



Upper extremity Physical Performance Tests (PPTs) have been used in sports contexts to provide functional status of the athletes. However, whether these tests present appropriate measurement properties to be considered a valuable measurement is not clear.
ObjectiveTo systematically review the measurement properties of upper extremity PPTs in athletes.
MethodsDatabases (e.g., Medline, EMBASE, CINAHL, SPORTDiscus, CENTRAL) were searched in March 2021. Two reviewers independently rated the methodological quality using the 4-point Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) checklist. Quality of evidence was graded by measurement property for each test, considering the adequacy, the sample size, and the methodological quality of the studies.
ResultsFifteen studies were included with a pooled sample of 684 athletes. The PPTs analyzed were Arm-Jump Board Test, Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST), Finger Hang Test, Medicine Ball Explosive Power Test, One-Arm Hop Test, Posterior Shoulder Endurance Test, Pull-Up Shoulder Endurance Test, Repetition to Failure Assessment, Seated Medicine Ball Throw Test (SMBT), Seated Single-Arm Shot-Put Test (SSPT), Shoulder Endurance Test, Two-Arm Bent Hang Test, Unilateral Seated Shot-Put Test, and Upper Limb Rotation Test. Evidence synthesis provided moderate and high-quality evidence for sufficient inter-session and intra-session reliability of the CKCUEST, respectively. There was moderate evidence for sufficient inter-session reliability of the SSPT and for insufficient validity of the SMBT.
ConclusionThe CKCUEST and the SSPT are sufficiently reliable in athletes. More studies are needed to investigate other psychometric properties for these tests and other upper extremity PPTs.
Physical performance-based tests (PPTs) are routinely used in sports rehabilitation and prevention to assess physical function related to sports demand, such as strength, power, and agility,1 and provide functional status of the athletes.1–3 PPTs are a low-tech, not time-consuming, portable, and easy-to-administer way of assessment that can be performed in different environments with minimal material.2,3
The International Olympic Committee recommends that screening tests must be reliable, with appropriate sensitivity and specificity, affordable, easy to perform, and widely available.4 The PPTs for the lower limb have been extensively investigated and some PPTs have appropriate measurement properties.3,5,6 In contrast, studies on upper extremity PPTs are scarce with limited evidence related to measurement properties.2 In 2016, a systematic review identified eleven studies that examined the measurement properties of six upper extremity PPTs,2 and only two showed moderate positive evidence for reliability and one for validity. Nevertheless, recent studies have been published and updated information on the evidence of upper extremity PPTs is needed to guide clinicians and researchers in the assessment of athletes.
Therefore, the purpose of this systematic review is to summarize and analyze the current evidence regarding the measurement properties of upper extremity PPTs in athletes.
MethodsThis systematic review followed the PRISMA checklist7 and was prospectively registered at PROSPERO (CRD 42021241883).
Search methods for identification of studiesElectronic searches were performed in Medline (via Ovid), EMBASE, CINAHL, Cochrane Central Register for Controlled Trials (CENTRAL), SCOPUS, SPORTdiscus, and Web of Science, from inception up to July 2022. Keywords related to PPTs, athletes, upper extremity, and measurement properties were combined and adjusted for each database (Supplementary material 1). The reference lists from the included articles were screened to identify potentially relevant studies.
Study selectionTwo reviewers independently analyzed titles and abstracts of the retrieved publications and, thereafter, analyzed full texts, according to eligibility criteria. The selection process was conducted by consensus, and a third reviewer was consulted in case of disagreement using the software State of the Art through Systematic Review.
Eligibility criteriaParticipantsStudies were included if they assessed athletes or participants enrolled in any sports practice of any sport from both sexes, without restrictions related to age, level of sports practice (e.g., recreational, high school level, semi-professional, and professional), and presence of injury.
Type of studiesStudies with any design and language that verified the measurement properties of upper extremity PPTs in athletes were included. PPTs were defined as assessments that measure constructs related to muscle strength and power, agility, endurance, flexibility, and readiness for return-to-play that stimulate activities or gestures of sports practice,2,5 using affordable, portable, and readily available equipment, with results reported as the number of repetitions, distance (centimeters or meters), or duration (seconds or minutes). Upper extremity was defined as the region spanning from shoulder girdle to the end of the fingers. Studies that investigated the measurement properties of technology-dependent instruments, including 2/3-dimensional motion analysis system, upper body ergometers, rowing ergometers, and dynamometer, were excluded.
Outcome measurePrimary studies were included if they reported one or more measurement properties, which were defined according to the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) taxonomy.8
Data extractionThree reviewers independently extracted the data and a fourth reviewer verified the data in case of discrepancies. A standardized form was used to extract the data, including information regarding characteristics of the study, participants, PPT, and measurement properties.
Methodology qualityTwo reviewers independently evaluated the methodological quality of each measurement property of the included studies, and a third author was consulted in case of discrepancies, using the COSMIN 4-point checklist,9,10 which scored as very good, adequate, doubtful, or inadequate. For scoring the quality of inter-session, intra-session, and inter-rater reliability studies, the item “assignment of the score or determination of the biological value” was not considered for analysis due to PPTs not involving biological samplings (e.g., blood and urine). Also, the item “administration of measurements” was not considered for intra-session reliability analysis, because the assessor would necessarily know the value previously obtained by that same participant when repeating that measurement. The total score was determined by taking the lowest score (worst score counts method).10
Quality criteria for measurement propertiesThe adequacy of measurement properties was assessed with the adapted version of Terwee et al.11 Each measurement property was rated as sufficient, insufficient, or indeterminate (Supplementary material 2).
Grading the quality of the evidenceThe quality of evidence (QoE) was graded by measurement property for each PPT, according to previous systematic reviews (Supplementary material 3).12–14
ResultsStudy selectionThe literature search retrieved 11,163 studies and, of those, 5262 were duplicates, which resulted in 5901 for assessment. The assessment of title and abstract excluded 5878 because the included individuals were not athletes, or individuals were not enrolled in sports practice, and/or measurement properties of PPTs were not assessed. Twenty-three were considered in the full-text assessment and 15 studies were included (Fig. 1).16–30
Characteristics of the primary studies
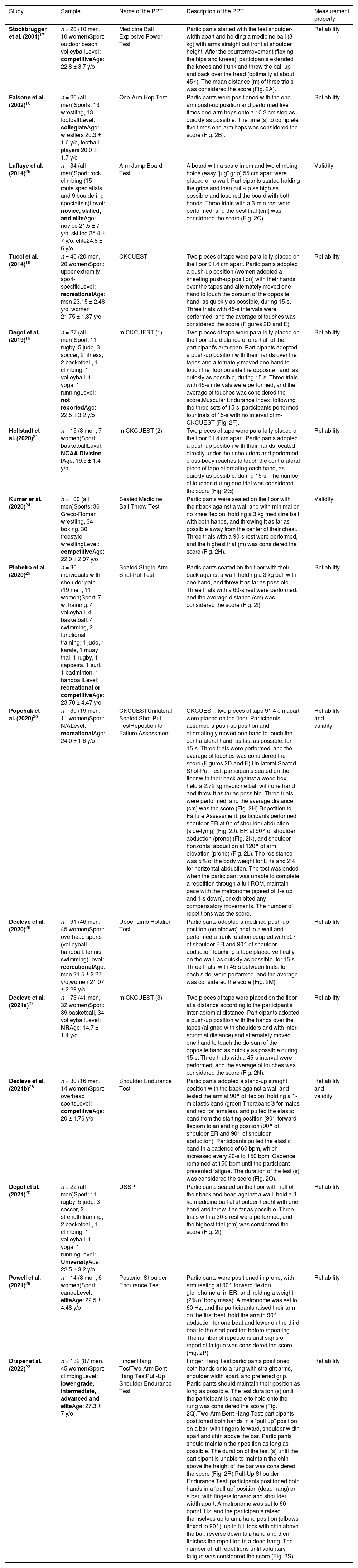
The characteristics of included studies are described in Table 1. The number of athletes in each study ranged from 14 to 132 (pooled sample: 684; 70.6% men) and the mean age of 22.0 ± 3.1 years, which ranged from 14.7 ± 1.4 to 27.3 ± 7 years old.
Data extraction of the included studies.
| Study | Sample | Name of the PPT | Description of the PPT | Measurement property |
|---|---|---|---|---|
| Stockbrugger et al. (2001)17 | n = 20 (10 men, 10 women)Sport: outdoor beach volleyballLevel: competitiveAge: 22.8 ± 3.7 y/o | Medicine Ball Explosive Power Test | Participants started with the feet shoulder-width apart and holding a medicine ball (3 kg) with arms straight out front at shoulder height. After the countermovement (flexing the hips and knees), participants extended the knees and trunk and threw the ball up and back over the head (optimally at about 45°). The mean distance (m) of three trials was considered the score (Fig. 2A). | Reliability |
| Falsone et al. (2002)16 | n = 26 (all men)Sports: 13 wrestling, 13 footballLevel: collegiateAge: wrestlers 20.3 ± 1.6 y/o, football players 20.0 ± 1.7 y/o | One-Arm Hop Test | Participants were positioned with the one-arm push-up position and performed five times one-arm hops onto a 10.2 cm step as quickly as possible. The time (s) to complete five times one-arm hops was considered the score (Fig. 2B). | Reliability |
| Laffaye et al. (2014)25 | n = 34 (all men)Sport: rock climbing (15 route specialists and 9 bouldering specialists)Level: novice, skilled, and eliteAge: novice 21.5 ± 7 y/o, skilled 25.4 ± 7 y/o, elite24.8 ± 6 y/o | Arm-Jump Board Test | A board with a scale in cm and two climbing holds (easy “jug” grip) 55 cm apart were placed on a wall. Participants started holding the grips and then pull-up as high as possible and touched the board with both hands. Three trials with a 3-min rest were performed, and the best trial (cm) was considered the score (Fig. 2C). | Validity |
| Tucci et al. (2014)18 | n = 40 (20 men, 20 women)Sport: upper extremity sport-specificLevel: recreationalAge: men 23.15 ± 2.48 y/o, women 21.75 ± 1.37 y/o | CKCUEST | Two pieces of tape were parallelly placed on the floor 91.4 cm apart. Participants adopted a push-up position (women adopted a kneeling push-up position) with their hands over the tapes and alternately moved one hand to touch the dorsum of the opposite hand, as quickly as possible, during 15-s. Three trials with 45-s intervals were performed, and the average of touches was considered the score (Figures 2D and E). | Reliability |
| Degot et al. (2019)19 | n = 27 (all men)Sport: 11 rugby, 5 judo, 3 soccer, 2 fitness, 2 basketball, 1 climbing, 1 volleyball, 1 yoga, 1 runningLevel: not reportedAge: 22.5 ± 3.2 y/o | m-CKCUEST (1) | Two pieces of tape were parallelly placed on the floor at a distance of one-half of the participant's arm span. Participants adopted a push-up position with their hands over the tapes and alternately moved one hand to touch the floor outside the opposite hand, as quickly as possible, during 15-s. Three trials with 45-s intervals were performed, and the average of touches was considered the score.Muscular Endurance Index: following the three sets of 15-s, participants performed four trials of 15-s with no interval of m-CKCUEST (Fig. 2F). | Reliability |
| Hollstadt et al. (2020)21 | n = 15 (8 men, 7 women)Sport: basketballLevel: NCAA Division IAge: 19.5 ± 1.4 y/o | m-CKCUEST (2) | Two pieces of tape were parallelly placed on the floor 91.4 cm apart. Participants adopted a push-up position with their hands located directly under their shoulders and performed cross-body reaches to touch the contralateral piece of tape alternating each hand, as quickly as possible, during 15-s. The number of touches during one trial was considered the score (Fig. 2G). | Reliability |
| Kumar er al. (2020)24 | n = 100 (all men)Sports: 36 Greco-Roman wrestling, 34 boxing, 30 freestyle wrestlingLevel: competitiveAge: 22.9 ± 2.97 y/o | Seated Medicine Ball Throw Test | Participants were seated on the floor with their back against a wall and with minimal or no knee flexion, holding a 3 kg medicine ball with both hands, and throwing it as far as possible away from the center of their chest. Three trials with a 90-s rest were performed, and the highest trial (m) was considered the score (Fig. 2H). | Validity |
| Pinheiro et al. (2020)29 | n = 30 individuals with shoulder pain (19 men, 11 women)Sport: 7 wt training, 4 volleyball, 4 basketball, 4 swimming, 2 functional training; 1 judo, 1 karate, 1 muay thai, 1 rugby, 1 capoeira, 1 surf, 1 badminton, 1 handballLevel: recreational or competitiveAge: 23.70 ± 4.47 y/o | Seated Single-Arm Shot-Put Test | Participants seated on the floor with their back against a wall, holding a 3 kg ball with one hand, and threw it as far as possible. Three trials with a 60-s rest were performed, and the average distance (cm) was considered the score (Fig. 2I). | Reliability |
| Popchak et al. (2020)30 | n = 30 (19 men, 11 women)Sport: N/ALevel: recreationalAge: 24.0 ± 1.6 y/o | CKCUESTUnilateral Seated Shot-Put TestRepetition to Failure Assessment | CKCUEST: two pieces of tape 91.4 cm apart were placed on the floor. Participants assumed a push-up position and alternatingly moved one hand to touch the contralateral hand, as fast as possible, for 15-s. Three trials were performed, and the average of touches was considered the score (Figures 2D and E).Unilateral Seated Shot-Put Test: participants seated on the floor with their back against a wood box, held a 2.72 kg medicine ball with one hand and threw it as far as possible. Three trials were performed, and the average distance (cm) was the score (Fig. 2H).Repetition to Failure Assessment: participants performed shoulder ER at 0° of shoulder abduction (side-lying) (Fig. 2J), ER at 90° of shoulder abduction (prone) (Fig. 2K), and shoulder horizontal abduction at 120° of arm elevation (prone) (Fig. 2L). The resistance was 5% of the body weight for ERs and 2% for horizontal abduction. The test was ended when the participant was unable to complete a repetition through a full ROM, maintain pace with the metronome (speed of 1-s up and 1-s down), or exhibited any compensatory movements. The number of repetitions was the score. | Reliability and validity |
| Decleve et al. (2020)26 | n = 91 (46 men, 45 women)Sport: overhead sports (volleyball, handball, tennis, swimming)Level: recreationalAge: men 21.5 ± 2.27 y/o;women 21.07 ± 2.29 y/o | Upper Limb Rotation Test | Participants adopted a modified push-up position (on elbows) next to a wall and performed a trunk rotation coupled with 90° of shoulder ER and 90° of shoulder abduction touching a tape placed vertically on the wall, as quickly as possible, for 15-s. Three trials, with 45-s between trials, for each side, were performed, and the average was considered the score (Fig. 2M). | Reliability |
| Decleve et al. (2021a)27 | n = 73 (41 men, 32 women)Sport: 39 basketball, 34 volleyballLevel: NRAge: 14.7 ± 1.4 y/o | m-CKCUEST (3) | Two pieces of tape were placed on the floor at a distance according to the participant's inter-acromial distance. Participants adopted a push-up position with the hands over the tapes (aligned with shoulders and with inter-acromial distance) and alternately moved one hand to touch the dorsum of the opposite hand as quickly as possible during 15-s. Three trials with a 45-s interval were performed, and the average of touches was considered the score (Fig. 2N). | Reliability |
| Decleve et al. (2021b)28 | n = 30 (16 men, 14 women)Sport: overhead sportsLevel: competitiveAge: 20 ± 1.76 y/o | Shoulder Endurance Test | Participants adopted a stand-up straight position with the back against a wall and tested the arm at 90° of flexion, holding a 1-m elastic band (green Theraband® for males and red for females), and pulled the elastic band from the starting position (90° forward flexion) to an ending position (90° of shoulder ER and 90° of shoulder abduction). Participants pulled the elastic band in a cadence of 60 bpm, which increased every 20-s to 150 bpm. Cadence remained at 150 bpm until the participant presented fatigue. The duration of the test (s) was considered the score (Fig. 2O). | Reliability and validity |
| Degot et al. (2021)20 | n = 22 (all men)Sport: 11 rugby, 5 judo, 3 soccer, 2 strength training, 2 basketball, 1 climbing, 1 volleyball, 1 yoga, 1 runningLevel: UniversityAge: 22.5 ± 3.2 y/o | USSPT | Participants seated on the floor with half of their back and head against a wall, held a 3 kg medicine ball at shoulder-height with one hand and threw it as far as possible. Three trials with a 30-s rest were performed, and the highest trial (cm) was considered the score (Fig. 2I). | Reliability |
| Powell et al. (2021)29 | n = 14 (8 men, 6 women)Sport: canoeLevel: eliteAge: 22.5 ± 4.48 y/o | Posterior Shoulder Endurance Test | Participants were positioned in prone, with arm resting at 90° forward flexion, glenohumeral in ER, and holding a weight (2% of body mass). A metronome was set to 60 Hz, and the participants raised their arm on the first beat, hold the arm in 90° abduction for one beat and lower on the third beat to the start position before repeating. The number of repetitions until signs or report of fatigue was considered the score (Fig. 2P). | Reliability |
| Draper et al. (2022)23 | n = 132 (87 men, 45 women)Sport: climbingLevel: lower grade, intermediate, advanced and eliteAge: 27.3 ± 7 y/o | Finger Hang TestTwo-Arm Bent Hang TestPull-Up Shoulder Endurance Test | Finger Hang Test:participants positioned both hands onto a rung with straight arms, shoulder width apart, and preferred grip. Participants should maintain their position as long as possible. The test duration (s) until the participant is unable to hold onto the rung was considered the score (Fig. 2Q).Two-Arm Bent Hang Test: participants positioned both hands in a “pull up” position on a bar, with fingers forward, shoulder width apart and chin above the bar. Participants should maintain their position as long as possible. The duration of the test (s) until the participant is unable to maintain the chin above the height of the bar was considered the score (Fig. 2R).Pull-Up Shoulder Endurance Test: participants positioned both hands in a “pull up” position (dead hang) on a bar, with fingers forward and shoulder width apart. A metronome was set to 60 bpm/1 Hz, and the participants raised themselves up to an l-hang position (elbows flexed to 90°), up to full lock with chin above the bar, reverse down to l-hang and then finishes the repetition in a dead hang. The number of full repetitions until voluntary fatigue was considered the score (Fig. 2S). | Reliability |
Abbreviations: °, degrees; bpm, beats per minute; CKCUEST, Closed Kinetic Chain Upper Extremity Stability Test; cm, centimeters; ER, external rotation; Hz, Hertz; kg, kilograms; m, meters; m-CKCUEST, modified CKCUEST; min, minutes; NCAA, National Collegiate Athletic Association; PPT, Physical Performance Test; s, seconds.
Different PPTs were investigated by the primary studies (Table 1 and Fig. 2 (A-S)). The results of reliability data and measurement error are described in Table 2 and the results of the validity data described in Table 3. Methodological quality and quality criteria for rating the results are described in Supplementary material 4 and 5, respectively.
; One-Arm Hop Test (B); Arm-Jump Board Test (C); Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) (men position) (D); CKCUEST (women position) (E); Modified CKCUEST – 1 (F); Modified CKCUEST – 2 (G); Seated Medicine Ball Throw Test (H); Seated Single-Arm/Unilateral Seated Shot-Put Test (I); Repetition to Failure Assessment: external rotation (ER) at 0° of shoulder abduction (side-lying -J); ER at 90° of shoulder abduction (prone - K); and shoulder horizontal abduction at 120° of arm elevation (prone - L); Upper Limb Rotation Test (M) Modified CKCUEST – 3 (N); Shoulder Endurance Test (O); Posterior Shoulder Endurance Test (P); Finger Hang Test (Q); Two-Arm Bent Hang Test (R); Pull-Up Shoulder Endurance Test (S).")
Physical performance tests. Medicine Ball Explosive Power Test (A); One-Arm Hop Test (B); Arm-Jump Board Test (C); Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) (men position) (D); CKCUEST (women position) (E); Modified CKCUEST – 1 (F); Modified CKCUEST – 2 (G); Seated Medicine Ball Throw Test (H); Seated Single-Arm/Unilateral Seated Shot-Put Test (I); Repetition to Failure Assessment: external rotation (ER) at 0° of shoulder abduction (side-lying -J); ER at 90° of shoulder abduction (prone - K); and shoulder horizontal abduction at 120° of arm elevation (prone - L); Upper Limb Rotation Test (M) Modified CKCUEST – 3 (N); Shoulder Endurance Test (O); Posterior Shoulder Endurance Test (P); Finger Hang Test (Q); Two-Arm Bent Hang Test (R); Pull-Up Shoulder Endurance Test (S).
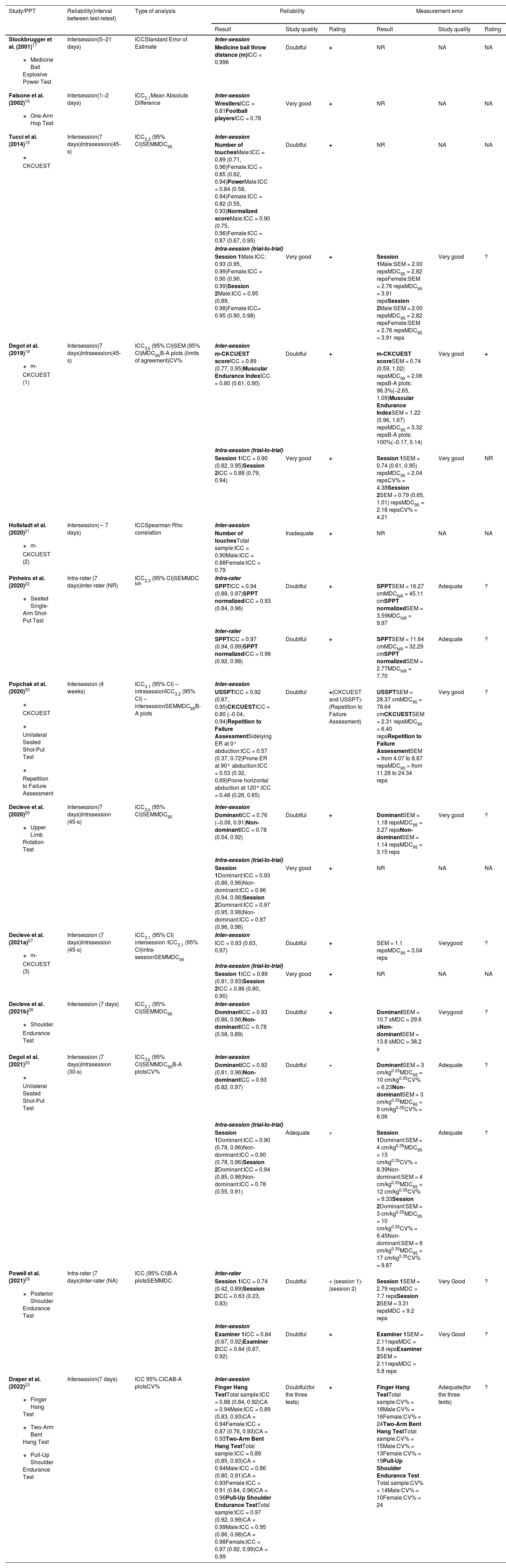
Results of the included studies that assessed reliability and measurement error.
| Study/PPT | Reliability(interval between test-retest) | Type of analysis | Reliability | Measurement error | ||||
|---|---|---|---|---|---|---|---|---|
| Result | Study quality | Rating | Result | Study quality | Rating | |||
Stockbrugger et al. (2001)17
| Intersession(5–21 days) | ICCStandard Error of Estimate | Inter-session | |||||
| Medicine ball throw distance (m)ICC = 0.996 | Doubtful | + | NR | NA | NA | |||
Falsone et al. (2002)16
| Intersession(1–2 days) | ICC2,1Mean Absolute Difference | Inter-session | |||||
| WrestlersICC = 0.81Football playersICC = 0.78 | Very good | + | NR | NA | NA | |||
Tucci et al. (2014)18
| Intersession(7 days)Intrasession(45-s) | ICC2,3 (95% CI)SEMMDC95 | Inter-session | |||||
| Number of touchesMale:ICC = 0.89 (0.71, 0.96)Female:ICC = 0.85 (0.62, 0.94)PowerMale:ICC = 0.84 (0.58, 0.94)Female:ICC = 0.82 (0.55, 0.93)Normalized scoreMale:ICC = 0.90 (0.75, 0.96)Female:ICC = 0.87 (0.67, 0.95) | Doubtful | + | NR | NA | NA | |||
| Intra-session (trial-to-trial) | ||||||||
| Session 1Male:ICC: 0.93 (0.95, 0.99)Female:ICC = 0.90 (0.90, 0.99)Session 2Male:ICC = 0.95 (0.89, 0.98)Female:ICC= 0.95 (0.90, 0.98) | Very good | + | Session 1Male:SEM = 2.00 repsMDC95 = 2.82 repsFemale:SEM = 2.76 repsMDC95 = 3.91 repsSession 2Male:SEM = 2.00 repsMDC95 = 2.82 repsFemale:SEM = 2.76 repsMDC95 = 3.91 reps | Very good | ? | |||
Degot et al. (2019)19
| Intersession(7 days)Intrasession(45-s) | ICC3,k (95% CI)SEM (95% CI)MDC95B-A plots (limits of agreement)CV% | Inter-session | |||||
| m-CKCUEST scoreICC = 0.89 (0.77, 0.95)Muscular Endurance IndexICC = 0.80 (0.61, 0.90) | Doubtful | + | m-CKCUEST scoreSEM = 0.74 (0.59, 1.02) repsMDC95 = 2.06 repsB-A plots: 96.3%(−2.65, 1.09)Muscular Endurance IndexSEM = 1.22 (0.96, 1.67) repsMDC95 = 3.32 repsB-A plots: 100%(−0.17, 0.14) | Very good | + | |||
| Intra-session (trial-to-trial) | ||||||||
| Session 1ICC = 0.90 (0.82, 0.95)Session 2ICC = 0.88 (0.79, 0.94) | Very good | + | Session 1SEM = 0.74 (0.61, 0.95) repsMDC95 = 2.04 repsCV% = 4.38Session 2SEM = 0.79 (0.65, 1.01) repsMDC95 = 2.18 repsCV% = 4.21 | Very good | NR | |||
Hollstadt et al. (2020)21
| Intersession(∼ 7 days) | ICCSpearman Rho correlation | Inter-session | |||||
| Number of touchesTotal sample:ICC = 0.90Male:ICC = 0.88Female:ICC = 0.79 | Inadequate | + | NR | NA | NA | |||
Pinheiro et al. (2020)22
| Intra-rater (7 days)Inter-rater (NR) | ICC2,3 (95% CI)SEMMDC NR | Intra-rater | |||||
| SPPTICC = 0.94 (0.88, 0.97)SPPT normalizedICC = 0.93 (0.84, 0.96) | Doubtful | + | SPPTSEM = 16.27 cmMDCNR = 45.11 cmSPPT normalizedSEM = 3.59MDCNR = 9.97 | Adequate | ? | |||
| Inter-rater | ||||||||
| SPPTICC = 0.97 (0.94, 0.99)SPPT normalizedICC = 0.96 (0.92, 0.98) | Doubtful | + | SPPTSEM = 11.64 cmMDCNR = 32.29 cmSPPT normalizedSEM = 2.77MDCNR = 7.70 | Adequate | ? | |||
Popchak et al. (2020)30
| Intersession (4 weeks) | ICC3,1 (95% CI) – intrasessionICC3,2 (95% CI) – intersessionSEMMDC95B-A plots | Inter-session | |||||
| USSPTICC = 0.92 (0.87, 0.95)CKCUESTICC = 0.80 (−0.04, 0.94)Repetition to Failure AssessmentSidelying ER at 0° abduction:ICC = 0.57 (0.37, 0.72)Prone ER at 90° abduction:ICC = 0.53 (0.32, 0.69)Prone horizontal abduction at 120°:ICC = 0.48 (0.26, 0.65) | Doubtful | +(CKCUEST and USSPT)-(Repetition to Failure Assessment) | USSPTSEM = 28.37 cmMDC95 = 78.64 cmCKCUESTSEM = 2.31 repsMDC95 = 6.40 repsRepetition to Failure AssessmentSEM = from 4.07 to 8.87 repsMDC95 = from 11.28 to 24.34 reps | Very good | ? | |||
Decleve et al. (2020)26
| Intersession(7 days)Intrasession (45-s) | ICC2,k (95% CI)SEMMDC95 | Inter-session | |||||
| DominantICC = 0.76 (−0.06, 0.91)Non-dominantICC = 0.78 (0.54, 0.92) | Doubtful | + | DominantSEM = 1.18 repsMDC95 = 3.27 repsNon-dominantSEM = 1.14 repsMDC95 = 3.15 reps | Very good | ? | |||
| Intra-session (trial-to-trial) | ||||||||
| Session 1Dominant:ICC = 0.93 (0.86, 0.96)Non-dominant:ICC = 0.96 (0.94, 0.98)Session 2Dominant:ICC = 0.97 (0.95, 0.98)Non-dominant:ICC = 0.97 (0.96, 0.98) | Very good | + | NR | NA | NA | |||
Decleve et al. (2021a)27
| Intersession (7 days)Intrasession (45-s) | ICC3,1 (95% CI) intersession /ICC2,1 (95% CI)intra-sessionSEMMDC95 | Inter-session | |||||
| ICC = 0.93 (0.63, 0.97) | Doubtful | + | SEM = 1.1 repsMDC95 = 3.04 reps | Verygood | ? | |||
| Intra-session (trial-to-trial) | ||||||||
| Session 1ICC = 0.89 (0.81, 0.93)Session 2ICC = 0.86 (0.80, 0.90) | Very good | + | NR | NA | NA | |||
Decleve et al. (2021b)28
| Intersession (7 days) | ICC2,1 (95% CI)SEMMDC95 | Inter-session | |||||
| DominantICC = 0.93 (0.86, 0.96)Non-dominantICC = 0.78 (0.58, 0.89) | Doubtful | + | DominantSEM = 10.7 sMDC = 29.6 sNon-dominantSEM = 13.8 sMDC = 38.2 s | Verygood | ? | |||
Degot et al. (2021)20
| Intersession (7 days)Intrasession (30-s) | ICC3,k (95% CI)SEMMDC95B-A plotsCV% | Inter-session | |||||
| DominantICC = 0.92 (0.81, 0.96)Non-dominantICC = 0.93 (0.82, 0.97) | Doubtful | + | DominantSEM = 3 cm/kg0.35MDC95 = 10 cm/kg0.35CV% = 6.23Non-dominantSEM = 3 cm/kg0.35MDC95 = 9 cm/kg0.35CV% = 6.06 | Adequate | ? | |||
| Intra-session (trial-to-trial) | ||||||||
| Session 1Dominant:ICC = 0.90 (0.78, 0.96)Non-dominant:ICC = 0.90 (0.78, 0.96)Session 2Dominant:ICC = 0.94 (0.85, 0.98)Non-dominant:ICC = 0.78 (0.55, 0.91) | Adequate | + | Session 1Dominant:SEM = 4 cm/kg0.35MDC95 = 13 cm/kg0.35CV% = 8.39Non-dominant:SEM = 4 cm/kg0.35MDC95 = 12 cm/kg0.35CV% = 9.33Session 2Dominant:SEM = 3 cm/kg0.35MDC95 = 10 cm/kg0.35CV% = 6.45Non-dominant:SEM = 6 cm/kg0.35MDC95 = 17 cm/kg0.35CV% = 9.87 | Adequate | ? | |||
Powell et al. (2021)29
| Intra-rater (7 days)Inter-rater (NA) | ICC (95% CI)B-A plotsSEMMDC | Inter-rater | |||||
| Session 1ICC = 0.74 (0.42, 0.89)Session 2ICC = 0.63 (0.23, 0.83) | Doubtful | + (session 1)- (session 2) | Session 1SEM = 2.79 repsMDC = 7.7 repsSession 2SEM = 3.31 repsMDC = 9.2 reps | Very Good | ? | |||
| Inter-session | ||||||||
| Examiner 1ICC = 0.84 (0.67, 0.92)Examiner 2ICC = 0.84 (0.67, 0.92) | Doubtful | + | Examiner 1SEM = 2.11repsMDC = 5.8 repsExaminer 2SEM = 2.11repsMDC = 5.8 reps | Very Good | ? | |||
Draper et al. (2022)23
| Intersession(7 days) | ICC 95% CICAB-A plotsCV% | Inter-session | |||||
| Finger Hang TestTotal sample:ICC = 0.88 (0.84, 0.92)CA = 0.94Male:ICC = 0.89 (0.83, 0.93)CA = 0.94Female:ICC = 0.87 (0.76, 0.93)CA = 0.93Two-Arm Bent Hang TestTotal sample:ICC = 0.89 (0.85, 0.93)CA = 0.94Male:ICC = 0.86 (0.80, 0.91)CA = 0.93Female:ICC = 0.91 (0.84, 0.96)CA = 0.96Pull-Up Shoulder Endurance TestTotal sample:ICC = 0.97 (0.92, 0.99)CA = 0.99Male:ICC = 0.95 (0.86, 0.98)CA = 0.98Female:ICC = 0.97 (0.92, 0.99)CA = 0.99 | Doubtful(for the three tests) | + | Finger Hang TestTotal sample:CV% = 18Male:CV% = 16Female:CV% = 24Two-Arm Bent Hang TestTotal sample:CV% = 15Male:CV% = 13Female:CV% = 19Pull-Up Shoulder Endurance Test Total sample:CV% = 14Male:CV% = 10Female:CV% = 24 | Adequate(for the three tests) | ? | |||
Abbreviations: ‐, insufficient; ?, indeterminate; +, sufficient; B-A, Bland-Altman plots; CA, Cronbach Alpha; CI, Confidence Interval; CKCUEST, Closed Kinetic Chain Upper Extremity Stability Test; cm, centimeters; CV%, Coefficient of Variation; ICC, Intraclass Correlation Coefficient; m, meters; m-CKCUEST, Modified CKCUEST; MDC, Minimal Detectable Change; NA, not applicable; NR, not reported; PPT, Physical Performance Test; reps, repetitions; SEM, Standard Error of Measurements.
Results of the included studies that assessed validity.
| Study/PPT | Type of validity | Outcomes | Study quality | Rating | Type of analysis | Results |
|---|---|---|---|---|---|---|
Laffaye et al. (2014)25
| Concurrent validity | Outcomes collected with a 3D accelerometer:
| Doubtful | ? | T-testCorrelation analysis | T-test: non-significant differences between the Arm-Jump Board Test (distance reached) and the accelerometer (T [33] = 1.07) |
| Correlation of the Arm-Jump Board Test (distance reached) versus:Velocity: r = 0.43Time: r = −0.12Index of efficiency: r = 0.87Relative power: r = 0.70Absolute power: r = 0.68 | ||||||
| Low systematic bias = −0.88 cm or −1.25 %Low CI (−4.61 cm < 95 %CI < 2.70 cm) | ||||||
Kumar et al. (2020)24
| Concurrent validity | Absolute peak power for the upper body during theWAnT using a modified electromagnetically braked crank-arm ergometer | Adequate | – | Pearson's correlationOne sample t-testOne-sample Wilcoxon Signed-Rank TestLinear regression | Correlation of the SMBT x WAnT in:All sportsmen: r = 0.55 (p = 0.0002)Boxers: r = 0.5358 (p = 0.0011)Freestyle wrestlers: r = 0.4244 (p = 0.019)Greco-Roman wrestlers: r = 0.6448 (p = 0.012) |
| T-test: non-significant differences between the SMBT and the WAnT in boxers (T = −1.90), freestyle and greco-roman wrestlers (T = 0.13 and 0.69, respectively) and all sportsmen (T = −0.33). | ||||||
| Wilcoxon Signed-Rank Test: non-significant differences between the SMBT and the WAnT in boxers (p = 0.1348), freestyle and greco-roman wrestlers (p = 0.9354 and 0.5089, respectively) and all sportsmen (p = 0.7925). | ||||||
| Linear regression:All sportsmen: p = 0.99Boxers: p = 0.102Freestyle wrestlers: p = 0.192Greco-Roman wrestlers: p = 0.838 | ||||||
Popchak et al. (2020)30
| Concurrent validity | Isokinetic strength assessments for shoulder movements of external (ER) and internal rotation (IR) at 60°/second and 180°/second using Biodex | Very good | -CKCUEST+USSPT-Repetition to Failure Assessment | Pearson r Correlation Coefficient (95% CI) | Correlation of the CKCUEST (number of touches) versus:Isokinetic ER 60°: r = 0.57 (0.37, 0.72)Isokinetic ER 180°: r = 0.59 (0.39, 0.73)Isokinetic IR 60°: r = 0.55 (0.34, 0.70)Isokinetic IR 180°: r = 0.59 (0.40, 0.73) |
| Correlation of the USSPT versus:Isokinetic ER 180°: r = 0.81 (0.73, 0.86)Isokinetic IR 180°: r = 0.74 (0.64, 0.81) | ||||||
| Correlation of the Repetition to Failure Assessment (number of repetitions) in sidelying ER at 0° abduction versus:Isokinetic ER 60°: r = 0.25 (0.07, 0.41)Isokinetic ER 180°: r = 0.20 (0.02, 0.37) | ||||||
| Correlation of the Repetition to Failure Assessment (number of repetitions) in prone ER at 90° abduction versus:Isokinetic ER 60°: r = 0.37 (0.20, 0.51)Isokinetic ER 180°: r = 0.38 (0.21, 0.52) | ||||||
| Correlation of the Repetition to Failure Assessment (number of repetitions) in prone horizontal abduction at 120° versus:Isokinetic ER 60°: r = 0.41 (0.25, 0.55)Isokinetic ER 180°: r = 0.40 (0.23, 0.54) | ||||||
Decleve et al. (2021b)28
| Construct validity | Shoulder isometric rotational strength for IR and ER with a hand-held dynamometer | Very good | Spearman Rank test (range) | Correlations between Shoulder Endurance Test (time in seconds) x isometric IR and ER rotations (r = 0.309, 0.431) |
Abbreviations: ‐, insufficient; ?, indeterminate; +, sufficient; 3D, three-dimensional; CI, confidence interval; CKCUEST, Closed Kinetic Chain Upper Extremity Stability Test; ER, external rotation; IR, internal rotation; PPT, Physical Performance Test; SMBT, Seated Medicine Ball Throw; USSPT, Unilateral Seated Shot Put Test; WAnT, Wingate Anaerobic Test.
One study16 investigated the inter-session reliability in 20 competitive beach volleyball athletes. Reliability was classified as sufficient (ICC = 0.99) with methodological quality scored as doubtful.9,10 The QoE was rated as low due to the low number of studies, small sample size, and doubtful methodology quality.
One-Arm hop test (Fig. 2B)One study15 with 26 uninjured collegiate athletes investigated the intra-session reliability, which was classified as sufficient for 13 wrestlers (ICC = 0.81) and 13 football players (ICC = 0.78) and the methodological quality was rated as doubtful.9,10 The quality of the evidence was rated as low due to the low number of studies, small sample size, and doubtful methodology quality.
Arm-Jump board test (Fig. 2C)One study19 with 34 athletes investigated the concurrent validity using the velocity, time, index of efficiency, relative and absolute power, collected with a 3D accelerometer. Correlations varied from weak to strong and validity was classified as indeterminate. The methodological quality was scored as doubtful due to the lack of information about measurement properties of the 3D accelerometer.9,10 Based on the methodological quality and criteria for rating the results, no evidence is available for the validity of this test.
CKCUEST (Figures 2D, E, F, G, and N)Five studies21,24–26,28 reported the measurement properties of the CKCUEST. Two studies24,25 performed the test according to the original version described in the literature and three21,26,28 modified the distance between the hands or the duration or interval between the series. Three studies21,25,26 with a pooled sample size of 140 athletes investigated intra-session reliability, which was classified as sufficient (intraclass correlation coefficient [ICC] = 0.86–0.95). The methodological quality of those studies was scored as very good,9,10 which resulted in high QoE. Three studies (n = 140)21,25,26 presented intra-session standard error of measurement (SEM) and minimal detectable change (MDC), which were rated as indeterminate because the minimal important changes (MIC) have not been defined for the CKCUEST.
Five studies21,24–26,28 (n = 185 athletes) verified the inter-session reliability, which was rated as sufficient (ICC = 0.79–0.93). The methodological quality of those studies was scored as doubtful or inadequate9,10 and the QoE was moderate. Three studies21,24,26 (pooled sample size of 130) presented inter-session SEM and MDC, which were rated as indeterminate because these properties have not been defined for the CKCUEST.
One study24 investigated the concurrent validity of the CKCUEST against isokinetic shoulder external rotators (ER) and internal rotators (IR) strength, which was classified as insufficient validity due to a moderately positive correlation (r = 0.55 to 0.59). The methodological quality of the study was rated as very good,9,10 and the QoE was low due to small sample size (n = 30).
Seated medicine ball throw test (Fig. 2H)One study18 investigated the concurrent validity of this test against the absolute peak power for the upper body during the Wingate Anaerobic Test using a modified electromagnetically braked crank-arm ergometer. Correlations were moderately positive in boxers, freestyle wrestlers, and Greco-Roman wrestlers (r = 0.40–0.54), which resulted in insufficient validity. The methodological quality of the study was adequate and the QoE was moderate, based on a sample of 100 athletes.
Seated single-arm/unilateral seated shot-put test (Fig. 2I)Three studies24,27,29 named this same test differently, which were pooled for the evidence synthesis. The methodological quality of the studies was scored as doubtful9,10 for reliability due to the lack of information about the time interval,24,29 similar assessment conditions,29 and/or the administration of measurements.24,29
Inter-rater reliability was tested in 30 recreational or competitive athletes with shoulder pain from different sports.29 Although the reliability was sufficient (ICC = 0.97), the doubtful9,10 methodological quality and small sample size resulted in a low QoE. Inter-rater SEM and MDC were rated as indeterminate because the MIC have not been defined for this test.
The inter-session reliability, analyzed by three studies (n = 82 athletes),24,27,29 was classified as sufficient (ICC = 0.92–0.94). The methodological quality of those studies was rated as doubtful,9,10 which resulted in moderate QoE. Inter-session SEM and MDC were reported in cm by two studies24,29 and in cm/kg0.35 by one study,27 which were rated as indeterminate because the MIC have not been defined.
Intra-session reliability was tested in 22 male athletes from different sports.27 Reliability was considered sufficient in both sessions (ICC = 0.78 to 0.94), methodological quality was adequate9,10 and the QoE was low. Intra-rater SEM and MDC were rated as indeterminate because the MIC have not been defined (Table 2).
One study24 with 30 athletes investigated the concurrent validity of this test against isokinetic shoulder strength during ER and IR, which resulted in sufficient validity due to strong and positive correlations (r = 0.73 to 0.83). The methodological quality of the study was rated as very good,9,10 and the QoE was low due to small sample size.
Repetition to failure test (Fig. 2J, K, and L)One study24 with 30 recreational athletes investigated the inter-session reliability of the posterior shoulder muscles in three different test positions: i) sideling ER at 0° abduction, ii) prone ER at 90° abduction, and iii) prone horizontal abduction at 120°. Test-retest reliability was classified as insufficient (ICC = 0.48–0.57) and the methodological quality was scored as doubtful.9,10 The QoE was rated as low due to the low number of studies, small sample size, and doubtful methodology quality. The same study provided SEM and MDC95, which were rated as indeterminate because the MIC have not been defined.
This study24 has also investigated the concurrent validity of the Repetition to Failure Assessment against isokinetic shoulder ER and IR strength. The correlations were weakly positive (r = 0.20 to 0.40), which resulted in insufficient validity. Although the methodological quality was very good,9,10 the QoE was low due to small sample size (n = 30).
Upper limb rotation test (Fig. 2M)One study20 investigated the inter and intra-session reliability of this test in 91 uninjured recreational overhead athletes. Reliability was rated as sufficient (inter-session, ICC = 0.76–0.78; intra-session, ICC = 0.93–0.97), while the methodological quality was doubtful9,10 for inter-session reliability and very good for intra-session reliability. The QoE was rated as low for inter and intra-session reliability due to small sample size. The methodological quality of inter-session SEM and the MDC95 was very good,9,10 and no evidence was established for measurement error because the MIC have not been defined.
Shoulder endurance test (Fig. 2O)One study22 with 30 competitive overhead athletes investigated the inter-session reliability, that was rated as sufficient (ICC = 0.78–0.93) and the methodological quality was doubtful.9,10 The QoE was rated as low due to small sample size and doubtful methodological quality. The methodological quality for SEM and the MDC was very good,9,10no evidence was established for measurement error because the MIC have not been defined.
The construct validity was analyzed against shoulder isometric IR and ER strength. The correlation was weak and positive (r = 0.309 to 0.431), which led to sufficient validity because the hypothesis was established and confirmed. The methodological quality of the study was very good,9,10 and the QoE was low due to small sample size.
Posterior shoulder endurance test (Fig. 2P)One study23 with 12 elite canoeing athletes investigated the inter-rater and inter-session reliabilities. Inter-rater reliability was sufficient in session 1 (ICC = 0.74) and insufficient in session 2 (ICC = 0.63). The QoE was rated as conflicting due to the conflicting results and doubtful methodological quality.23 Inter-session reliability was sufficient (ICC = 0.84) and resulted in low-quality evidence due to the low number of studies, small sample size, and doubtful methodological quality.9,10 The methodological quality of inter-rater SEM and the MDC95 was very good9,10 and no evidence was established for measurement error because the MIC have not been defined.
Finger hang test (Fig. 2Q)One study17 assessed the inter-session reliability of the Finger Hang Test in 132 rock climbers and presented sufficient reliability (ICC = 0.86–0.88). The methodological quality was doubtful9,10 and QoE was low.
Two-Arm bent hang test (Fig. 2R)One study17 assessed the inter-session reliability of the Two-Arm Bent Hang Test in 132 rock climbers and presented sufficient reliability (ICC = 0.86–0.91). The methodological quality was doubtful9,10 and QoE was low.
Pull-Up shoulder endurance test (Fig. 2S)One study17 reported the inter-session reliability of this test in rock climbers. Reliability was considered sufficient (ICC = 0.95–0.97). The methodological quality was doubtful9,10 and QoE was low.
DiscussionThis review synthesized the current evidence about the measurement properties of PPTs to assess the upper extremity of athletes. Although the reliability was considered sufficient (ICC ≥ 0.70) for almost all upper extremity PPTs, the evidence synthesis was downgraded in most of the cases due to small sample sizes and doubtful methodological quality of the primary studies.9,10 The methodological quality of reliability studies was downgraded because of a lack of clarity about the knowledge of the assessor on the scores obtained in the previous session (on inter-session rehabilitation studies), as well as the absence of details about the setting that the instrument was administered (e.g. hospital, home, outpatient clinic, laboratory), and the given instructions for the test. Other factors, such as a wide range of time intervals between the test-retest measurements and the lack of information about the clinical stability of the athlete throughout the test-retest period negatively influenced the results. The CKCUEST was the only PPT that showed high and moderate QoE for intra and inter session reliability, respectively, and the Seated Single-Arm Shot-Put Test showed sufficient reliability. Tarara et al.2 showed moderate evidence that both tests are reliable. However, evidence about the reliability of other upper extremity PPTs is still lacking, mainly those that consider the COSMIN risk of bias tool.8,9
Error of measurement values are important to assist clinical decision-making and interpreting studies’ findings.30 In this review, 10 studies20–26,29 analyzed the SEM or MDC of PPTs, and most of them20–26 presented very good methodological quality. However, they did not define the MIC, which is required to rate the results according to the COSMIN quality criteria.
Four studies assessed the validity of the upper extremity PPTs, one19 with doubtful, one with adequate,18 and two22,24 with very good methodological qualities. However, due to the low number of studies and small sample sizes, the QoE, in general, was low19,22,24 or moderate.18 The Arm-Jump Board Test in rock-climbing19 presented strong correlations with data from a 3D accelerometer (velocity, time, index of efficiency, and relative and absolute powers), but there was a lack of information about the measurement properties of the 3D accelerometer. Furthermore, the studies that investigated the concurrent validity of the CKCUEST and Unilateral Seated Shot-Put Test observed moderate to strong correlations of those tests with isokinetic strength of shoulder IR and ER.24 The construct validity of the Shoulder Endurance Test was previously investigated22 and showed weak correlations with isometric strength of shoulder IR and ER.
Tarara et al.,4 conducted a systematic review with 11 included studies that investigated the measurement properties of 6 PPTs. They also used the Terwee Scale, COSMIN checklist, and modified GRADE approach. For comparison, our systematic review included 15 studies that assessed 13 PPTs, 6 of which were also included in that previous systematic review.4 Furthermore, COSMIN checklist was updated in 2018 and 2020,10,31 so the newest version was applied. Therefore, the results of this review provide an updated and detailed information about the measurement properties on PPTs.
Strength and limitationThis systematic review was conducted and reported following PRISMA guidelines.7 The comprehensive search strategy, careful evaluation of the methodological quality according to the COSMIN,8,9 and grading the level of evidence12–14 provided updated information on measurement properties of the upper extremity PPTs. This study summarized and graded the level of evidence of the reliability, standard error, and validity of PPTs, which can assist clinicians in choosing a PPT according to the characteristics of the population, results of reliability and validity, and interpretation according to SEM and MDC, following an evidence-based approach. However, care should be taken because the QoE for most of the tests was very low, inconsistent, or with no evidence, and there is a lack of information about the responsiveness of all upper extremity PPTs.
Seventy percent of the sample were men, which may limit the generalizability of the findings, and more studies are needed to verify the measurement properties of PTTs in women. This systematic review focused on investigating measurement properties of the PPTs, so technology-dependent instruments, including hand-held dynamometer, isokinetic dynamometer, and 2/3-dimentional motion analysis, were not within the scope of this review. However, those instruments are important in the assessment of upper extremity and their measurement properties should be summarized by future reviews.
Implications for researchFurther investigation on the inter-session and inter-rater reliability, measurement error, validity, and responsiveness of the upper extremity PPTs are still needed for enhancing the level of evidence. Using the COSMIN recommendations for planning, conducting, and reporting measurement properties studies will enhance the methodological quality of future studies.
The stability of clinical factors that could influence the scores obtained in the assessments, using scales or questionnaires (e.g., Visual Analogue Scale,32 Global Rating of Change [−3 to +3]32), and if the test-retest assessments were performed under similar conditions (e.g., familiarization with the test, same environment, and instructions) are important details that enhance the methodological quality of a reliability study. Also, it is recommended to report if the rater was blinded to the values obtained in the first assessment session; using appropriate time interval (i.e., 7 to 14 days) between the test-retest measurements to assure that patients were stable between the assessments and avoid recall bias. Additionally, it is recommended to randomize the limb or tests order, blinding athletes to the results until the second session is completed and including at least a sample size of 50 athletes to investigate measurement properties.
SEM and MDC values are important to the clinical decision-making, but there is a lack of these measurements for many PPTs, as well as information regarding the responsiveness and MICs of upper extremity PPTs, ideally using an anchor‐based longitudinal approach (e.g. global rating of change) and longitudinal study designs.
Also, research is needed to investigate the validity against gold standard measurements or at least instruments with adequate measurement properties as a comparison. As an example, it seems important to assess the correlation of the Shoulder Endurance Test with shoulder horizontal abductors and extensors muscle strength or IR, ER, horizontal abductors, and extensors resistance using an isokinetic dynamometer.
Implications for practicePPTs are frequently used in clinical practice to assess athletes' performance, rehabilitation progress, predict the risk of new injuries, and guide prevention and rehabilitation programs.2,5 The results of the present review indicate that the CKCUEST and Seated Single-Arm/Unilateral Seated Shot-Put Test are reproducible to be used in clinical practice. The Seated Medicine Ball Throw is a valid test to be used to evaluate upper body power. The other tests mentioned in this review should be used with caution because the measurement properties were not sufficient to support clinical practice.
ConclusionThis systematic review identified that the CKCUEST presented sufficient inter-session and intra-session reliability, based on moderate and high-quality of evidence, respectively. The Seated Single-Arm Shot-Put Test also presented sufficient inter-session reliability, based on moderate quality of evidence. The CKCUEST, Unilateral Seated Shot-Put Test, and Repetition to Failure Assessment Test demonstrated a low level of evidence of sufficient validity and the Seated Medicine Ball Throw presented moderate quality of evidence of insufficient validity.
FundingThis study did not receive financial support.



