
Six-minute walk test (6MWT) is the most used test to assess functional capacity. Including arm span in the prediction equations for 6MWT performance might be an alternative for use in traditional reference equations.
ObjectiveThe aim was to investigate the usability of arm span to predict the 6MWT distance in healthy children.
Methods262 healthy children aged between 6 and 12 years old participated in this study. 6MWT was conducted according to the standardized protocol. Height, weight, and arm span were measured before performing the 6MWT. A multiple stepwise linear regression analysis was used to generate the regression model.
ResultsThe 6MWT distance had strong positive correlations with age, arm span, height, and weight (p<0.001). There was also a very strong correlation between arm span and height (p<0.001). Age and arm span were found as significant predictors in the first regression model. These two variables explained 60.2% of the variance in the 6MWT distance. Age and height were also found as significant predictors, explaining 60.5% of the variance in the 6MWT distance. The two following formula were obtained to predict the 6MWT distance: (−23.09+(31.12×Age)+(2.39×Arm span)) or (−80.0+(28.98×Age)+(2.92×Height)).
ConclusionsThe results suggest that the combination of arm span (or height) and age are strong predictors of the 6MWT distance in healthy children.
A cardiopulmonary exercise test, during which maximum oxygen consumption is measured, is accepted as the gold standard in the measurement of exercise capacity.1 Although considered the most accurate method for measuring exercise capacity, the test requires expensive equipment and specialized staff.2 Because cardiopulmonary exercise test is impractical and unfeasible in clinical settings, several submaximal exercise tests have been developed as an alternative. Among those, the six-minute walk test (6MWT) is the most well-established and used test in clinical settings and research.3 The 6MWT is easier to administer, more acceptable, and provides a better reflection of activities of daily living than other walk tests.4 Additionally, the 6MWT is increasingly used in children.4
A large number of studies have been conducted to determine factors affecting the performance on the 6MWT.4–13 In the majority of these studies, anthropometric measurements were used, and height was shown to be a significant predictor of the 6MWT distance.4–14 However, measurement of height may not give accurate results in some situations, especially due to spinal deformities such as scoliosis and kyphoscoliosis, which are frequently seen in children during developmental stages.15,16 Arm span, instead of height, is used for calculating body mass index in children with spinal deformity.16 In addition, arm span has been shown to be closely associated with pulmonary function parameters and nutritional status in children, adults, and older people.17–19 Because the relationship between height and arm span can vary with age and population, estimating height from arm span can be difficult. Therefore, including arm span in the prediction equations for the 6MWT distance might be a better alternative than indirectly predicting height from arm span for use in traditional reference equations.19 To the best of our knowledge, arm span has not been investigated as a predictor of the 6MWT distance in children. If a prediction equation using arm span was as good as one using height, it could be used to predict the 6MWT distance in children with spinal deformities, in whom height does not give accurate results. Therefore, this study aimed to investigate the potential for arm span to create a prediction equation of the 6MWT distance in healthy children.
MethodsDesign and populationTypically developing children aged 6–12 years were recruited from 4 randomly selected local primary schools for this cross-sectional study. Children who were able to understand and fully comply with the assessments were included in the study. Schools were visited by the researchers, and an invitation letter with a questionnaire to identify health-related problems and demographic characteristics were sent to the parents of eligible children. Parents completed the questionnaire a few days before the testing. Children with known chronic cardiorespiratory, neurological, or musculoskeletal disorders, or who had a common cold within the last four weeks were excluded from the study. A total of 262 eligible children were stratified into seven age subcategories with a one-year interval between 6 and 12 years.
Because there was no study that used arm span as a predictor for the 6MWT, it was not possible to directly calculate a desired a priori sample size. But, it has been shown that the performance on the 6MWT was moderately correlated with spirometric values,5,13 and the prediction equations of spirometric values using arm span were previously reported.19 Therefore, a priori sample size was calculated as 146 for a medium effect size (0.15) and a power of 0.99 using G*Power (Ver. 3.1.9.4, University of Dusseldorf, Germany).20 Due to the indirect calculation, the power was set at a higher threshold. This study included all 262 participants of a previously published study.14
This study was approved by the Ethics Committee of Dokuz Eylül University with the approval number “1060-GOA”. Permission to conduct the study was also obtained from the Turkish National Education Ministry and school authorities. Informed consent was obtained from the parents of the children before participation.
MeasurementsThe participants’ height and weight were determined using standardized anthropometric methods prior to testing on the 6MWT. Arm span was measured by positioning the participants, heels together with the back against a flat wall and the arms stretched sideways with the palms facing the investigator. The distance between the tips of the middle fingers was measured.
The 6MWT was conducted according to the standardized protocol described by the American Thoracic Society guidelines.21 The 6MWT was performed in a flat, straight corridor. Each participant walked along a 30 m tape line, with cones placed at each end of the course. The participants were told to avoid vigorous exercise within 2hours before the test. No “warm-up” period before the test was allowed and the participants sat at rest in a chair, located near the starting position, for at least 10minutes before the test started. The participants were asked to walk for 6minutes at their best pace but not to run or race. Encouragement during the testing was standardized (‘keep going’, ‘you are doing well’) and the announcement of time remaining was given to the participants. No comments were made regarding the participant's performance.
Statistical analysisThe normality of the data distribution was verified using the Kolmogorov-Smirnov test, the skewness and the kurtosis of the sample, and the graphical representation of the distribution. Descriptive statistics were calculated for each age group and all participants. Arm span, height, weight, and 6MWT distance were compared according to sex for each age group and all participants using a t test. Pearson product-moment correlation coefficient was used to examine associations between age, arm span, height, and weight. Correlation coefficients>0.5 were considered as strong, 0.3 to 0.5 as moderate, and 0.2 to 0.3 as weak.22 A multiple stepwise linear regression analysis was used to generate the regression model for 6MWT distance as the dependent variable. The model was used to examine the influence of age, arm span, weight, and height on the 6MWT distance. The effect size, ƒ2 value, was calculated based on the formula, ƒ2=R2/(1−R2). The ƒ2 value was interpreted as small (0.02), moderate (0.15), and large (0.35). All data were analyzed using SPSS for Windows software (Version 23.0. Armonk, NY: IBM Corp.).22
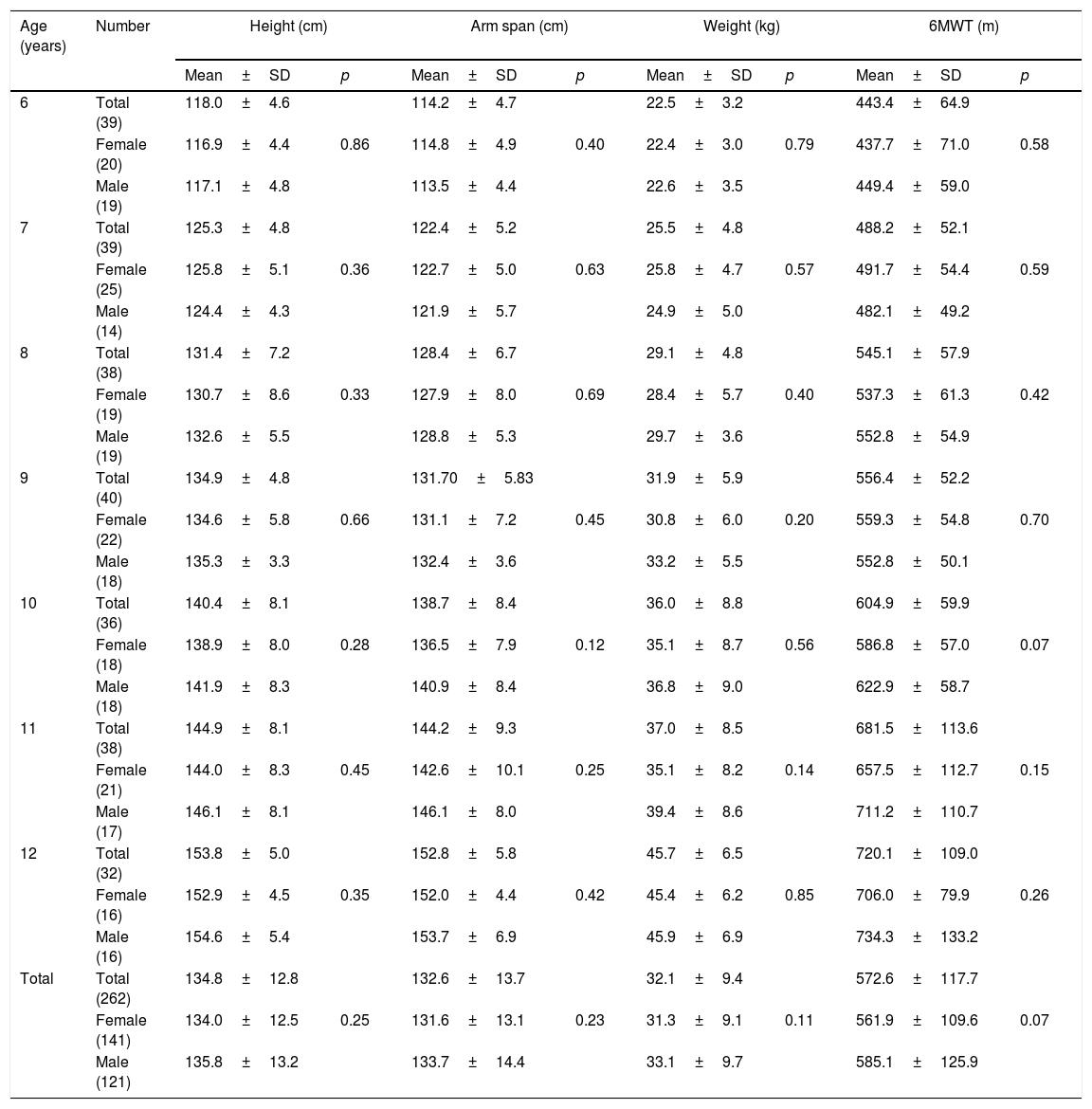
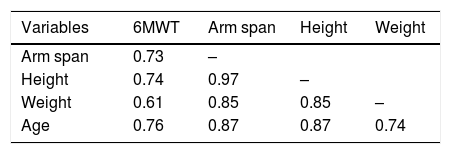
ResultsAll participants completed the entire 6MWT according to the protocol and thus no data were excluded from the analysis. There was no adverse effect during the tests. The characteristics of the participants are presented in Table 1. Arm span, height, weight, and 6MWT distance increased steadily with age. Arm span, height, weight, and 6MWT were not significantly different between sexes for all age groups (p>0.05) (Table 1). The arm span/height ratio was 0.98±0.02 indicating arm span was slightly less than height. As indicated in Table 2, the 6MWT distance had a strong positive correlation with age, arm span, height, and weight (p<0.001). There was also a very strong correlation between arm span and height (p<0.001).
Characteristics of the participants by age group and comparisons between sexes.
| Age (years) | Number | Height (cm) | Arm span (cm) | Weight (kg) | 6MWT (m) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean±SD | p | Mean±SD | p | Mean±SD | p | Mean±SD | p | ||
| 6 | Total (39) | 118.0±4.6 | 114.2±4.7 | 22.5±3.2 | 443.4±64.9 | ||||
| Female (20) | 116.9±4.4 | 0.86 | 114.8±4.9 | 0.40 | 22.4±3.0 | 0.79 | 437.7±71.0 | 0.58 | |
| Male (19) | 117.1±4.8 | 113.5±4.4 | 22.6±3.5 | 449.4±59.0 | |||||
| 7 | Total (39) | 125.3±4.8 | 122.4±5.2 | 25.5±4.8 | 488.2±52.1 | ||||
| Female (25) | 125.8±5.1 | 0.36 | 122.7±5.0 | 0.63 | 25.8±4.7 | 0.57 | 491.7±54.4 | 0.59 | |
| Male (14) | 124.4±4.3 | 121.9±5.7 | 24.9±5.0 | 482.1±49.2 | |||||
| 8 | Total (38) | 131.4±7.2 | 128.4±6.7 | 29.1±4.8 | 545.1±57.9 | ||||
| Female (19) | 130.7±8.6 | 0.33 | 127.9±8.0 | 0.69 | 28.4±5.7 | 0.40 | 537.3±61.3 | 0.42 | |
| Male (19) | 132.6±5.5 | 128.8±5.3 | 29.7±3.6 | 552.8±54.9 | |||||
| 9 | Total (40) | 134.9±4.8 | 131.70±5.83 | 31.9±5.9 | 556.4±52.2 | ||||
| Female (22) | 134.6±5.8 | 0.66 | 131.1±7.2 | 0.45 | 30.8±6.0 | 0.20 | 559.3±54.8 | 0.70 | |
| Male (18) | 135.3±3.3 | 132.4±3.6 | 33.2±5.5 | 552.8±50.1 | |||||
| 10 | Total (36) | 140.4±8.1 | 138.7±8.4 | 36.0±8.8 | 604.9±59.9 | ||||
| Female (18) | 138.9±8.0 | 0.28 | 136.5±7.9 | 0.12 | 35.1±8.7 | 0.56 | 586.8±57.0 | 0.07 | |
| Male (18) | 141.9±8.3 | 140.9±8.4 | 36.8±9.0 | 622.9±58.7 | |||||
| 11 | Total (38) | 144.9±8.1 | 144.2±9.3 | 37.0±8.5 | 681.5±113.6 | ||||
| Female (21) | 144.0±8.3 | 0.45 | 142.6±10.1 | 0.25 | 35.1±8.2 | 0.14 | 657.5±112.7 | 0.15 | |
| Male (17) | 146.1±8.1 | 146.1±8.0 | 39.4±8.6 | 711.2±110.7 | |||||
| 12 | Total (32) | 153.8±5.0 | 152.8±5.8 | 45.7±6.5 | 720.1±109.0 | ||||
| Female (16) | 152.9±4.5 | 0.35 | 152.0±4.4 | 0.42 | 45.4±6.2 | 0.85 | 706.0±79.9 | 0.26 | |
| Male (16) | 154.6±5.4 | 153.7±6.9 | 45.9±6.9 | 734.3±133.2 | |||||
| Total | Total (262) | 134.8±12.8 | 132.6±13.7 | 32.1±9.4 | 572.6±117.7 | ||||
| Female (141) | 134.0±12.5 | 0.25 | 131.6±13.1 | 0.23 | 31.3±9.1 | 0.11 | 561.9±109.6 | 0.07 | |
| Male (121) | 135.8±13.2 | 133.7±14.4 | 33.1±9.7 | 585.1±125.9 | |||||
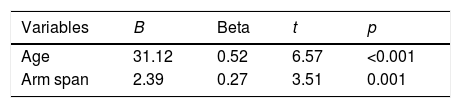
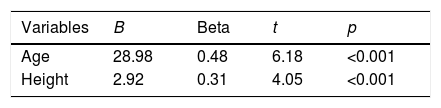
Age (years) and arm span (cm) were found as significant predictors of 6MWT distance (m) in the first regression model. These two variables explained 60.2% of the variance with a large effect size (ƒ2=1.51) (Table 3). Age (years) and height (cm) were also found as significant predictors in a second regression model, explaining 60.5% of the variance in the 6MWT distance, with a large effect size (ƒ2=1.53) (Table 4). The 6MWT distance can be predicted with the formulas; 6MWT distance=−23.09+(31.12×Age)+(2.39×Arm span) or 6MWT distance=−80.0+(28.98×Age)+(2.92×Height).
This study investigated the usability of arm span instead of height to predict the 6MWT distance in healthy children. The results suggest that either height or arm span, when combined with age, explain approximately 60% of the variance in the 6MWT distance.
There are numerous studies reporting a significant correlation between arm span and height in children and adults.23–27 However, in some studies, the agreement between arm span and standing height has been found to be poor.28,29 Despite some inconsistencies, most of the studies reveal a close relationship between height and arm span but do not allow a direct interpretation of the relationship between arm span and 6MWT distance. Unlike standing or sitting height, arm span would be least affected by spinal deformity. Therefore, assessing arm span is a practical and commonly used method to assess “real height” in children with scoliosis or other diseases.30,31 According to the results of our study, height and arm span were both strongly correlated with the 6MWT distance.
The influence of sex, age, anthropometric attributes, geography, environment, ethnicity, lifestyle, and cultural differences on performance on the 6MWT has been investigated in several studies.5–10 The results of previous studies have shown that height, age, and weight were also significantly correlated with the 6MWT distance.5–9 Present guidelines have indicated that the 6MWT distance is influenced by age, sex, height, weight, and motivation.32,33 Our study has revealed for the first time that arm span was also a significant predictor of the results on the 6MWT in healthy children.
Our results indicated that there was no difference in the 6MWT between female and male participants. Therefore, our reference equation can be used for both female and male children. The previous studies support this finding as they also have demonstrated no significant difference in the 6MWT between female and male children.7,8,10,11 A study conducted in the UK demonstrated that age alone explained 41% of the variance in 6MWT performance, and if height and weight were added, 44% of the variation could be explained.7 Another study conducted on Caucasian children showed that in addition to age, reference equations must take height and weight into account.12 In our study, a combination of age and height explained 60.5% of the variance in the 6MWT, which was similar to a combination of age and arm span (60.2%).
In many studies, it has been reported that the arm span was longer than height.28,34–36 However, in this study, consistent with the results of another study conducted on Turkish children, height was slightly more than arm span.37 These results suggest that published prediction equations for the 6MWT, using anthropometric measures, may not be applicable to different ethnicity.
This study has some limitations. First, no patient population was included. Second, although the children were recruited from randomly selected schools located in two cities of Turkey, the selection in each school was conducted by convenience. Last, due to practical and economic limitations, other factors, such as cardiorespiratory fitness, socioeconomic condition, psychosocial status, motivation, level of physical activity, and level of sexual maturation, which are known factors that may influence performance on the 6MWT, were not investigated.38 Therefore, our results may not be representative of all populations and should be interpreted with caution.
ConclusionThe combination of arm span (or height) and age were found to be strong predictors of the 6MWT distance (i.e. the measurement of exercise capacity) in healthy children. The results of the study suggest that arm span, instead of height, may be used for prediction of the 6MWT distance in healthy children.
Conflicts of interestThe author declares no conflicts of interest.
We would like to express our sincere thanks to Turhan Kahraman from the Department of Physical Therapy and Rehabilitation, Faculty of Health Sciences, Izmir Katip Celebi University, Izmir, Turkey for statistical help, and making suggestions for early versions of this manuscript.



