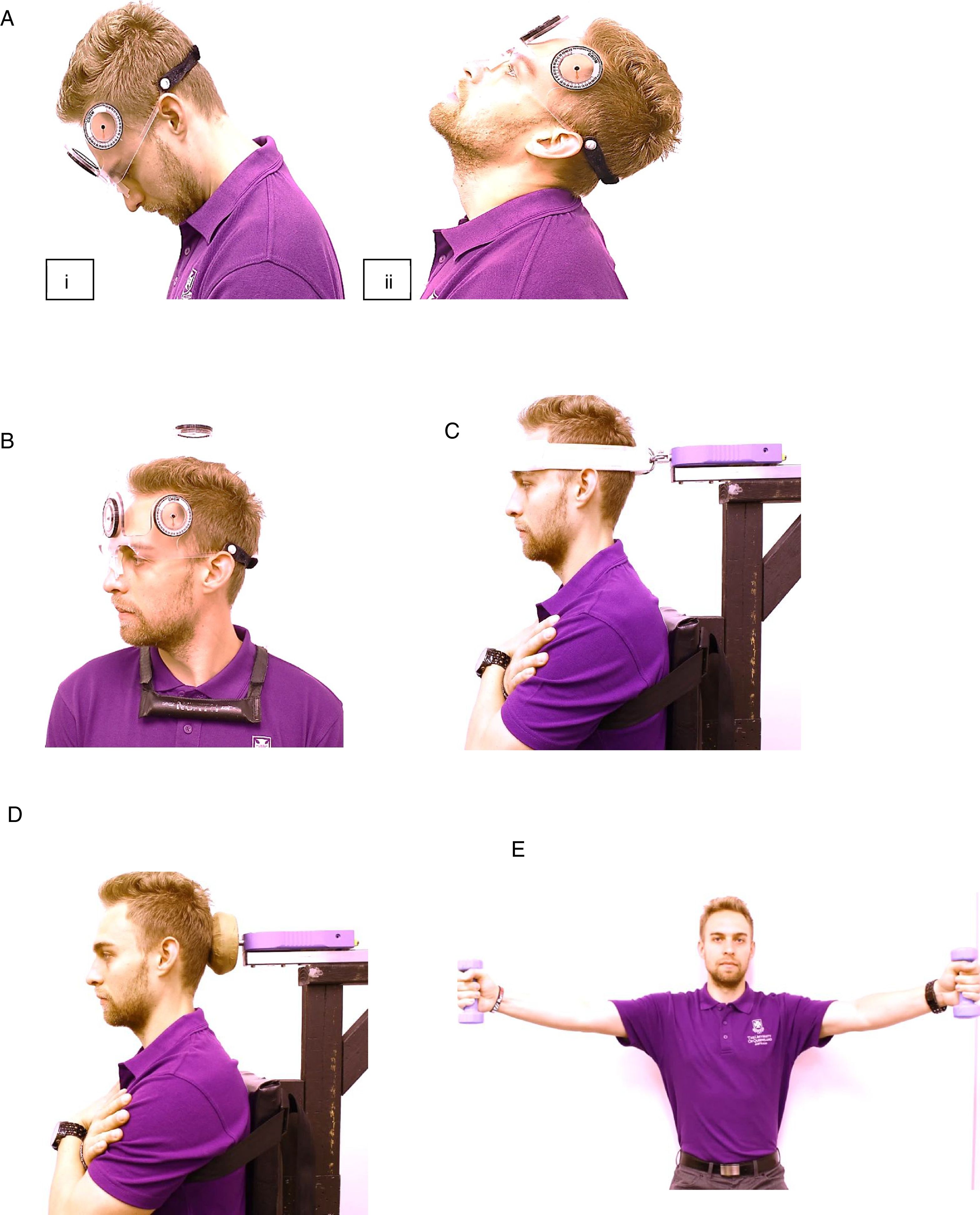
(A) (i) Cervical flexion and (ii) extension range of motion tests. (B) Cervical rotation range of motion test. (C) Neck flexor maximum strength and endurance muscle test position. (D) Neck extensor maximum strength and endurance muscle test position. (E) Position for shoulder lift strength and endurance test.
Maximum isometric neck flexor (Fig. 1C) and extensor (Fig. 1D) muscle strength (kgf) and endurance (seconds) was recorded. Participants were seated with a digital dynamometer mounted onto a rigid arm adjusted to suit participant anthropometrics. Strength tests were repeated thrice with a thirty second rest period between repetitions. Endurance was evaluated with a sustained contraction at 50% of maximum strength until the participant indicated the contraction could no longer sustain the hold. During testing, participants performed a standardised warm up (two submaximal contractions), and received standard verbal and visual (computer screen demonstrating live force performance) feedback. The participants were instructed to inform the investigator if they experienced discomfort or pain during the test at which point the test was terminated. Isometric neck strength and endurance tests have previously demonstrated good reliability.28–32
Bilateral shoulder strength was measured in kilograms (kgf) using dumbbells with a one repetition maximum (1RM) test (Fig. 1E). Bilateral shoulder endurance was recorded as the number of repetitions the participant could perform using the same shoulder lift technique with a weight one kilogram less than their 1RM.33–35 These methods of shoulder strength and endurance testing were replicated from previous trials as a general test for the function of the neck/shoulder musculature.33–35 The participants were instructed to perform the shoulder tests to their maximal capacity and to cease the test if they experienced discomfort or pain. In the instance where there was better performance in one arm compared to the other, results were recorded for the arm that recorded the poorer performance.
Self-reported data on the individual and work-related risk factors was collected via an online survey. Information about the highest level of education achieved and total number of comorbidities were collected from participants. Quality of Life (QOL) was measured using Assessment of QOL (AQOL) 6D, a valid and reliable measure consisting of 20 questions (six dimensions: independent living, relationships, mental health, coping, pain and senses), with higher scores indicating higher QOL (0–1 minimum to maximum).36 Psychological distress was evaluated with the short-form K6 questionnaire (six questions) which has excellent internal consistency and reliability.37 The K6 has a 0–4 scale for each of the six items, with zero being “none of the time”, and four being “all of the time” for questions related to how much of the time participants experienced specific feelings (e.g. “nervous”, “hopeless”).38 Higher scores indicate higher psychological distress (0–24 minimum to maximum).38,39
Fear avoidance beliefs for physical activity and work were assessed using three items from the fear avoidance belief questionnaire.40,41 Response options were on a seven-point scale from “completely disagree” (score of zero) to “completely agree” (score of seven). Participants were considered to hold fear avoidance beliefs for physical activity if they completely agreed with these statements: “physical activity should be avoided when in pain”, and “I should not do physical activities which (might) make my pain worse”. Participants would hold fear-avoidance beliefs for work if they agreed with this statement: “pain in the neck and shoulders is commonly caused by work”.40,41 These questions have been used to identify fear avoidance beliefs for neck pain in a sample of health workers.40
Exercise self-efficacy was measured via a single question “I am confident that I am able to exercise at least 20min three times or more a week even though…”, with a total of six items to complete the question each scored on a five-point Likert scale from “not at all confident (score of one)” to “completely confident (score of five)”.42–44 Examples of the items included “…I’m under a lot of stress”, “…I feel I don’t have the time”, and “…I have to exercise alone”. The score on each item was summed with a higher total score indicative of higher exercise self-efficacy.42–44
Self-reported physical activity was assessed with the International Physical Activity Questionnaire (IPAQ) (short form) which has been shown to be a valid and reliable tool.45 Participants were deemed to have met the recommended guidelines for physical activity if they met any of the following criteria: (a) performed vigorous intensity exercise at least 20min/day, three days/week, (b) performed moderate intensity activity 30min/day, five days/week, or (c) performed exercises on five or more days of any combination of walking, moderate/vigorous intensity activities of a minimum of 600 MET-min/week.46 Participants were deemed as having exceeded the recommended guidelines for physical activity if they met any of the following criteria: (a) performed vigorous intensity exercise at least three days/week achieving at least 1500 MET-min/week, or (b) performed at least seven days of any combination of walking, moderate-intensity or vigorous intensity activities, achieving at least 3000 MET-min/week. Participants were considered as “does not meet guidelines” if they did not meet the criteria for “meets guidelines” or “exceeds guidelines” as described above.46
Participants’ reported their occupation based on the following categories “Category 1” (i.e. manager or senior official), “Category 2” (professional, associate professional, technical, or others) and “Category 3” (administrative, secretarial, or personal services).47 Information about the type of industry participants worked (e.g. private, state government) was also obtained. Participants also reported their total hours worked in the last seven days, and number of computer hours at work per day.
Work-related psychosocial factors were evaluated using the JCQ (short-form), consisting of 18 items across four domains including psychological job demands (three items), physical job demands (two items), job control (nine items), and social support from supervisors and colleagues (four items).48,49 This instrument is commonly used to assess psychosocial stressors at work and is based on the demand-control-support (DCS) model.49 The total score for each domain was used for analysis.
Job Satisfaction was measured using Kunin faces on a seven-point response rating scale from “extremely dissatisfied” (score of one) to “extremely satisfied” (score of seven),50,51 with the mean used for statistical analysis.
An ergonomic assessment of the workstation was performed for each participant by a trained physical or occupational therapist, with each assessment lasting 30–45min. The ergonomic assessment consisted of a checklist of seven sub-categories including chair, desk, monitor, keyboard, mouse, telephone and the physical environment.52 The checklist has good to moderate inter-rater reliability.52 Each of the seven sub-categories consisted of a positive or negative outcome. The maximum total ergonomic score possible was 38, with a higher score relating to a better workstation setup. In this study, the seven subcategories were collapsed into a total ergonomic score for ease of analysis.
ProcedureAn online survey (hosted by Qualtrics®) was used to collect data on neck pain intensity, as well as demographic (i.e. age, sex, BMI) and neck paid related measures (pain medication intake and health professional help sought for neck/shoulder symptoms), individual, and work-related factors. All physical measures (neck/shoulder ROM, muscle strength and endurance) were collected at the participant's workplace at a pre-arranged time. The time between completion of the survey and physical measures for each participant was one to two weeks.
Reliability of physical testsThe intra-rater reliability of the physical measures performed in this study was examined in 30 separate participants with and without neck pain, and who did not participate in the main study (age, mean (SD): 39 (13.8), sex: 19 females, 11 males, neck pain intensity last three months, mean (SD): 1.37 (1.9)) overseen by one of the investigators (XC) who is a qualified physical therapist and conducted the majority of the physical measures (87% total) in the overall study. For intra-rater reliability, tests were performed by this investigator (XC) on two separate sessions spaced one to two weeks apart. Due to the large participant numbers in the study, two other trained physical therapists also oversaw some measurement sessions (13% total). Therefore, their inter-rater reliability (with XC) was evaluated in 13 of the 30 participants. All assessors were registered physical therapists with at least two years of clinical experience in Australia. The inter and intra-rater reliability testing were conducted in the Cervical Spine & Whiplash Research Unit laboratory at the University of Queensland. The test sequences were randomised, and repeated a week after each session. The testers were blinded to each other's data entries.
Statistical analysesThe scores for neck pain intensity were dichotomized so that participants could be appropriately allocated into the “No Pain” (score of zero) or “Pain” (score >0) groups.53–55 The decision to dichotomize the pain intensity variable rather than analyse as a continuous variable was that scores were not normally distributed and transformation did not improve the distribution. Univariate logistic regression was used to examine the relationships between the presence of pain, and independent variables, with age, sex and BMI as covariates. Independent variables shown to have a significant univariate relationship (exit p≤0.10)53 with pain were retained for backwards logistic regression modelling. The regression model was tested for the assumptions of collinearity using variance inflation factor (VIF) and goodness of fit using Pearson χ2. Severe collinearity was assumed to be present if VIF>10.56,57 In addition, univariate multinomial regression was used to examine the relationships between a more senior occupational category, and selected individual and work-related risk factors in a post hoc analysis. Statistical analysis was performed using STATA/IC (version 15.0). A p<0.05 was accepted as statistically significant.
ResultsParticipant characteristics are presented in Table 1. The overall response rate from the 14 organisations was 21%, with 763 of 3571 potential participants recruited into the trial. Of these participants, three withdrew, six were excluded due to not meeting eligibility criteria, and 13 discontinued participation after group allocation into the trial, leaving 741 participants’ baseline data being available for analysis. Due to technical issues with the online survey, the neck pain intensity data for one participant was not recorded, leaving a total of 740 participants constituting the sample in this study.
Participant characteristics of office workers with and without neck paina (n=740).
| Variables | No pain (n=281) | Pain (n=459) |
|---|---|---|
| Age (years) | ||
| Mean (SD) | 43.59 (10.76) | 42.13 (10.62) |
| Sex (n, %) | ||
| Male | 127 (17.16) | 162 (21.89) |
| Female | 154 (20.81) | 297 (40.14)** |
| Body Mass Index (kg/m2) Mean (SD) | 27.58 (5.88) | 26.72 (5.65)* |
| Pain medication taken last 4 weeks for neck/shoulder symptoms | ||
| Yes (n, %) | 13 (1.76) | 112 (15.14)** |
| No (n, %) | 268 (36.22) | 347 (46.89) |
| Healthcare professional seen last 12 months for neck/shoulder symptoms | ||
| Yes (n, %) | 37 (5.00) | 191 (25.81)** |
| No (n, %) | 244 (32.97) | 268 (36.22) |
%, cell percentages.
The intra- and inter-rater reliability coefficients of the physical measures were performed on 30 participants and overseen by the main measurement investigator (XC). All physical measures were shown to have excellent intra-rater test–retest reliability (intra-class correlation co-efficient (ICC) range 0.80–0.96) (Type ICC (2,k)). All inter-rater reliability results were also excellent (ICC range 0.81–0.97), except for cervical flexor endurance at ICC of 0.69 (good), and cervical right and left rotation range of motion (ICC range 0.46–0.49) (fair).58
Neck painParticipants with neck pain (n=459) (62%) reported mean (SD) pain intensity of 3.13 (1.81) and median (min-max) of 3 (1–8). There was a significantly higher proportion of females with neck pain than males (p<0.01). BMI was significantly lower for those in the Pain group (p<0.05). There was a significantly high proportion of participants in the Pain group taking pain medications and seeking healthcare professional management for their neck/shoulder symptoms than the No Pain group.
Univariate regression analysis found several individual factors to be significantly higher (psychological distress, fear avoidance beliefs for work) or lower (QOL, exercise self-efficacy, cervical flexion ROM, cervical flexor, extensor and shoulder lift muscle strength) in the Pain group compared to the No Pain group (p≤0.10). Participants who had the highest level of education in trade college, and not meeting the IPAQ guidelines were also associated with Pain (p≤0.10). Similarly, the Pain group showed a significant univariate relationship with several work-related factors (the more senior occupational categories, private and local government industries, working on the computer more than six hours per day, and reduced job satisfaction) compared to No Pain group (p≤0.10) (Table 2).
Comparison between office workers with and without neck paina (n=740).
| Variables | No Pain (n=281) | Pain (n=459) | Odds Ratio (95% CI) | p valueb |
|---|---|---|---|---|
| Individual factors, mean (SD) | ||||
| Physical measures | ||||
| Cervical flexion ROM (degrees) | 62.51 (9.93) | 61.29 (9.84) | 0.99 (0.97–1.00) | 0.10 |
| Cervical extension ROM (degrees) | 66.02 (12.54) | 66.73 (13.24) | 1.00 (0.99–1.02) | 0.47 |
| Cervical right rotation ROM (degrees) | 63.97 (10.23) | 64.52 (9.74) | 1.00 (0.99–1.02) | 0.48 |
| Cervical left rotation ROM (degrees) | 65.14 (10.50) | 65.63 (9.35) | 1.01 (0.99–1.02) | 0.51 |
| Cervical flexor muscle strength (kg) | 13.97 (6.07) | 12.31 (5.45) | 0.95 (0.93–0.98) | <0.01 |
| Cervical flexor muscle endurance (s) | 42.01 (19.34) | 41.16 (20.80) | 0.99 (0.99–1.01) | 0.58 |
| Cervical extensor muscle strength (kg) | 19.14 (7.14) | 17.49 (7.01) | 0.97 (0.95–0.98) | <0.01 |
| Cervical extensor muscle endurance (s) | 88.97 (61.91) | 88.10 (62.55) | 0.99 (0.99–1.00) | 0.86 |
| Shoulder lift muscle strength (kg) | 7.29 (3.20) | 6.63 (3.11) | 0.94 (0.89–0.98) | <0.01 |
| Shoulder lift endurance (repetitions) | 9.86 (4.44) | 10.18 (4.80) | 1.01 (0.98–1.05) | 0.37 |
| Individual factors | ||||
| Others | ||||
| Highest level of education, n(%) | ||||
| Primary to Year 12 | 70 (9.46) | 97 (13.11) | Reference | Reference |
| University | 174 (23.51) | 282 (38.11) | 1.17 (0.82–1.68) | 0.40 |
| Trade College | 37 (5.00) | 80 (10.81) | 1.56 (0.95–2.56) | 0.08 |
| Comorbidities (total number), mean (SD) | 0.63 (0.94) | 0.64 (0.88) | 1.01 (0.86–1.19) | 0.88 |
| Psychological distress (K6), mean (SD) | 3.06 (2.96) | 4.14 (3.42) | 1.11 (1.06–1.17) | <0.01 |
| Quality of life (AQOL), mean (SD) | 0.86 (0.11) | 0.81 (0.13) | 0.02 (0.01–0.08) | <0.01 |
| Fear avoidance beliefs (work), mean (SD) | 2.98 (1.69) | 3.77 (1.56) | 1.35 (1.23–1.48) | <0.01 |
| Fear avoidance beliefs (physical activity), mean (SD) | 7.52 (3.21) | 7.33 (3.05) | 0.98 (0.93–1.03) | 0.42 |
| Exercise self-efficacy, mean (SD) | 22.43 (5.93) | 21.23 (5.59) | 0.96 (0.94–0.99) | 0.01 |
| IPAQ, n(%) | ||||
| Does not meet guidelines | 87 (11.76) | 167 (22.57) | 1.32 (0.96–1.84) | 0.09 |
| Meets guidelines | 166 (22.43) | 240 (32.43) | Reference | Reference |
| Exceeds guidelines | 28 (3.78) | 52 (7.03) | 1.28 (0.78–2.12) | 0.33 |
| Work-related factors, mean (SD) | ||||
| Occupation categoryc, n(%) | ||||
| Category 1 | 48 (6.49) | 94 (12.70) | 1.52 (0.99–2.33) | 0.06 |
| Category 2 | 123 (16.62) | 223 (30.14) | 1.40 (1.01–1.96) | 0.05 |
| Category 3 | 110 (14.86) | 142 (19.19) | Reference | Reference |
| Industry, n(%) | ||||
| Other | 37 (5.00) | 42 (5.68) | Reference | Reference |
| Private | 67 (9.05) | 130 (17.57) | 1.71 (1.00–2.91) | 0.05 |
| State government | 122 (16.49) | 187 (25.27) | 1.35 (0.82–2.22) | 0.24 |
| Federal government | 40 (5.41) | 61 (8.24) | 1.34 (0.74–2.44) | 0.33 |
| Local government | 15 (2.03) | 39 (5.27) | 2.29 (1.09–4.81) | 0.03 |
| Hours worked altogether last 7 days, mean (SD) | 39.77 (9.97) | 39.54 (9.13) | 0.99 (0.98–1.01) | 0.75 |
| Computer hours per day at work, n(%) | ||||
| Less than 6h | 58 (7.84) | 66 (8.92) | Reference | Reference |
| 6h or more | 223 (30.14) | 393 (53.11) | 1.55 (1.05–2.29) | 0.03 |
| JCQ (social support), mean (SD) | 15.66 (2.52) | 15.42 (2.56) | 0.96 (0.91–1.02) | 0.22 |
| JCQ (psychological demand), mean (SD) | 8.49 (2.54) | 8.74 (2.53) | 1.04 (0.98–1.10) | 0.19 |
| JCQ (physical demand), mean (SD) | 3.33 (1.28) | 3.30 (1.30) | 0.98 (0.88–1.10) | 0.79 |
| JCQ (job control), mean (SD) | 21.65 (3.24) | 21.32 (3.53) | 0.97 (0.93–1.02) | 0.20 |
| Job satisfaction, mean (SD) | 5.10 (1.10) | 4.83 (1.13) | 0.80 (0.69–0.92) | <0.01 |
| Total ergonomic score, mean (SD) | 31.72 (3.02) | 31.78 (3.00) | 1.01 (0.96–1.06) | 0.82 |
Participants were dichotomized into No Pain (0 out of 9) and Pain (>0 out of 9) for pain intensity on average last 3 months.
Category 1 (manager, or senior official), Category 2 (professional, associate professional, technical or others), Category 3 (administrative, secretarial, or personal services).
%, cell percentage; IPAQ, International Physical Activity Questionnaire; JCQ, Job Content Questionnaire; ROM, range of motion; N/A, not applicable.
Table 3 displays the final regression model for neck pain. The results for collinearity (mean VIF 1.10) and goodness of fit (p>0.05) were satisfactory. In order of strength of relationship, the presence of neck pain was significantly associated with more senior occupational categories (Categories 1 and 2), performing more than six hours of computer work per day, female sex, greater fear avoidance beliefs for work, greater psychological distress, and reduced cervical flexion ROM.
Risk factors associated with the presence of neck pain (adjusted for age, sex and body mass index) (n=740).
| Predictors | OR (95% CI) | p value |
|---|---|---|
| Occupation categorya | ||
| Category 1 | 2.31 (1.42–3.76) | <0.01 |
| Category 2 | 1.48 (1.02–2.13) | 0.04 |
| Category 3 | Reference | Reference |
| Computer hours worked per day | ||
| Less than 6h | Reference | Reference |
| 6h or more | 1.61 (1.06–2.46) | 0.03 |
| Female sex | 1.49 (1.06–2.10) | 0.02 |
| Fear avoidance beliefs for work | 1.30 (1.18–1.44) | <0.01 |
| Psychological distress (K6) | 1.11 (1.05–1.18) | <0.01 |
| Cervical flexion range of motion | 0.98 (0.96–1.00) | 0.02 |
As occupational category demonstrated a strong relationship with the presence of neck pain, further analysis was conducted to better understand the potential contributors to this relationship. It appears that a more senior occupational category was significantly associated with higher job control, higher job satisfaction and less than six hours of computer use. However, working in a more senior occupational role was also associated with working longer hours per week, and higher psychological demand (p≤0.01) (Table 4).
Post hoc analysis of the univariate relationships between occupational categories and the independent variables, adjusted for age and sex (n=740).
| Predictors | RRR (95% CI) for Occupation Category 1a | RRR (95% CI) for Occupation Category 2a |
|---|---|---|
| Individual factors | ||
| Psychological distress (K6) | 0.96 (0.89–1.03) | 0.99 (0.94–1.05) |
| Quality of life (AQOL) | 3.69 (0.61–22.13) | 0.91 (0.24–3.46) |
| Fear avoidance beliefs (work) | 0.98 (0.86–1.11) | 1.09 (0.98–1.20) |
| Fear avoidance beliefs (physical activity) | 0.94 (0.88–1.01) | 1.02 (0.96–1.07) |
| Exercise self-efficacy | 1.03 (1.00–1.07) | 1.00 (0.97–1.03) |
| Work-related factors | ||
| Computer hours per day at work | ||
| Less than 6h | 2.29 (1.35–3.90)* | 1.03 (0.64–1.67) |
| 6h or more | Reference | Reference |
| Hours worked altogether last 7 days | 1.06 (1.03–1.09)* | 0.99 (0.98–1.01) |
| JCQ (job control) | 1.56 (1.43–1.72)* | 1.13 (1.07–1.19)* |
| JCQ (psychological demand) | 1.27 (1.16–1.39)* | 1.02 (0.95–1.10) |
| Job satisfaction | 1.37 (1.12–1.67)* | 1.07 (0.92–1.25) |
| JCQ (physical demand) | 0.86 (0.71–1.03) | 1.12 (0.98–1.27) |
| JCQ (social support) | 1.04 (0.96–1.14) | 1.00 (0.93–1.06) |
The findings of this study support our hypothesis that several individual and work-related factors influence the presence of neck pain in office workers, most of which are modifiable. In order of the strength of relationship, the presence of neck pain was significantly associated with the more senior occupational categories, working more than six hours on the computer per day, female sex, the belief that work may cause neck pain (fear avoidance), greater psychological distress, and reduced cervical flexion ROM. Overall these findings that have been derived from a large sample of office workers from multiple organisations, suggesting that the aetiology and persistence of neck pain in office workers may be influenced by multiple factors. These factors include those that are specific to work but also some that are specific to the individual worker. Importantly some of these factors are potentially modifiable, providing some insight into how neck pain in the most common of occupations, office work, may be addressed.
Our findings support the evidence from epidemiological studies that female office workers have a higher risk of having neck pain than men.1,6,59,12 However, our findings did not support previous reports indicating an increased incidence of neck pain with age.1 Of the previous studies investigating the association between greater fear avoidance beliefs for work and neck pain in workers, only one study on hospital nurses was found to support our findings.40 Our findings were also supported by previous studies which reported significant associations between higher mental7 or psychological6 stress and neck pain in office workers, albeit the available studies did not utilise the same measurement tool (i.e. K6) as in the present study. An association has also previously been shown between reduced cervical flexion ROM and neck pain,6,17,19 in contrast to another study on female office workers (where no significant associations were found).18 The latter study was however potentially confounded as the results were based on a smaller sample size, and crude associations using univariate correlation statistics.1,18
Interestingly our post hoc analysis revealed that despite senior office workers spending reduced hours at a computer, they still reported working on average 44h per week, which is five hours longer than the other workers. In contrast, a previous study reported significant proportion of employees in the higher level management and professional occupational categories working longer computer hours per day.60 The study, however, quantified neck pain in terms of incidence proportion, using pain during the last 12 months as the case definition.60 Nonetheless, our findings (increased time at computer for less senior workers, and longer work hours for senior workers) may indicate that it is the long duration of work (and perhaps the inability to unwind) that impacts perceived neck pain in senior office workers, rather than the nature of work itself. Of further interest our post hoc analysis also showed that office workers in more senior positions had significantly higher psychological demand, job control, yet greater job satisfaction than other employees, which is supported by previous evidence.61 Thus cumulatively our results indicate that higher psychological demand and longer hours spent at work were associated with neck pain in the more senior office workers, but it is possible that these negative aspects of work are buffered by better job control resulting in higher job satisfaction. Further studies are required to substantiate our findings.
Study limitationsSymptomatic participants in this study had a relatively low severity of pain (numerical rating scale median of 3/9 points) and therefore some limitations may exist with robustly determining an association with other variables.62 However, it was a population specific study and our large sample most probably represents a realistic profile of this targeted population. The results are specific to the office worker population and caution should be taken to generalising findings to other occupational groups especially where the task demands are different. Additionally, while results may explain associative links between neck pain and the individual and work-related risk factors examined, causation between these associations cannot be inferred.
Study strengthsThis study analysed a comprehensive battery of risk factors that included where possible quantifiable measures that were recorded on-site. The findings of the study have implications from a clinical and industry perspective as some of the factors shown to have a relationship with pain are potentially modifiable. Therefore, interventions to address some of these modifiable factors may be of potential benefit in reducing the burden of neck disorders in office workers in the future.
ConclusionSeveral potentially modifiable individual and work-related factors were identified to be associated with the presence of self-reported neck pain in office workers. Future studies will be needed to investigate whether strategies to alter these modifiable risk factors translate to changes in neck pain.
FundingThis study is funded by the National Health and Medical Research Council (NHMRC) (Fund approval number APP1042508) and the Australian Postgraduate Award.
Authors’ contributionAll authors have made substantial contribution to the conception and design, data acquisition, data analysis and interpretation, writing and revision of the paper, and approved the final version for submission.
Ethical approvalAll procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of interestsThe authors declare no conflict of interests.
The research would not have been possible without support from the participating companies, the on-site liaisons, and the research participants – the authors would like to thank all who have been involved.



