






Ageing reduces muscle strength and function, increasing mortality risk. Identifying simple performance markers can guide interventions for healthy ageing.
ObjectiveTo assess the prospective dose-response association of the 5-repetition Chair Stand Test (5-CST) and handgrip strength (HGS) with mortality in middle-aged and older adults.
MethodsThis prospective study included community-dwelling participants aged 50 years or older from the SHARE study. HGS and 5-CST were assessed at baseline, with all-cause mortality tracked through follow-up interviews. Cox regression with restricted cubic splines was used, controlling for several confounders.
Results43,605 participants (mean age (SD): 65.3 (9.1), 54 % women) were included. During a mean follow-up of 7.3 ± 2.2 years, there were 4154 deaths (9.5 %). Both 5-CST and HGS were curvilinearly associated with all-cause mortality. Using the median level of 5-CST as a reference (11 s), 10th percentile of 5-CST (7 s) showed a hazard ratio (HR) of 0.74 (95 %CI: 0.69, 0.80). The 90th percentile (18 s) of 5-CST showed a HR of 1.18 (95 %CI: 1.14, 1.22). Stratified analysis indicated 5-CST was most strongly associated with mortality in women. Regarding HGS, using the median level as a reference (33 kg), the 10th percentile of muscle strength (21 kg) showed a HR of 1.62 (95 %CI: 1.50, 1.75). The 90th percentile (51 kg) of muscle strength showed a HR of 0.58 (95 %CI: 0.52, 0.64).
ConclusionBoth tools provide valuable information, but HGS may be considered more relevant for identifying those at increased mortality risk, while 5-CST may be especially useful in women.
Aging is associated with physiological and architectural changes in musculoskeletal health,1 including decreased muscle mass and increased intramuscular fat.2 This decline can have a significant impact on daily activities.3 In this regard, rapid population aging is a global phenomenon that poses important public health challenges,4 such as the need to identify markers to predict and prevent mortality risk and guide the design of interventions to promote healthy aging. The implementation of preventive strategies aimed at improving physical health can not only reduce mortality in older adults but also enhance quality of life. Among physical health indicators, low levels of muscle strength and functional capacity are considered important risk factors for morbidity and mortality in this age group.
Handgrip strength (HGS) and the 5-repetition Chair Stand Test (5-CST) are two widely used tests to assess physical health in older people.5,6 HGS is an inexpensive, rapid, simple, and reliable marker of general muscular strength in adults.7–9 Moreover, HGS is widely accepted as an explicator of frailty, cognitive impairment, multimorbidity, and all-cause and disease-specific mortality.10–13 On the other hand, the 5-CST assesses functional capacity, fall risk, and lower-limb strength, providing a more integrated view of mobility and functionality.14–16 Importantly, a major advantage of 5-CST is that it is easy to perform in a variety of settings, including the home, as no other equipment than a timer and a chair is required. Both tests are endorsed by major clinical guidelines and research frameworks, such as the EWGSOP2 consensus,17 as key components in the assessment of sarcopenia, frailty, and functional decline. Their widespread use in epidemiologic studies facilitates international comparisons and benchmarking. In addition, both the HGS and the 5-CST have shown consistent associations with adverse outcomes such as disability, hospitalization, and mortality, making them particularly valuable for public health surveillance and prognostic modeling. Nevertheless, few studies have directly compared the predictive value of both tests within the same cohort, leaving an important gap in understanding their relative utility for mortality risk stratification.
Given their simplicity and applicability in clinical and research settings, the debate over which of these two tests best predicts mortality remains a relevant topic.18,19 Mainly, for the use of HGS as an indicator of global strength, considering the conflicting evidence of association between HGS with lower limb strength (e.g., knee extensor) regardless of age and health status.18 Thus, evaluating the prospective association of HGS and 5-CST with mortality in the elderly may provide a basis for optimizing assessment tools and guiding interventions to prevent functional decline and reduce mortality risk. This study aims to compare the predictive dose-response ability of HGS and 5-CST with respect to mortality in a large, multi-country representative sample of middle-aged and older adults. The value of each test separately in its prognostic value for mortality is expected to be known.
MethodsParticipants and designThis prospective study uses data from the Survey of Health, Ageing and Retirement in Europe (SHARE), covering 27 European countries and Israel.20,21 Among all observations in the dataset (n = 685,919), we included a total of 43,605 community-dwelling individuals aged ≥50 years who had valid measurements of both HGS and 5-CST at wave 5 (baseline, 2013), along with data from at least one follow-up assessment up to December 2022. A detailed flowchart of the selection process is shown in Fig. 1.
 and Five Repetition Chair Stand Test (5-CST).")
SHARE employs a multi-stage stratified sampling design in which participating countries are divided into different strata according to geographical area, and municipalities or postcodes within these strata serve as primary sampling units.20,21 Data are collected in each survey wave through computer-assisted face-to-face interviews in the home. SHARE uses pre-harmonized interviews, and new respondents are enrolled in each wave to compensate for losses. The target population of SHARE is everyone aged 50 and over whose usual place of residence is in one of the countries participating in SHARE. Individuals are excluded from the initial or refreshment sample if they are imprisoned, hospitalized, or out of the country during the entire survey period, if they do not speak the language(s) of the country, or if they have moved to an unknown address. Regardless of their age, partners living in the same household are interviewed.
Chair stand testThe 5-CST was measured once per participant. Participants were instructed to cross their arms over their chest, stand up from a seated position in a chair, and then sit down again, repeating this sequence five times as quickly as possible. A stopwatch was used to measure the time (in seconds) taken to complete five repetitions without using the hands.
Handgrip strengthHGS was assessed using a handgrip dynamometer (Smedley, S Dynamometer, TTM, Tokyo, 0–100 kg). Each hand was measured twice under the guidance of trained interviewers. Participants held their upper arm parallel to the trunk, with the elbow at 90° flexion and the wrist in a neutral position while standing or sitting. Trained interviewers provided standardized instructions to press the dynamometer with maximum effort for 2 s. The value of HGS (unit: kg) was defined as the maximum value of either hand for the present analyses.
MortalityDeath was recorded in end-of-life interviews with proxy respondents, that is, a relative, household member, neighbor, or other person close to the deceased participant, who provided information on date and cause of death. For cause of death, the proxy respondent was asked "What was the main cause of death?" with multiple response options. For this study, we focused on all-cause mortality, which includes deaths from any cause. In the case of a missing value for the date of death, we imputed the mean of the date of the last interview with the participant and the date of the interview with the end-of-life representative. This imputation was applied in 3.3 % of all recorded deaths.
CovariatesThe potential confounders included in the adjustment were: age, sex, body mass index (BMI), smoking status (current smoker, former smoker, never smoker), educational level (classified as low, medium, or high based on ISCED-1997 categories), marital status (divorced or married, living separated from spouse, never married or widowed), geographic region (Eastern, Northern, Southern, Western Europe, and Israel), and number of medications taken.
Statistical analysesCox proportional hazards regression was used to assess the prospective association of 5-CST and HGS, respectively, with all-cause mortality. We used restricted cubic splines with knots at the 10th, 50th, and 90th percentiles of the 5-CST time and HGS kilogram distribution to account for potential nonlinearity. Results were presented as hazard ratios (HR) with 95 % confidence intervals (CI). All analyses were adjusted for age, sex, body mass index, smoking status, educational level, marital status, geographic region, and number of medications taken.
To visualize the association of 5-CST and HGS with the risk of all-cause mortality, we plotted the estimated HRs against the predictors, using the median values as the reference point. In addition, a stratified analysis by sex was performed. All statistical analyses were performed with SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). A p-value of less than 0.05 was considered statistically significant.
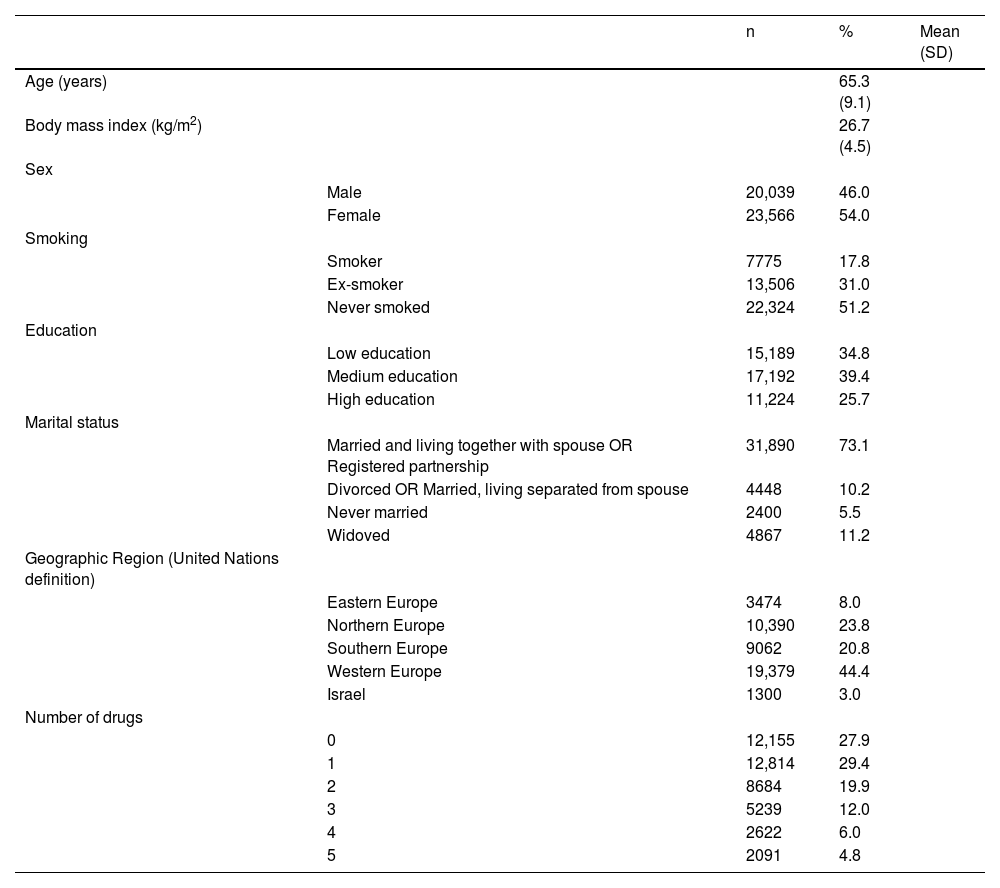
ResultsThe study included 43,605 participants with a mean age of 65.3 years (SD = 9.1). The sample was 54 % female and 46 % male. The mean BMI was 26.7 kg/m² (SD 4.5). The cohort was geographically diverse, with 44.4 % from Western Europe, 23.8 % from Northern Europe, 20.8 % from Southern Europe, 8.0 % from Eastern Europe, and 3.0 % from Israel. The baseline characteristics of the participants are detailed in Table 1. During a mean follow-up of 7.3 ± 2.2 years, a total of 4154 deaths (9.5 %) from all causes were recorded.
Baseline characteristics of participants (n = 43,605).
A curvilinear association between performance on the 5-CST and the risk of all-cause mortality was observed. As illustrated in Fig. 2, using the median 5-CST time (11 s) as the reference point, individuals in the 10th percentile (7 s) had a hazard ratio (HR) of 0.74 (95 % CI: 0.69, 0.80), indicating a protective effect. In contrast, those in the 90th percentile (18 s) had a HR of 1.18 (95 % CI: 1.14, 1.22), reflecting increased risk.
. Note: The solid line shows the hazard ratios and the dashed lines show the 95 % confidence intervals. Model adjusted for age, sex, body mass index, smoking status, educational level, marital status, geographic region, and number of medications taken. Reference value: 11 s.")
Association of 5-repetition Chair Stand Test with risk of death during follow-up in adults older than 50 years (n = 43,605). Note: The solid line shows the hazard ratios and the dashed lines show the 95 % confidence intervals. Model adjusted for age, sex, body mass index, smoking status, educational level, marital status, geographic region, and number of medications taken. Reference value: 11 s.
Sex-stratified analyses revealed differential patterns in the 5-CST–mortality relationship. As shown in Fig. 3, while both men and women demonstrated increased risk with slower performance, the association was more pronounced in women. In men, the relationship plateaued beyond 17 s (90th percentile = 17 s, HR = 1.19, 95 % CI: 1.13, 1.24), whereas in women, the risk continued to rise (90th percentile = 19 s, HR = 1.24, 95 % CI: 1.17, 1.32).

Sex-stratified association of the 5-repetition chair-stand test with risk of death during follow-up. Note: The solid line shows the hazard ratios and the dashed lines show the 95 % confidence intervals. Model adjusted for age, sex, body mass index, smoking status, educational level, marital status, geographic region, and number of medications taken.
Fig. 4 displays the relationship between handgrip strength (HGS) and all-cause mortality, which also followed a curvilinear pattern. Using the median grip strength (33 kg) as the reference, individuals in the 10th percentile (21 kg) exhibited a significantly elevated risk (HR = 1.62, 95 % CI: 1.50, 1.75), while those in the 90th percentile (51 kg) had a lower risk (HR = 0.58, 95 % CI: 0.52, 0.64).
. Note: The solid line shows the hazard ratios and the dashed lines show the 95 % confidence intervals. Model adjusted for age, sex, body mass index, smoking status, educational level, marital status, geographic region, and number of medications taken. Reference value: 33 kg.")
Association of Handgrip Strength with risk of death during follow-up in adults older than 50 years (n = 43,605). Note: The solid line shows the hazard ratios and the dashed lines show the 95 % confidence intervals. Model adjusted for age, sex, body mass index, smoking status, educational level, marital status, geographic region, and number of medications taken. Reference value: 33 kg.
Fig. 5 shows sex-specific analyses of HGS and mortality. In men, the association was steeper, particularly at lower grip strength levels (10th percentile = 32 kg, HR = 1.55, 95 % CI: 1.44, 1.66). In women, the risk increase was slightly less pronounced (10th percentile = 19 kg, HR = 1.42, 95 % CI: 1.31, 1.54).

Sex-stratified association of handgrip strength with risk of death during follow-up. Note: The solid line shows the hazard ratios and the dashed lines show the 95 % confidence intervals. Model adjusted for age, sex, body mass index, smoking status, educational level, marital status, geographic region, and number of medications taken.
Taken together, these results demonstrate that both HGS and 5-CST are independently and non-linearly associated with mortality risk, with sex-specific patterns suggesting their complementary roles in clinical screening. A summary of the results is presented in Fig. 6.

Full multivariable Cox regression models, including hazard ratios and 95 % confidence intervals for both 5-CST and HGS, are presented in Online Material.
DiscussionIn a large sample of middle-aged and older adults from 28 countries, both 5-CST performance and HGS are gradually associated with the risk of all-cause mortality. Although both tests provide valuable information on mortality risk in older people, HGS is a stronger predictor of all-cause mortality than 5-CST, especially in males. In contrast, the sex-stratified analysis suggests that 5-CST may be especially relevant for identifying women over 50 years of age at high mortality risk, as the increased risk was more sensitive to higher test times in this group. This is the first cohort study with long-term follow-up (mean 7 years) to perform a comparative analysis for the association between both markers and mortality.
Mortality risk of 5-CSTOur results indicate that above 10 s for men and 11 s for women there is an increased risk of mortality. Similar thresholds were recently reported as the optimal cut-off values of the 5-CST for assessing sarcopenia in older adults within the Chinese community.22 Furthermore, our observed percentiles are consistent with EWGSOP2 guidelines,17 which define poor physical performance as taking ≥15 s to complete the 5-CST. In our cohort, the 50th percentile was 11 s and the 90th percentile was 18 s, placing a substantial proportion of high-risk individuals above this clinical threshold. From previous studies, little is known about mortality risk behaviors above and below this threshold. As a novel finding, our estimates showed that beyond this point, the slope of mortality risk diverged between sexes as the test time increased, becoming more pronounced in women while stabilizing in men (Fig. 3). This can be explained by few cases among men with slow 5-CST performance, as the confidence interval is quite wide (i.e., increasing the uncertainty).
In addition, sex-related physiological differences may explain this variation, as the mechanisms driving muscle decline and its impact on mortality may differ between men and women. First, the 5-CST, a test designed to assess maximum performance in a short period, is related to functional mobility and muscular power capability (maximum strength generated over a short period of time).23,24 Relative muscle power has been reported to be independently and negatively associated with mortality and hospitalization in older adults25 and is more important than strength to prevent falls and predict mortality in older adults.26 Second, men tend to have higher muscle power even in older ages,27 which may help maintain performance and stabilize mortality risk despite slower times. In contrast, women experience more significant age-related muscle atrophy, particularly in type II fibers (faster fibers),28 since from menopause onwards, they experience greater loss of muscle strength than men due to decreased estrogen, which plays a key role in maintaining muscle mass.29–31 This hormonal deficiency leads to accelerated muscle atrophy and weakness, which affects the speed of execution in the 5-CST and contributes to a steeper rise in mortality risk after the threshold.
Based on our results and these factors, 5-CST seems more recommendable for measuring mortality risk in women than men. These results highlight the practical utility of the 5-CST as a simple, low-cost, equipment-free tool that can be used in community, primary care and physical therapy settings to identify older women at increased risk of mortality. Its feasibility in a wide range of settings makes it a promising screening tool for targeted interventions in populations with limited access to advanced diagnostic resources. Compared to other functional tests such as gait speed or SPPB, the 5-CST mainly reflects the power of the lower limbs. Given its sensitivity in women, the 5-CST could be incorporated into preventive health assessments to help stratify risk and prioritize early mobility-enhancing interventions.
Mortality risk of HGSHigher HGS was associated with lower mortality risk in both men and women, though the patterns differed. These findings are consistent with several studies.11,32–34 Additionally, a previous study examined all-cause mortality in older adults, finding that HGS up to 42 kg for men and 25 kg for women was associated with lower mortality risk, similar to our study (44 kg for men and 27 kg for women).34 Our 10th percentile values (32 kg for men and 19 kg for women) were slightly above the EWGSOP2 thresholds for low grip strength (<27 kg for men, <16 kg for women),17 yet already linked to elevated mortality. This reinforces the prognostic relevance of HGS even before reaching clinical cutoffs. Despite previous studies on mortality risk and HGS by sex, little is known about the specific trends of the risk curves above and below the HR = 1. Interestingly, in our results, the mortality risk for men decreases sharply as HGS increases, then tends to stabilize. In contrast, in women, while the relationship is similar, the decline in mortality risk is more gradual, and at higher levels of HGS, the risk remains closer to 1. Also, this can be explained by the few women with high values and confidence interval becoming wider (i.e., increasing the uncertain estimate).
This suggests that although increasing HGS reduces mortality risk in both sexes, the protective effect is more pronounced in men, while in women, the effect is less noticeable. These sex-related differences can be explained because, generally, men have greater grip strength than women, and the decline in kg with age differs between the sexes, being faster in men than women,35,36 due to the hormonal factors.29–31 In conjunction with previous research,11 our findings justify preventive strategies for older adults with low HGS in both sexes. However, although HGS is a valid indicator of overall muscle strength and correlates significantly with lower limb strength, it may not fully reflect specific deficits. Where possible, complementary tests such as isometric knee extension should be considered whenever possible.
Our results, however, consider that the reduction in mortality risk with increased HGS differs between men and women. Therefore, these differences must be considered when assessing HGS and implementing strategies to improve longevity and quality of life.
5-CST and HGS as modifiers of mortality riskBased on our results, both tools provide valuable information, but HGS is more relevant for identifying those at increased mortality risk in both men and women. Nevertheless, the role of HGS as a modifiable factor after exercise remains controversial.37 A previous meta-analysis showed that resistance training in older adults leads to small but significant improvements in HGS, as reported by various training methods.38 Thus, it is recommended that HGS should not be used to assess overall functional performance after exercise regimens.38 In contrast, other meta-analyses suggest that exercise interventions increase on average HGS by 3–6 kg compared to usual care, where each 1 kg increase in this test is associated with a 9 % reduction in the risk of all-cause mortality in older adults aged >65 years.39,40 The relevance of HGS as a prognostic measure lies in its role as a marker of overall body strength; however, evidence on its association with lower limb strength (e.g., knee extensors) remains conflicting, regardless of age and health status.18,19 In contrast, the 5-CST may provide a more specific assessment of strength in the lower limbs and trunk.41 Low HGS typically indicates general weakness, suggesting a need for overall strength training rather than focusing on isolated muscle groups—except in cases where hand-specific conditions, such as osteoarthritis or rheumatoid arthritis, are present. Another key point is the limited window of opportunity for strength improvement in the HGS compared to the lower limbs, as lower body muscle mass, strength, and power are affected more by aging than are upper body measures.42 On the other hand, 5-CST is a simple test that can also be used to train muscle power and, therefore, as a factor to be considered a modifiable risk.43–47 Moreover, when using both tests, it is crucial to consider the sex-related risk differences and their sensitivity to change after resistance training programs aimed to reduce mortality risk.43,44
Emerging evidence suggests that these measures may not be interchangeable. For example, Verstraeten et al. demonstrated that in geriatric patients hospitalized for rehabilitation, HGS and CST yielded substantially different prevalence estimates of probable sarcopenia, with little concordance, and that only HGS - but not CST - was associated with institutionalization and mortality.48 Our findings are consistent in showing that HGS is more strongly associated with mortality. However, we also observed that CST had prognostic value, especially in women. This suggests that, while HGS may be preferable for general risk stratification, CST may retain value in specific subgroups or when assessing functional impairment. Another advantage of HGS, beyond its association with mortality, is its reliability and clinical utility in detecting muscle weakness even in cognitively impaired older adults.49 Additionally, HGS measured at admission can also predict functional decline in older adults at discharge.50
In clinical practice, these findings support the use of HGS and 5-CST not only as predictors of long-term outcomes, but also as entry points for initiating tailored strength and mobility programs. For example, older adults with low HGS may benefit from global resistance training interventions, whereas those with longer 5-CST times may require more targeted exercises to improve lower extremity strength and balance. These stratified approaches could help physical therapists design efficient, individualized programs with a potential impact on survival and quality of life.
LimitationsThe results of this study should be interpreted with caution, taking into account the following limitations. First, although the model adjusted for several confounding variables, it may not have been sufficient to completely eliminate confounding factors. In addition, some of these variables may change over time, affecting the relationship between testing and mortality. Thus, there is still the possibility of both residual confounding and confounding over time. Second, as the mortality outcome was obtained through a proxy relative, there is still the possibility of some degree of misclassification bias. Third, since the analytical sample only included participants with valid HGS and 5-CST data, it is possible that people with severe physical or cognitive impairments were excluded, which could introduce a selection bias. Fourth, Although the SHARE protocol standardizes administration across countries, specific details on chair type, safety procedures, or discontinuation rates are not available in the dataset. Similarly, the dataset does not include information on the interval between repetitions of HGS measurements. Finally, although our study sample included individuals in an age range associated with higher mortality, it is plausible that the associations of the chair-stand test extend to younger age groups and require further investigation.
An additional consideration is the geographic diversity of the sample, which included participants from Eastern, Northern, Southern and Western Europe, as well as Israel. This broad representation reinforces the external validity of our results. However, regional differences in health systems and socio-economic conditions may influence associations. Although we adjusted our models for geographical regions, some residual confounding cannot be excluded. Future studies could explore these associations within specific regions to better understand local contextual effects. Furthermore, future research should investigate whether changes in 5-CST and HGS can predict mortality trajectories over time. The effectiveness of interventions aimed at improving these markers in high-risk groups, such as older women, should also be evaluated.
ConclusionHandgrip strength is a stronger predictor of all-cause mortality than the 5-CST. However, the 5-CST may also be useful, especially in middle-aged and older women. Both tools provide valuable information, but handgrip strength is more relevant for identifying those at increased mortality risk. Given the simplicity and accessibility of both assessments, their implementation as routine screening tools in physical therapy practice could facilitate early identification of middle-aged and older adults at increased risk of mortality. This would support earlier interventions and better clinical decisions, especially for older adults experiencing functional decline.
The authors declare no competing interests.



