


High intensity interval training (HIIT) has been used as a cardiovascular exercise strategy to promote greater adherence in cardiovascular rehabilitation. However, little is known about the effect of this training modality on cardiac autonomic control.
ObjectiveTo perform a systematic review to evaluate the effects of HIIT on cardiac autonomic responses in humans.
MethodsPEDro, SCOPUS and PubMed were searched from the inception to March 29th, 2018. Moreover, the methodological quality and statistical reporting from all eligible clinical trials were assessed by the PEDro scale. The articles were eligible if: The primary objective was related to the effects of HIIT on the cardiac autonomic nervous system. Outcomes evaluated were indirect measures of cardiac autonomic control, represented by HRV indexes.
ResultsThe search strategies resulted in 339 citations and 2 additional citations were identified through other sources. After deleting the duplicate articles and revising the full text, 6 articles were included. Overall, the results showed an improvement in parasympathetic and/or sympathetic modulation after HIIT, when evaluated by linear and non-linear indexes of HRV.
ConclusionsHIIT is a promising tool to improve the cardiac autonomic control, with more recommendation in healthy individuals and patients with metabolic syndrome.
Various sources of evidence suggest that regularly practicing physical exercise has an inverse relationship with premature mortality and the development of chronic cardiovascular diseases (CVD), as well as preventing major risk factors.1 This relationship occurs due to neurohumoral, vascular and structural changes in the cardiovascular system.1 Neural adaptations to aerobic physical exercise, such as decreased cardiac sympathetic and increased parasympathetic modulation in rest, are important cardioprotective factors as sympathetic hyperactivity is an integral part of the pathophysiology of various cardiac diseases.2–4
Therefore, the evaluation of autonomic control by indirect measures, such as heart rate variability (HRV), has been applied to clinical practice to provide information on cardiac regulation, as well as to evaluate neural adaptations to physical exercise.5–8 HRV can be evaluated by linear methods, which quantify the sympatho-vagal balance or non-linear methods, which consider the complexity of the interaction of biological systems on the heart.7–9 Reduction in resting HRV is a sensitive indicator of cardiac autonomic impairment and is associated with a higher risk of CVD morbidity and mortality. This condition occurs due to the predominance of sympathetic modulation, consequently, enhancing the cardiac overload and/or reduction of cardiac parasympathetic modulation. Therefore, interventions to increase HRV, that is, increment of parasympathetic modulation at rest, should be investigated.10
Although regular physical exercise is a factor in increasing HRV, few patients are referred to and engaged into a physical training program.11 Low adherence is often associated with exercise intolerance caused by the pathological condition, in addition to the lack of time.12 In view of this situation, high intensity interval training (HIIT) may be a cardiovascular exercise strategy to promote greater adherence in cardiovascular rehabilitation as it covers shorter training sessions (20–25min), comprising high intensity exercise intervals (85% to 95% of maximum HR and/or maximum oxygen consumption) interspersed with rest or active recovery, allowing patients to have complete periods at high intensity.13,14 Moreover, the periods of high intensity stimulate more intense cardiovascular and muscular adaptations in cardiopathy patients, which favors mitochondrial function and calcium reabsorption rate into the sarcoplasmic reticulum, reducing skeletal muscle fatigue and increasing exercise capacity.15
Although some studies demonstrate better effects of HIIT, when compared to continuous moderate intensity training, on the aerobic capacity of patients with CVD, little is known about the effect of this training modality on cardiac autonomic control.15,16 Thus, the purpose of this study was to conduct a systematic review to evaluate the effects of HIIT on cardiac autonomic responses in humans, evaluated by HRV, allowing the training application in the rehabilitation and prevention of pathologies that have autonomic imbalance as clinical characteristics.
MethodsThis systematic review was reported following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).17 Moreover, the State of the Art through Systematic Review (StArt)18 was used to help and systematize the search and data extraction (available from: http://lapes.dc.ufscar.br/tools/start_tool).
Data sources and search strategyElectronic databases from inception to March 29th, 2018 were searched including: PEDro (Physiotherapy Evidence Database), SCOPUS (Elsevier) and PubMed (via National Library of Medicine). The following MeSH terms were used for the intervention type (“high intensity interval training”) and outcomes (“autonomic nervous system” OR “heart rate”). Furthermore, the search was limited to humans (population of interest) and the English language. Finally, the additional limits were used: clinical study, clinical trial, controlled clinical trial and randomized clinical trial.
Study criteria and selectionThe eligibility criteria were determined using the Patient/Population–Intervention–Comparison/Comparator–Outcome (PICO) format. The selected studies had looked at: Adults with or without cardiovascular disease (P); who carried out a HIIT program (I); there were no comparisons with other interventions (C); our results of interest were measurements of cardiac autonomic control through HRV (O). Review articles, non-randomized clinical trials, short communications, letters with insufficient information to analyze the results, case studies, guidelines, theses, dissertations, qualitative studies, scientific conference abstracts, studies on animals, acute interventions, non-English language articles and articles addressing other exercises type (continuous aerobic training and resistance training) as primary intervention, were excluded.
Two authors (PRS and RMA) initially selected the articles by screening titles and abstracts, independently, according to the study criteria. Full-text screening was performed when considered potentially eligible by the two reviewers. If there were some disagreements between these reviewers, a third independent reviewer (RPS) was consulted to determine inclusion in the systematic review. In addition, when articles were not available, the authors were contacted and references of articles selected were verified to search for other relevant studies.
Data extractionFrom each selected study, data were reported through descriptive analysis and complementary the deltas of HRV indexes (post minus pre) were calculated. Moreover, the data were extracted by two independent reviewers (PRS and RMA), using standardized forms that included information about characteristics of participants and groups (population, sample size, groups, gender, age, peak oxygen consumption [VO2PEAK] and body mass index [BMI] at baseline); characteristics of intervention (ergometer, high intensity interval, recovery interval, number and duration of sessions, intervention time, supervised intervention); measurements and main outcomes related to the effects of HIIT on HRV indexes. In addition, the secondary variables and other functional gains (blood pressure, functional capacity, corporal composition, cardiovascular function, cardiorespiratory fitness and metabolic changes) found in each study were also extracted.
Heart rate variability analysisThe comparison of interest were indexes of HRV assessment by linear methods (frequency and time domains), also non-linear methods (e.g., SampEn, Poincaré method and detrended fluctuation analysis) which are described below.
Linear methodsThe frequency domain to quantify the short-term HRV provides two main frequency components: high frequency (HF), that represents an index of parasympathetic modulation and low frequency (LF), that when expressed in normalized units correspond to cardiac sympathetic modulation.8 However, some authors consider the LF, if expressed in absolute values, as a component that has sympathetic and parasympathetic influences19 while others showed that this component does not have cardiac sympathetic influence but reflects baroreceptor reflex activity.20,21
In addition, the LF/HF ratio is applied as an indicator of “sympatho-vagal balance,” where possibly an increase is related to sympathetic predominance and a decrease indicates greater parasympathetic modulation.22 However, there is still questionable the interpretation of LF/HF, since the LF band does not correspond purely to sympathetic modulation, also the interpretation of this ratio depends on the environmental conditions and collection time (short or long term).23 In addition, the interactions of the autonomic nervous system pathways have a complex and non-linear dynamic, making controversial the “sympatho-vagal balance” theory.24
Moreover, components of very low frequency (VLF) and ultra-low frequency (ULF) are less used because, although there are some hypotheses, their physiological mechanisms are still being investigated. Furthermore, the analyses of ULF requires a recording period of at least 24h and it seems to be related to very slow-acting biological processes, like metabolism, the renin-angiotensin-aldosterone system and thermoregulation.8,19,20,25 While, the VLF ideally requires a long-term recording period (over 24h) and appears to be related to heart's intrinsic nervous system and its oscillations is influenced by sympathetic nervous system.8,26
Another linear approach, the time domain method identified the intervals between successive beats and carried out the numerical analyses such as: standard deviation of the RR interval (SDNN) and standard deviation of the means of the normal RR intervals, every 5min (SDANN) that represents the conjoint sympathetic and parasympathetic modulation8; square root of the mean squared differences of successive RR intervals (RMSSD) and the percentage of adjacent RR intervals with a duration difference greater than 50ms (pNN50) and both indicate cardiac parasympathetic modulation.10 Finally, triangular interpolation of RR intervals (TINN) express the global variability with joint action of the autonomic nervous system pathways.27
Non-linear methodsComplementarily, the non-linear methods such as: SampEn, Poincaré method and detrended fluctuation analysis (DFA), consider the complex dynamic of biological systems on RR interval series. The values of SampEn approaching 0 are considered highly regular and larger values mean greater complexity.28 The Poincaré method consists of constructed plots from the RR interval data for each participant and these plots display each RR interval as a function of the subsequent RR interval in that time-series. This analysis can visually search for patterns buried within a time series.29 Moreover, these plots can derive two main non-linear measurements, SD1 and SD2.
The SD1 represents the dispersion of points perpendicular to the identity line and measures of short-term HRV in ms. It characterizes cardiac parasympathetic modulation30,31 and it correlates with baroreflex sensitivity,32 while SD2 represents the dispersion of points along the identity line and indicates the short and long-term HRV in ms (jointly cardiac sympathetic and parasympathetic modulation and correlates with LF power and baroreflex sensitivity).32 Finally, the slope α1 of DFA analysis, consists of brief fluctuations, while the slope α2 describes long-term fluctuations. The slope α1 reflect the baroreflex sensitivity, while the long-term reflects the mechanisms that limit oscillations of the beat cycle.8,33
Quality assessmentThe methodological quality of individual studies was assessed using the Physiotherapy Evidence Database (PEDro) scale34 and two researchers classified the articles independently (PRS and RMA). When there was any disagreement, the researchers discussed it to obtain a consensus between them concerning the final score. Articles were classified into two levels: high quality (score: ≥6) and low quality (score: <6).35 The PEDro scale included 11 questions related to methodological quality and statistical reporting: eligibility criteria were specified; subjects were randomly allocated to groups; allocation was concealed; the groups were similar at baseline regarding the most important prognostic indicators; there was blinding of all subjects; there was blinding of all therapists who administered the therapy; there was blinding of all assessors who measured at least one key outcome; measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups; all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat”; the results of between-group statistical comparisons are reported for at least one key outcome; the study provides both point measures and measures of variability for at least one key outcome. However, the maximum final score was 10 points because it did not include question 1 (specifying the origin of the subject and eligibility criteria) as it affects the external validity rather than internal validity.36 Moreover, for interpretation and discussion of the results, the impact of methodological quality was considered according to the PEDro scale total score.
ResultsStudy selectionThe search strategies in the electronic databases resulted in 339 citations and 2 additional citations were identified through other sources. After deleting duplicate articles and revising the full text, 6 articles were included. The main reasons for excluding the articles were: (a) assessment of acute effects37–40; (b) other measurements of cardiac autonomic control and not by HRV41–43; (c) non-randomized clinical trials44–47 (Fig. 1).
Quality assessment
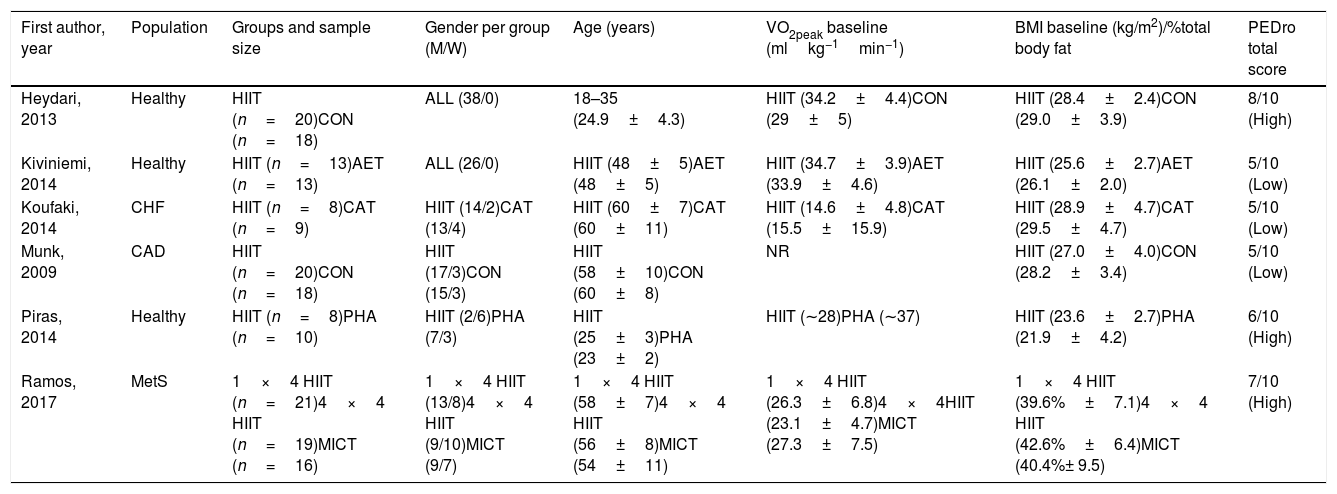
The methodological quality of the included studies is described in Table 1. The mean score of PEDro was 6 (ranging from 5 to 8), with 3 studies of high quality48–50 and 3 studies of low quality.51–53 Commonly, the items not performed or omissions in reporting information were: blinding of all subjects (6 studies), all therapists who administered the therapy (5 studies) and all assessors who measured at least one key outcome (5 studies) and the allocation was not concealed (4 studies).
Study and participants characteristics.
| First author, year | Population | Groups and sample size | Gender per group (M/W) | Age (years) | VO2peak baseline (mlkg−1min−1) | BMI baseline (kg/m2)/%total body fat | PEDro total score |
|---|---|---|---|---|---|---|---|
| Heydari, 2013 | Healthy | HIIT (n=20)CON (n=18) | ALL (38/0) | 18–35 (24.9±4.3) | HIIT (34.2±4.4)CON (29±5) | HIIT (28.4±2.4)CON (29.0±3.9) | 8/10 (High) |
| Kiviniemi, 2014 | Healthy | HIIT (n=13)AET (n=13) | ALL (26/0) | HIIT (48±5)AET (48±5) | HIIT (34.7±3.9)AET (33.9±4.6) | HIIT (25.6±2.7)AET (26.1±2.0) | 5/10 (Low) |
| Koufaki, 2014 | CHF | HIIT (n=8)CAT (n=9) | HIIT (14/2)CAT (13/4) | HIIT (60±7)CAT (60±11) | HIIT (14.6±4.8)CAT (15.5±15.9) | HIIT (28.9±4.7)CAT (29.5±4.7) | 5/10 (Low) |
| Munk, 2009 | CAD | HIIT (n=20)CON (n=18) | HIIT (17/3)CON (15/3) | HIIT (58±10)CON (60±8) | NR | HIIT (27.0±4.0)CON (28.2±3.4) | 5/10 (Low) |
| Piras, 2014 | Healthy | HIIT (n=8)PHA (n=10) | HIIT (2/6)PHA (7/3) | HIIT (25±3)PHA (23±2) | HIIT (∼28)PHA (∼37) | HIIT (23.6±2.7)PHA (21.9±4.2) | 6/10 (High) |
| Ramos, 2017 | MetS | 1×4 HIIT (n=21)4×4 HIIT (n=19)MICT (n=16) | 1×4 HIIT (13/8)4×4 HIIT (9/10)MICT (9/7) | 1×4 HIIT (58±7)4×4 HIIT (56±8)MICT (54±11) | 1×4 HIIT (26.3±6.8)4×4HIIT (23.1±4.7)MICT (27.3±7.5) | 1×4 HIIT (39.6%±7.1)4×4 HIIT (42.6%±6.4)MICT (40.4%± 9.5) | 7/10 (High) |
AET, aerobic endurance training; BMI, body mass index; CAD, coronary artery disease; CAT, continuous moderate intensity aerobic exercise; CON, control group; CHF, chronic heart failure; HIIT, high-intensity interval training; M, men; MetS, metabolic syndrome; MICT, moderate-intensity continuous training; NR, not report; PHA, peripheral heart action training; VO2peak, peak oxygen consumption; W, women; For age, VO2peak, and BMI at baseline, data are expressed as mean and standard deviation.
The characteristics of participants and groups are described in Table 1. The total sample size was 193 individuals aged from 18 to 60 years old, with the BMI at baseline from 21.9 to 29.5kg/m2. Five articles reported the peak oxygen consumption (VO2peak) ranging from 14.6 to 37mlkg−1min−1, while one study did not report this measurement.21 Regarding the groups, there was a range from 8 to 21 individuals per group, and two studies presented a control group,48,53 three compared the HIIT with aerobic training of moderate intensity49,51,52 and one with peripheral heart action training.50 Three articles included a healthy population in their samples,48,50,51 while the other studies evaluated the effects of HIIT in patients with coronary artery disease (CAD),53 chronic heart failure52 and metabolic syndrome (MetS).49
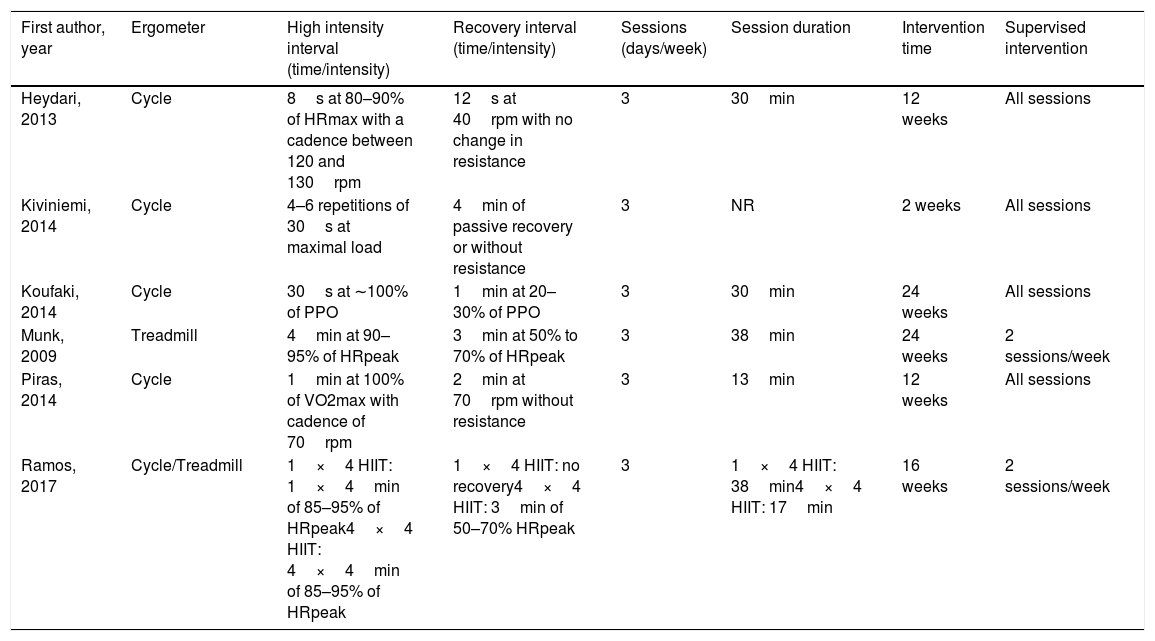
Characteristics of interventionsThe characteristics of HIIT interventions are summarized in Table 2. Most studies used the cycle ergometer to perform the training sessions while one also used the treadmill according to preference and physical limitation of the participants49 and one study trained the participants only on the treadmill.53 The time of the high intensity interval ranged from 8s to 4min, with intensity between 80% and 100% prescribed by the HRpeak, VO2max/peak or peak power output (PPO) reached in the incremental test. The cadence of the high intensity interval in cycle was maintained from 70 to 130rpm, while four studies did not report this information.49,51–53 Regarding recovery interval periods, the time ranged from 12s to 4min of active recovery without resistance. Moreover, most frequently, the training was performed three training sessions per week of 13–38min per session and all were supervised in at least two of them. Furthermore, the mean of the duration of HIIT was 14 weeks, varying from 2 to 24 weeks.
Characteristics of HIIT interventions.
| First author, year | Ergometer | High intensity interval (time/intensity) | Recovery interval (time/intensity) | Sessions (days/week) | Session duration | Intervention time | Supervised intervention |
|---|---|---|---|---|---|---|---|
| Heydari, 2013 | Cycle | 8s at 80–90% of HRmax with a cadence between 120 and 130rpm | 12s at 40rpm with no change in resistance | 3 | 30min | 12 weeks | All sessions |
| Kiviniemi, 2014 | Cycle | 4–6 repetitions of 30s at maximal load | 4min of passive recovery or without resistance | 3 | NR | 2 weeks | All sessions |
| Koufaki, 2014 | Cycle | 30s at ∼100% of PPO | 1min at 20–30% of PPO | 3 | 30min | 24 weeks | All sessions |
| Munk, 2009 | Treadmill | 4min at 90–95% of HRpeak | 3min at 50% to 70% of HRpeak | 3 | 38min | 24 weeks | 2 sessions/week |
| Piras, 2014 | Cycle | 1min at 100% of VO2max with cadence of 70rpm | 2min at 70rpm without resistance | 3 | 13min | 12 weeks | All sessions |
| Ramos, 2017 | Cycle/Treadmill | 1×4 HIIT: 1×4min of 85–95% of HRpeak4×4 HIIT: 4×4min of 85–95% of HRpeak | 1×4 HIIT: no recovery4×4 HIIT: 3min of 50–70% HRpeak | 3 | 1×4 HIIT: 38min4×4 HIIT: 17min | 16 weeks | 2 sessions/week |
HIIT, high intensity interval training; HRmax, heart rate maximal; HRpeak, heart rate peak; NR, not reported; PPO, peak power output; Rpm, rounds per minute; VO2max, maximal oxygen consumption.
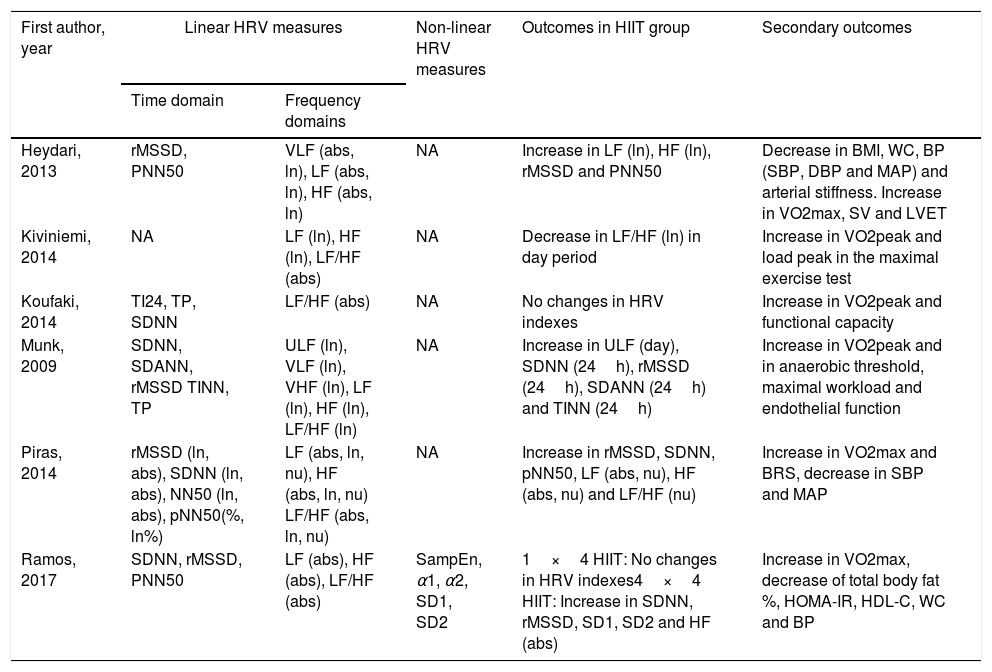
All information about the effects of HIIT on indexes of HRV is described in Table 3. The studies evaluated the cardiac autonomic control by linear and/or non-linear analysis, moreover, the HRV was acquired at rest condition during short (10min) and long-term (30min to 24h) ECG recording.
Effects of HIIT on HRV indexes and secondary outcomes.
| First author, year | Linear HRV measures | Non-linear HRV measures | Outcomes in HIIT group | Secondary outcomes | |
|---|---|---|---|---|---|
| Time domain | Frequency domains | ||||
| Heydari, 2013 | rMSSD, PNN50 | VLF (abs, ln), LF (abs, ln), HF (abs, ln) | NA | Increase in LF (ln), HF (ln), rMSSD and PNN50 | Decrease in BMI, WC, BP (SBP, DBP and MAP) and arterial stiffness. Increase in VO2max, SV and LVET |
| Kiviniemi, 2014 | NA | LF (ln), HF (ln), LF/HF (abs) | NA | Decrease in LF/HF (ln) in day period | Increase in VO2peak and load peak in the maximal exercise test |
| Koufaki, 2014 | TI24, TP, SDNN | LF/HF (abs) | NA | No changes in HRV indexes | Increase in VO2peak and functional capacity |
| Munk, 2009 | SDNN, SDANN, rMSSD TINN, TP | ULF (ln), VLF (ln), VHF (ln), LF (ln), HF (ln), LF/HF (ln) | NA | Increase in ULF (day), SDNN (24h), rMSSD (24h), SDANN (24h) and TINN (24h) | Increase in VO2peak and in anaerobic threshold, maximal workload and endothelial function |
| Piras, 2014 | rMSSD (ln, abs), SDNN (ln, abs), NN50 (ln, abs), pNN50(%, ln%) | LF (abs, ln, nu), HF (abs, ln, nu) LF/HF (abs, ln, nu) | NA | Increase in rMSSD, SDNN, pNN50, LF (abs, nu), HF (abs, nu) and LF/HF (nu) | Increase in VO2max and BRS, decrease in SBP and MAP |
| Ramos, 2017 | SDNN, rMSSD, PNN50 | LF (abs), HF (abs), LF/HF (abs) | SampEn, α1, α2, SD1, SD2 | 1×4 HIIT: No changes in HRV indexes4×4 HIIT: Increase in SDNN, rMSSD, SD1, SD2 and HF (abs) | Increase in VO2max, decrease of total body fat %, HOMA-IR, HDL-C, WC and BP |
X¯RR interval, mean of all RR intervals; α1 and α2, detrended fluctuation analysis; abs, absolute; BMI, body mass index; BP, blood pressure; BRS, baroreflex sensitivity; DBP, diastolic blood pressure; HF, high frequency; HRV, heart rate variability; LVET, left ventricular ejection time; LF, low frequency; ln, logarithm natural; MAP, mean arterial pressure; NA, not assessed; NN50, number of sequential N–N intervals differing by longer than 50ms; nu, normalized units; PNN50, percentage of successive differences between normal adjacent intervals >50ms; rMSSD, square roost of the mean differences between consecutive high-squared RR interval; SampEn, sample entropy; SD1 and SD2, geometric parameter of the Poincaré plot; SDANN, the standard deviation of the average normal RR intervals for 288 5-minute segments of a 24-hour ECG recording; SBP, systolic blood pressure; SDNN, standard deviation of all normal RR interval; SV, stroke volume; TI24, triangular Index of a 24h recording; TINN, the triangular interpolation of NN interval histogram; ULF, ultra low frequency; VHF, very high frequency; VLF, very low frequency; VO2max, maximal oxygen consumption; VO2peak, peak oxygen consumption; WC, waist circumference.
All studies used the frequency domain to quantify the short-term HRV, while five studies also adopted time domain approaches.48–50,52,53 On the other hand, one article49 performed the non-linear analyses including the sample entropy (SampEn), Poincaré method and DFA.
Linear methodsRegarding analysis of time and frequency domain, five studies showed improvements in parasympathetic and/or sympathetic modulation, observed in some HRV indexes. Since in the time domain, an increase of the SDNN (Δ: 5.3–27), PNN50 (Δ: 2.7–4.2), rMSSD (Δ: 0.3–7.1), SDANN (Δ: 27) and TINN (Δ: 108) components was observed.48–50,53 While in the frequency domain, the HFabs (Δ: 44.1–416.13), HFln (Δ: 0.3), LF/HFnu (Δ: 0.13) and ULFln (Δ: 1.1) were increased48,50 and the LF/HFln (Δ: −0.2) was decrease.51 However, the changes in linear indexes were not observed in one study after HIIT.52
Non-linear methodsAmong the nonlinear analysis of HRV, one study with patients with MetS identified an increase in SD1 (Δ: 3.3) and SD2 (Δ: 4.8), when evaluated by the Poincaré method, suggesting an improvement in nonlinear heart rate dynamics.49 Briefly, the results about effects of HIIT on cardiac autonomic modulation of each included article are expressed in Fig. 2 qualitatively.
Secondary outcomes
In addition, others secondary outcomes were observed post HIIT as described in Table 3. All included studies showed improvement of cardiorespiratory fitness, demonstrated by the increase in maximal or peak oxygen consumption (VO2max and VO2peak, respectively), load peak in the maximal exercise test and/or VO2peak at anaerobic threshold. Moreover, the functional capacity assessed by sit-to-stand and gait speed was improved post training.52 Regarding the cardiovascular benefits, were found decrease of blood pressure values,48–50 reduction of arterial stiffness,48 improvement in cardiac48 and endothelial function.53 Finally, other gains such as improvement in body composition,48,49 lipid profile,49 insulin resistance,49 baroreflex sensitivity50 were observed.
DiscussionThis present systematic review, through an evaluation of 6 randomized clinical trials, demonstrated that HIIT can be a training option to improve the cardiac autonomic control in healthy conditions and in patients who have CAD and MetS. The positive effects on HRV observed, were an increase of parasympathetic modulation at rest, represented by the linear indexes, such as: HF, rMSSD, pNN50 and decrease in LF/HF.48–50,53 However, the LF/HF index, presented controversial effects between included studies, Kiviniemi51 observed that this index decreased after the HIIT, representing an increase in vagal modulation; while Piras50 found an increase of LF/HF, indicating a greater sympathetic modulation. On the other hand, when evaluated by non-linear methods, values of DFA did not modify, while increase in SD1 and SD2 indexes of the Poincare analysis were observed reflecting predominance of vagal modulation post training.49
These adaptations represent reductions of cardiovascular risk and overall mortality in cardiovascular rehabilitation, as well as prevention in the development of cardiovascular diseases and their risk factors in healthy individuals.21 Although there is no consensus for the prescription of a HIIT protocol, in general, when performed between 80% and 100% of HRmax, over 20min for 3 days/week can be effective to promote responses on cardiac autonomic control, with effects observed shortly after two weeks.51
Furthermore, several physiological mechanisms support the application of this training in clinical practice. When compared to continuous training, HIIT has a greater ability to stimulate nitric oxide (NO) syntheses by endothelium, due to the shear stress promoted in the vessel wall during high intensity periods.54 The bioavailability of this oxide, promotes stimulus in vagal neurons which are also modulated by endothelial NO.55 Moreover, the HIIT induces a greater degree of distensibility of carotid artery, which is associated with improvements in baroreflex sensitivity.48,56,57 Some studies in this revision attributed these effects by an increase in LF power and its possible relation with baroreceptor reflex sensitivity,48,50,51 although there is still no consensus in the literature about this relationship.19,20,58 In addition, it is well defined that HIIT favors oxidative capacity by improving mitochondrial function, facilitating the diffusion capacity of skeletal muscle.15,59 These mechanisms favor aerobic power (VO2max), which may be correlated to the predominance of rest vagal modulation after HIIT, as demonstrated by one study included.53
In contrast, one study did not identify changes in the indexes of HRV in patients with CHF52 post HIIT. One hypothesis is that these individuals worsened their overall health status during the study and underlying medical conditions, resulting in substantial pauses throughout the experimental protocol.52 Another possible hypothesis to non-changes in HRV indexes post HIIT is that the protocol was performed at a low volume of training. According to some authors, the autonomic control can be improved after high doses of endurance training, equivalent to 75% of HRmax for 200min/wk and is able to restore the indexes of the HRV of elderly sedentary people. On the other hand, low doses of training, performed at 75% HRmax for 95–150min/wk may improve baroreflex sensitivity indexes, but not HRV.60 Although HIIT generally has a lower training volume, the protocol performed by this study52 may not have been enough to promote adaptations in cardiac autonomic function or overlap the effects of medication in these patients.
In general, the quality of the included articles ranged from 5 to 8 points on the PEDro scale. Thus, the evidences that support the beneficial effects of HIIT on the cardiac autonomic control seem to be more reliable in healthy individuals48,50 and in patients with MeTS,49 which presented high methodological quality. Moreover, this systematic review was limited by the heterogeneity of the included studies, in relation to training protocols, populations and methods of analysis. In addition, although individuals with cardiometabolic diseases had their medications monitored and controlled during the trials included in this review,49,53 healthy individuals may have benefited more from HIIT compared to those who administer drugs that may influence the results on HRV.
Finally, despite the promising results of HIIT on cardiac autonomic control demonstrated in this systematic review, it is necessary to carry out future randomized clinical trials that consider the evaluation of the effects of HIIT on the HRV indices, as well as the investigation of the relationship between these analyses. Thus, making it possible to prescribe this method of training, with safety and effectiveness in clinical practice.
ConclusionAlthough this systematic review was limited by different population and protocols of exercise, considering the current evidence, the HIIT is a promising tool to improve the HRV, favoring the increase of parasympathetic modulation at rest, mainly in healthy individuals and patients with MetS, according to the methodological quality and risk of bias of the included studies.
Conflicts of interestThe authors declare that there is no conflict of interest
The authors would like to acknowledge the São Paulo Research Foundation – FAPESP (2017/13402-0) for funding this study.



