




Increased foot pronation during walking has been associated with low back pain. This association may be due to the impact of increased pronation on pelvic motion.
ObjectiveTo investigate the effects of increased bilateral foot pronation on pelvic kinematic in frontal and transverse planes during the loading response phase of gait.
MethodsPelvic, hip, and foot angular positions of 20 participants were collected while they walked at fast speed wearing flat and medially inclined insoles inserted in the shoes. Pelvic motion in frontal and transverse planes was analyzed during the loading response phase. Foot eversion-inversion was analyzed during the complete stance phase to verify the insoles effectiveness in inducing increased pronation and to exclude excessive pronators.
ResultsInclined insoles were effective in inducing increased foot pronation. Pelvic and hip motion were altered in the increased pronation condition compared to the control condition. In the frontal plane, mean pelvic position was more inclined to the contralateral side (mean difference [MD]: 0.54°; 95%CI: 0.23, 0.86) and its range of motion (ROM) was reduced (MD: 0.50°; 95%CI: 0.20, 0.79). In the transverse plane, mean pelvic position was less rotated toward the contralateral leg (MD: 1.03°; 95%CI: 0.65, 1.60) without changes in ROM (MD: 0.04°; 95%CI: -0.17, 0.25). The hip was more internally rotated (MD: 1.37°; 95%CI: 0.76, 1.98) without changes in ROM (MD: 0.10°; 95%CI: -1.02, 1.23).
ConclusionIncreased bilateral foot pronation changes pelvic motion during walking and should be assessed, as a contributing factor to possible pelvic and lower back disorders.
Increased foot pronation during walking has been associated with low back pain,1 which is a common condition.2 This association might be due to the influence of increased foot pronation on pelvic motion during gait.3 Arguably, adequate pelvic motion in the frontal and transverse planes is required to guarantee optimal impact absorption by tissues around the hip joint,4 which would prevent transfer of excessive stresses to more proximal structures typically implicated in low back symptoms (e.g. sacroiliac and spinal joints). During gait, the greatest demand for impact absorption occurs during the loading response phase.5 However, the effects of bilateral increased pronation on pelvic motion during this particular gait phase have not been described.
Increased pelvic range of motion (ROM) in the frontal plane may increase stresses to pelvic and spinal joints during the gait loading response phase. Increased foot pronation dynamically shortens the lower limb, which may relate to pelvic drop.3 Additionally, the magnitude of pelvic drop is associated with the magnitude of lumbar lateral flexion during gait.6 It is, therefore, reasonable to believe that increased foot pronation might increase pelvic drop during the loading response phase and may increase stress on tissues around the lower back.
Increased bilateral foot pronation may also influence pelvic movement in the transverse plane during the gait loading response phase. Typically, during this phase, pelvic rotation is coupled with hip internal rotation of the reference limb and hip external rotation of the contralateral lower limb.7,8 Increased foot pronation increases hip internal rotation8; therefore, increased bilateral foot pronation during the loading response phase of the reference limb might increase hip internal rotation to both limbs and consequently alter pelvic rotation. For example, it is reasonable to speculate that during the right foot loading response phase, increased left foot pronation is expected to promote left hip internal rotation, which increases passive tension of hip soft tissues and may limit anterior pelvic rotation (leftward). Because hip internal rotation would have already started, the available range of this movement during anterior pelvic rotation would be reduced, and the maximum left hip internal rotation could be reached, limiting pelvic full rotation in this phase. Pelvic rotation typically contributes to increases in step length observed in faster walking speeds (>3km/h),9 while minimizing pelvic torsional stresses. Therefore, a reduced range of pelvic rotation due to increased foot pronation may increase torsional stresses to pelvic joints and help explain the relationship between increased foot pronation and low back symptoms.1,10
This study investigated the effects of induced bilateral foot pronation on pelvic kinematics in the frontal and transverse planes during the loading response phase of gait. In addition, considering the close relationship between foot, hip, and pelvis kinematics, we also reported the effects of foot pronation on hip kinematics in the transverse plane.
MethodsParticipantsThe sample size was calculated based on a pilot study with 10 participants which considered the differences of the pelvic mean position between the two conditions in both planes. This calculation indicated a minimum sample size of 19 participants, considering the power as 80% and alpha 0.05. Twenty-six healthy young adults (18 females and 8 males) volunteered to participate in this study. The inclusion criteria were (i) no history of pain or injury in the lower limbs and lumbo-pelvic region for the last 12 months; (ii) no history of surgery in the lower limbs, pelvis, or trunk, (iii) shank-forefoot alignment <24°, which is an indication of varus foot alignment beyond the normal range,11 (iv) ankle dorsiflexion and eversion ROM >13° 12 and >10°,13 respectively, and (v) hip internal rotation ROM >23°,14 because limited ROM at these joints could prevent the induced foot pronation effects on pelvic kinematics. Participants’ ROM and alignment measurements were collected by the same examiner using a goniometer. The exclusion criterion was the presence of excessive foot pronation during gait, which was defined as mean rearfoot eversion angle during the stance phase of gait >6.7°.11 All participants signed an informed consent and this study was approved by the Ethical Research Committee of the Universidade Federal de Minas Gerais (CAAE: 169.0.203.000-11). No participant complained of pain or discomfort during data collection.
Experimental designParticipants walked on a flat electric treadmill ProAction G635 Explorer (BH Fitness – Vitoria-Gasteiz, Spain) wearing a pair of Crusader 4 (Mizuno Inc® – Vietnam) neutral shoes of appropriate size. The walking speed was set at 5 km/h (i.e. 1.39 m/s). This choice was based on the fact that faster walking speeds increase pelvic ROM.15
There were two conditions defined by the shoe insole type used bilaterally. For the control condition, participants wore a pair of shoes with flat insoles. For the experimental condition, they used a pair of shoes with 15° medially inclined insoles designed to induce increased foot pronation bilaterally. The 15° inclination was applied throughout the insole length. Both insoles were made of high-density Ethylene Vinyl Acetate (EVA) in 10 different sizes to fit the available walking shoes.
ProceduresInitially, an interview and physical assessment were conducted to evaluate volunteers’ eligibility to participate in the study. Then, data were recorded during gait at 100Hz using a three-dimensional motion analysis system (Codamotion®, Charnwood Dynamics Ltd., Rothley, England) with three CODA units, containing three infrared sensors each.
A single examiner identified anatomical landmarks and created virtual markers with a pointer integrated with the motion analysis system.16,17 For the pelvis, the proximal landmarks were the top of the iliac crests, and distal landmarks the greater trochanters. Landmarks were used as reference position to create local coordinate systems for the rearfoot, shank, thigh, and pelvis. Cluster with three tracking markers each were used on these segments to minimize soft tissue artifacts18 (Fig. 1A). The shoes had a posterior opening to allow rearfoot cluster attachment directly to the calcaneus (Fig. 1B). Technical markers were placed on the shoe area corresponding to the calcaneus and forefoot to define gait events19 (Fig. 1C).
 Clusters of tracking markers mounted on the lower limb and pelvis; b) Rearfoot cluster placement and shoe adaptation; c) Technical markers indicated by red arrows.")
A static standing trial was recorded with the participants wearing shoes with flat insoles bilaterally. To compute the rearfoot position, time-series used to exclude excessive pronators, the subtalar neutral position was used as the reference (0°) position. For that, a second static trial was recorded. Participants remained on the treadmill with the same shoes, insoles, and clusters. The same examiner placed the foot in the subtalar neutral position defined as the foot position in which the talus’ head is equally palpated along its medial and lateral borders at its articulation with the navicular.20 Participants maintained upright stance, holding the foot in the subtalar neutral position for 5 seconds, while position data were registered.
After the static trials, data from tracking and technical markers were registered while participants walked on the treadmill for 30 gait cycles in each condition. An examiner carefully changed the insoles between the two conditions to assure that it did not affect the rearfoot cluster position. Prior to data collection at each condition, participants practiced walking until they felt comfortable with the walking shoe and insoles. The order of test conditions was randomized.
Data reductionGlobal coordinate system (XYZ) was determined according to the treadmill position: X-axis was defined as anterior-posterior, Y-axis as medial-lateral, and Z-axis as superior-inferior.21 Local coordinate system was also created for each segment with the same axis and directions. Rearfoot, shank, thigh, and pelvis kinematic signals were processed using Visual 3D Motion Analysis software (C-Motion, Inc., Rockville, USA). Position data from each marker were filtered with Butterworth, fourth-order, zero-lag, low-pass filter with a cut-off frequency of 6Hz.22
The following kinematic variables were calculated: a) rearfoot eversion-inversion relative to the shank (around X-axes); b) pelvic movement in the transverse plane (around Z-axes) relative to the laboratory; c) pelvic movement in the frontal plane (around X-axes) relative to the laboratory; and d) thigh rotation relative to the pelvis (around Z-axes). All kinematic data were calculated based on the Cardan sequence Y-X-Z.23 Rearfoot eversion, one of the pronation components, was used as an index of foot pronation.24
The average eversion-inversion position of the right rearfoot throughout the 30 gait stance phases was computed to ensure that the medially inclined insoles increased foot pronation with respect to the control condition, and to exclude individuals presenting excessive foot pronation. To assess the increased foot pronation effect on pelvic motion, the mean ROM and the average pelvic position in the transverse and frontal planes during the 30 loading response phases of the right lower limb were calculated.
Three gait events were identified using the technical markers (Fig. 1C) to identify two phases of gait: (a) the entire stance phase of gait - used for analyses of the exclusion criterion related to excessive foot pronation; (b) the loading response phase - used for analyses of the effect of foot pronation on pelvic motion and hip rotation. The events were: initial contact (determined based on a marker located on the lateral aspect of the calcaneus), forefoot contact and toe off (both determined based on the marker located on the fifth metatarsal head).19 Stance phase of gait was defined from initial contact to toe off, whereas the loading response phase of gait from initial contact to forefoot contact.19
ReliabilityA pilot study with 10 participants was conducted to investigate the reliability of measures and procedures of this study. Data were collected in two different sessions, separated by one week. The intra-examiner reliability (ICC) of the rearfoot position relative to the shank while the subtalar was maintained in neutral position was 0.81. Intra- and inter-examiner reliabilities (ICC) for gait events determination varied from 0.97 to 0.99. Coefficients of multiple correlation (CMC) were used to calculate inter-test reliability of time-series and varied from 0.80 to 0.85. All measures and procedures indicated good to excellent reliability.25,26
Statistical analysisStatistical analyzes were performed using IBM SPSS Statistics software for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). Data were normally distributed, according to Shapiro-Wilk's test. Paired t-tests were used to compare the two insole conditions with respect to: average rearfoot position during gait stance phase; ROM and average position of pelvis in frontal and transverse planes and of hip in transverse plane during the loading response phase of gait (α= 0.05). The mean difference (MD) between conditions and 95% confidence interval (CI) were also calculated.
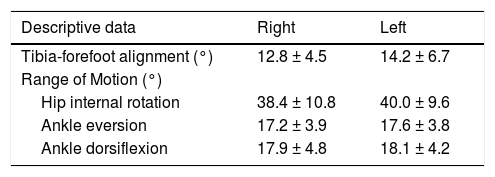
ResultsParticipantsSix participants presented excessive foot pronation and were excluded from the study. Results are based on 20 adults (15 females and 5 males) with average age, mass, and height of 23.7 ± 3.4 years, 64.2 ± 12.1 kg and 1.68 ± 0.06 m, respectively. Descriptive data of the participants are presented in Table 1.
Descriptive data of the participants (n=20).
Data are presented as mean ± standard deviation.
The average rearfoot position during the stance phase was significantly different between insole conditions. Wearing the inclined insole increased mean rearfoot eversion by 6.20 ± 1.93° (95% CI: 5.82, 6.58). The rearfoot was either less inverted or more everted throughout the entire stance phase (Fig. 2).
Pelvic kinematics during loading response: Frontal plane.")
Fig. 3A illustrates mean pelvic movement in the frontal plane during the reference leg stance phase. Paired t-test indicated that inclined insoles increased contralateral pelvic drop during the loading response phase (MD: 0.54°; 95% CI: 0.23, 0.86). Also, the ROM significantly reduced in the increased pronation condition, compared to the control condition (MD: 0.50°; 95% CI: 0.20, 0.79). Results are illustrated in Fig. 3B and3C, respectively.
 Pelvic movement in frontal plane during stance phase of gait (mean curve defined over the 30 gait cycles of all participants). The gray highlighted area refers to the loading response of the reference leg; b) Average position of the pelvis in the frontal plane during the loading response phase of gait performed under the control (CC) and increased pronation (IPC) conditions. More negative values suggest greater magnitudes of contralateral drop; c) Mean pelvic range of motion in the frontal plane during the loading response phase of gait performed under control (CC) and increased pronation (IPC) conditions.")
Effects of increased pronation on pelvic motion in the frontal plane; a) Pelvic movement in frontal plane during stance phase of gait (mean curve defined over the 30 gait cycles of all participants). The gray highlighted area refers to the loading response of the reference leg; b) Average position of the pelvis in the frontal plane during the loading response phase of gait performed under the control (CC) and increased pronation (IPC) conditions. More negative values suggest greater magnitudes of contralateral drop; c) Mean pelvic range of motion in the frontal plane during the loading response phase of gait performed under control (CC) and increased pronation (IPC) conditions.
Fig. 4A illustrates mean pelvic movement in the transverse plane during the reference leg stance phase. The pelvic average position in the transverse plane was less rotated to the left (towards the contralateral limb) when pronation was induced, compared to the control condition (MD: 1.03°; 95% CI: 0.65, 1.60). The ROM was not significantly different between conditions (MD: 0.04°; 95% CI: -0.17, 0.25). Results are illustrated in Fig. 4B and4C, respectively.
 Pelvic movement in transverse plane during stance phase of gait (mean curve defined over the 30 gait cycles of all participants). The gray highlighted area refers to the loading response of the reference leg; b) Mean pelvic position in transverse plane during loading response phase of gait performed under control (CC) and increased pronation (IPC) conditions; c) Mean pelvic range of motion in the transverse plane during loading response phase of gait performed under control (CC) and increased pronation (IPC) conditions.")
Effects of increased pronation on pelvic motion in the transverse plane; a) Pelvic movement in transverse plane during stance phase of gait (mean curve defined over the 30 gait cycles of all participants). The gray highlighted area refers to the loading response of the reference leg; b) Mean pelvic position in transverse plane during loading response phase of gait performed under control (CC) and increased pronation (IPC) conditions; c) Mean pelvic range of motion in the transverse plane during loading response phase of gait performed under control (CC) and increased pronation (IPC) conditions.
The hip average position in the transverse plane was more internally rotated when increased pronation was induced, compared to the control condition (MD: 1.37°; 95% CI: 0.76, 1.98). Hip ROM was not significantly different between conditions (MD: 0.10°; 95% CI: -1.02,1.23).
DiscussionThis study showed that increased bilateral foot pronation increased hip internal rotation, increased pelvic contralateral drop, reduced pelvic ROM in the frontal plane, and reduced pelvic rotation toward the contralateral side during the loading response phase of gait. These findings reveal a potential mechanism underlying the relationship between increased foot pronation and pelvic motion that could contribute to the development of pelvic and lower back musculoskeletal conditions.
Increased pronation caused greater pelvic contralateral drop during the loading response phase. Pinto et al.,27 in contrast, demonstrated that bilateral pronation induction did not change pelvic posture in the frontal plane during standing position. They revealed that unilateral foot pronation caused ipsilateral pelvic drop, suggesting pronation shortened the lower limb and consequently led to functional leg length discrepancy, increasing pelvic drop toward the more pronated side. The foot pronation effects on functional leg length may also explain the increased contralateral drop demonstrated by the present study. During the loading response phase, while the reference foot is pronating, the contralateral foot, which is in the push-off phase, is supinating, which attenuates pelvic contralateral drop through increase in functional leg length.3 Therefore, inducing foot pronation to the contralateral side, dynamically shortens the contralateral limb and consequently increases pelvic contralateral drop. However, Resende et al.3 found a similar result when pronation was induced unilaterally. Thus, leg length discrepancy is not the only explanation for this finding.
The foot pronation effects on hip rotation and hip abductors lever arm may also explain the increased pelvic contralateral drop. This mechanical coupling between foot and hip motion was also demonstrated elsewhere.8 Increased foot pronation leads to increased hip internal rotation, which, by moving the greater trochanter medially, may reduce the gluteus medius and minimus lever arm. Thus, the reduced capacity of these muscles to generate torque may explain the greater pelvic contralateral drop (hip adduction). Following this hypothesis, we might also expect increased contralateral drop during single-leg stance, considering hip internal rotation is greater. This result, however, was not reported by Resende et al.3 The loading response phase is when impact absorption mainly occurs and when hip abductors activity is mostly required during walking to control hip adduction and contralateral pelvic drop.5 Therefore, a reduction in the hip abductors lever arms may be sufficient to hamper torque generation, resulting in the observed increased contralateral pelvic drop in the increased pronation condition. However, during single-leg stance, when less impact is expected, hip abductors might be less required compared to the loading response phase and, even with greater reduction in abductors lever arm, they may be capable of avoiding pelvic drop.
Increased bilateral foot pronation reduced pelvic ROM in the frontal plane, which may affect muscular work. Work may be represented by the product of muscular torque and ROM.28 Therefore, reduced pelvic ROM may reduce hip abductors eccentric work and, consequently, decrease load absorption during the loading response phase. As seen in Fig. 3A, reduced pelvic ROM in the frontal plane was consequent to the reduced pelvic ipsilateral drop at initial contact during the increased pronation condition. This reduction in pelvic drop, in turn, can be explained by the fact that the contralateral (left) foot is in the push-off phase (expected to be supinated) and pronation induction to this foot may be more representative, causing left limb dynamic shortening, as discussed above. Because the pelvis is in a more dropped position at the beginning of the stance phase, its ROM until the end of the loading response phase was reduced.
Fig. 4A shows that in both conditions the pelvis remained rotated to the left, but less so when bilateral increased pronation was induced. Different hip movement between test conditions may explain this result. As shown in this study, foot pronation leads to hip internal rotation. The hip ROM is expected to be increased to the contralateral hip, as the reference leg moves forward during walking and the pelvis rotates to the left.29 Therefore, left hip internal rotation is expected to be greater during the right foot loading response when pronation is increased. While we did not measure left hip motion, this pattern of coupling between foot and hip motions was documented previously8 and, in our study, foot pronation was increased at push-off phase during increased pronation condition (Fig. 2). Thus, it is a reasonable assumption that increase in left hip internal rotation occurred during loading response of the right limb when excessive pronation was induced. Because hip internal rotation increases passive tension of hip external rotators, it may limit pelvic rotation leftwards. This helps explain the reduced pelvic rotation towards the contralateral side found in this study. Conversely, increased pronation did not change pelvic ROM.
The present study was the first to analyze pelvic rotation in the transverse and frontal planes with bilateral pronation induction during walking. It revealed short-term effects during gait loading response phase. More studies are required to explore whether such effects are present in long-term excessive pronators individuals. It is possible that tissue and neuromuscular adaptations - such as reduction in hip external rotators stiffness due to greater hip internal rotation ranges,30 and hypermobility of foot first ray31 due to push-off in pronated position - might modify such effects. Regardless, knowing the effects of increased bilateral pronation itself will help rationalize possible changes in pelvic motion in long-term excessive pronators.
It is important to note that, although the mean differences between conditions were small, they represent modifications of approximately 52% and 9% of the total pelvic ROM in the transverse and frontal planes during the loading response phase, respectively. These changes in pelvic rotation might be relevant. Müller et al.32 found that individuals with low back pain had pelvic rotation toward the contralateral limb reduced in <35% in the early gait stance phase, compared to asymptomatic people. Thus, it is possible that this small change of 1.03°, in a total range of 1.99°, could be potentially harmful. Instead, the observed changes in pelvic position in the frontal plane may not lead to low back pain unless associated with other contributing factors such as decreased hip abductors activity5 and leg length discrepancy.27 Jiménez-del-Barrio et al.33 found that individuals with low back pain increased pelvic drop by 55% (2.02°) in average, compared to asymptomatic individuals during gait stance phase. Thus, the 0.54° increase in the contralateral pelvic drop was found to represent about 16% of the difference between symptomatic and asymptomatic individuals reported by Jiménez-del-Barrio et al.33 Although this small difference could not lead to low back pain by itself, it still may contribute to the occurrence of low back or pelvic dysfunctions. This study's findings revealed a potential mechanism underlying the relationship between increased foot pronation and pelvic motion, especially in the transverse plane, during walking that clinicians should consider when examining patients with pelvic and low back disorders.
The walking speed chosen in this study (5km/h) was the same for all participants; however, their body height range was small and so the relative effort was similar between them. Additionally, this walking speed is considered normal for this age group.34 It is also important to note that pelvic motion was tracked with external markers, which may include errors due to skin movement artifacts. The mean differences observed may be within the margin of measurement errors.35 Notably, we employed procedures to minimize measurement errors. We used clusters of tracking markers, which reduce soft tissue artifacts.18 Clusters were not replaced nor repositioned throughout data collection. We restricted our analysis only to the gait loading response phase, in which the hip ROM is not large.29 Additionally, the conditions’ order was randomized and data collection happened on the same day, during a short period, and the only modification made by the examiners was in the type of insoles, which were carefully changed so it didn't affect the clusters’ position. Finally, the tested reliability of our system and protocol to capture pelvic motions has been shown to be high (0.80-0.85). Thus, we expect the errors to be smaller than those reported in the literature35 and, consequently, the reported changes in pelvic motion associated with foot pronation to be reliable albeit of small magnitude.
The present study findings suggest that increased bilateral pronation could alter spinal and sacroiliac joints stresses. The observed inclined pelvic position (Fig. 3B) may favor asymmetric joint loads and stresses especially at the low back joints.6 Asymmetric spinal loading has been implicated on degenerative processes leading to low back pain.36 Furthermore, changes observed in the transverse plane indicate that the pelvis contributes less to step length, which may favor greater hip sagittal motion and then greater torsional loads at pelvic joints.37 Therefore, increased foot pronation could be potentially related to the development of pelvic and low back stresses, especially if associated with other relevant factors.
ConclusionsBilateral increases in foot pronation led to small but significant changes in pelvic motion. Induced bilateral foot pronation increased mean contralateral pelvic drop and reduced the pelvic ROM in the frontal plane during the loading response phase of gait. Additionally, increased foot pronation reduced pelvic rotation towards the contralateral side. These findings show that foot pronation may be a contributing factor for altering pelvic motion and should be considered, associated with other clinically relevant factors, when assessing pelvic motions during walking for individuals with pelvic and lower back disorders.
Conflicts of interestNone to declare.
This research was supported by the Brazilian Funding Agencies CAPES, CNPQ and FAPEMIG.



