
The six-minute walk test (6MWT) is an important tool for evaluating functional capacity and exercise tolerance. The reference equations for the 6MWT in healthy subjects were established on the basis of American and European populations, but reference equations have been proposed with different variables for the Brazilian population.
ObjectiveTo analyze the predictive validity of six reference equations for the six-minute walking distance (6MWD) in healthy adult men.
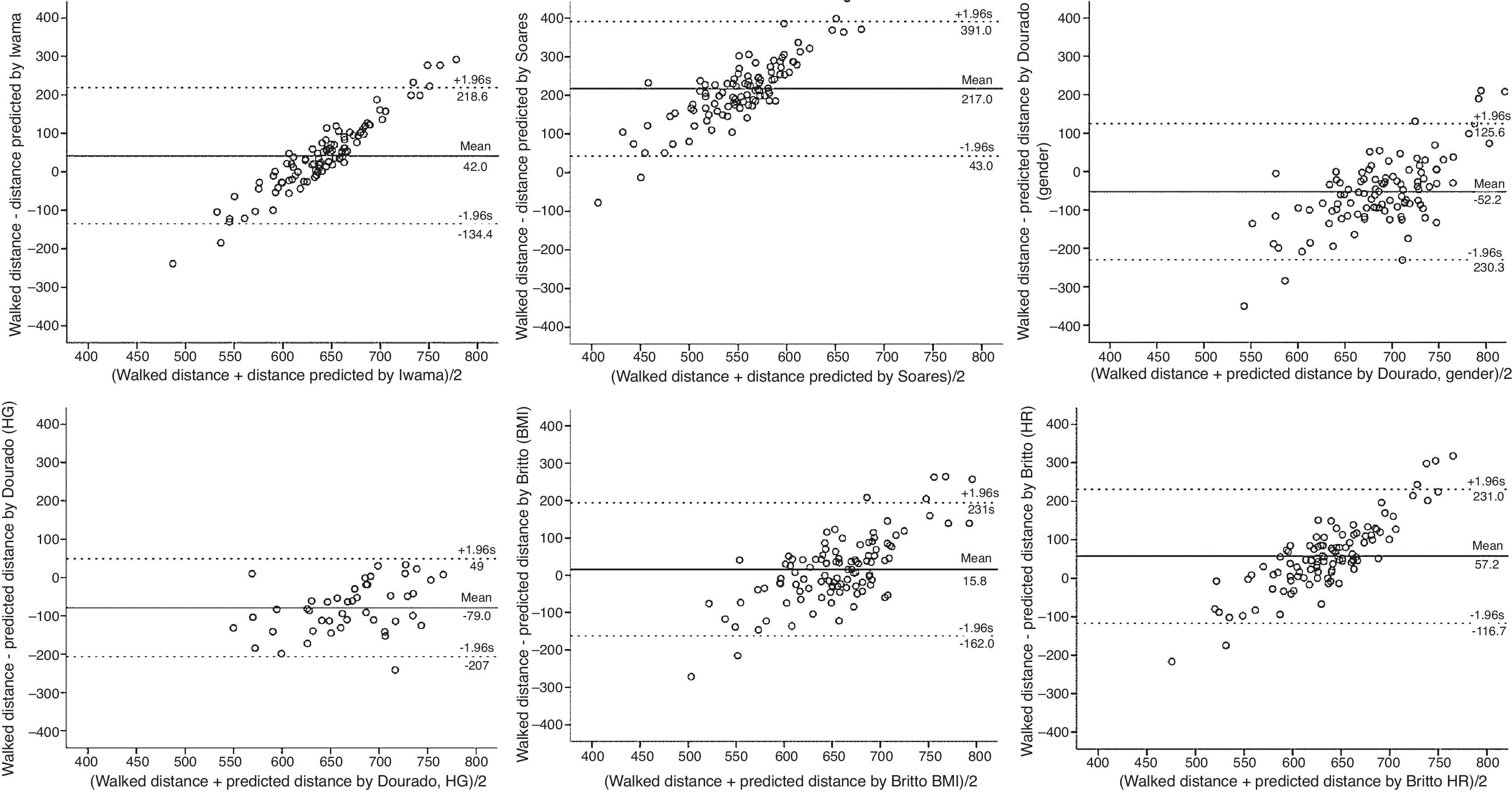
MethodsWe evaluated 103 individuals in relation to level of physical activity (IPAQ), respiratory symptoms (MRC), handgrip strength, and 6MWD test. The data were submitted to a normality test, then the Bland–Altman agreement test was used to compare individual 6MWD values with that expected for each equation.
ResultsThe subjects were active, with a mean age of 34.12 (SD=8.88) years and no respiratory symptoms. The mean of the 6MWD was 663.43 (SD=93.01)m. The 6MWD's predicted values came closest to the walked distance covered by Britto et al.’s equation (using BMI) of 647.62 (SD=38.62)m.
ConclusionsThe equation proposed by Britto et al. using body mass index (BMI) was the closest to the 6MWD for the individuals studied and could be widely used as a reference tool during the 6MWT in healthy Brazilian men.
The six-minute walk test (6MWT) is the test most often used to assess functional exercise capacity, which allows the diagnosis of global exercise response.1 This test is easy, inexpensive, and reliable.2,3 The protocol for the 6MWT recommends that the individual walk as quickly as possible without running for 6min on a flat walkway measuring 30m or 100ft.4–7
The 6MWT is used to classify the individual's functional capacity by means of reference equations, which consider factors such as gender, age, height, weight, and handgrip strength.8–10 Among the many reference equations proposed in the literature,6,11–14 that of Enright and Sherrill15 is the most widely used and internationally cited. Enright and Sherrill proposed their predictive equation for healthy adults after assessing 290 American men and women aged 40–80 years.15
Predictive equations have also been proposed for the Brazilian population. Iwama et al.16 proposed an equation that takes into account anthropometric and demographic factors and tested it on 61 individuals over the age of 13. Soares and Pereira17 developed one predictive equation in healthy individuals of both genders, which included 66 individuals aged 20–80. Dourado et al.18 proposed two different reference equations for the calculation of 6MWD, which included 98 individuals aged 40–60 years, one of them considering handgrip strength test and the other gender. The most recent Brazilian reference equation described by Britto et al.,19 which included 617 healthy individuals from various regions of Brazil, ranging 27–68 years, takes into account demographic and physiological characteristics. The study proposed two equations, the first taking into account gender, age, and body mass index (BMI), and the second considering gender, age, height, and heart rate.19
Although several other predictive equations proposed in the literature have good methodological quality and an adequate sample,6,11–19 none of them compared these predictive equations to determine which might be particularly appropriate for use for the Brazilian population. Although these Brazilian equations have been tested to determine which variables can explain the 6MWT, no study16–19 reported the predictive validity to determine which is closest to the walking distance. We believe it is fundamentally important to identify which one might be the most appropriate to be used in the Brazilian population.16–19
The 6MWT is a simple, fast, inexpensive, and non-invasive test with good clinical applicability and high accuracy for evaluating an individual's functional capacity.2–4 Therefore, the present study aimed to analyze the predictive validity of six equations with reference to a 6MWD proposed for a healthy Brazilian adult population.16–19
MethodsStudy designThis is a cross-sectional study of 103 healthy males aged 18–55, employed in general services, maintenance, operations, and industry, recruited from two universities and a foundry between February and September 2014.20,21
The current study is part of a larger project entitled “Influence of Aging and Work Experience in Physical Performance, Biopsychosocial Aspects, and Motor Workers’ Strategies,” approved in the Public Notice released by the Ministry for Science and Technology (process no. 557752/2009-4) and authorized by the Research Ethics Committee of Universidade Cidade de São Paulo (UNICID), São Paulo, SP, Brazil (protocol 0048.1.186.000-10).
ProcedureThe participants were enrolled from a convenience sample. All individuals were healthy, having no cardiorespiratory, metabolic, neuromuscular, or musculoskeletal diseases, and were able to walk without assistance devices. They received information about the study and agreed to participate by signing the consent form.
First, the weight and height of participants were measured using a scale (Salvapé Produtos Ortopédicos Ltda., São Paulo, SP, Brazil) and a stadiometer (Sanny, American Medical do Brasil Ltda., São Paulo, SP, Brazil) in order to calculate the BMI. Next, the participants answered three questionnaires: a manual-dominance test,22 which preceded the handgrip strength test; the Medical Research Council (MRC) dyspnea scale23; and the International Physical Activity Questionnaire (IPAQ),24 to assess the level of physical activity for tasks performed at home, at work, and at leisure. The participants were categorized as either active for more than 150min (2h and 30min) of moderate-intensity aerobic activity each week or sedentary (less than 150min).24
The handgrip strength test was measured by maximum strength of the hand flexors, using a hydraulic hand dynamometer (SH5001, Saehan Corp., Korea). Forty-five individuals were assessed following the recommendations of the American Society of Hand Therapists (ASHT).25 Each participant was seated comfortably in a chair, with legs at a 90° angle, feet resting on the floor, back straight and supported by the chair, shoulders slightly adducted, elbows flexed to 90°, forearms neutral, without using the chair for support. Each participant was instructed to grip the handle using his maximum strength, without moving the arm or elbow, for a period of up to 5s. A single evaluator standardized the verbal instruction. Three measurements were performed, with rest periods (5min) between them, and the highest measure obtained was used for analysis.22,25
The 6MWT was performed according to the recommendations of the European Respiratory Society/American Thoracic Society.7 All participants received instructions about the test procedures, and each one was told that if he had any discomfort or pain, he would be allowed to rest for as long as necessary. Two tests were performed, with an interval of about 1 hour between them, in order not to mask the effect of learning.7 Before and after each 6MWT, blood pressure, heart rate, oxygen saturation, dyspnea sensation, and limb fatigue (by the Borg Scale26) were measured. Delta heart rate (ΔHR) represented the difference between final and initial heart rate obtained in the 6MWT.
The 6MWT was performed on a flat surface 30m in length. Each meter was marked, and cones were positioned at the beginning and at of the end of the path. Each participant was instructed to walk, not run, as fast as he could for 6min. At the end of each minute, he received a verbal incentive (“You’re doing great, keep it up”) and was informed of the time remaining until the end of the test. The examiner notified the participant 30s before the end of the test, giving a clear command to indicate the end of the test (“Stop”). At that time, the examiner marked the point at which the participant had come to a stop.8
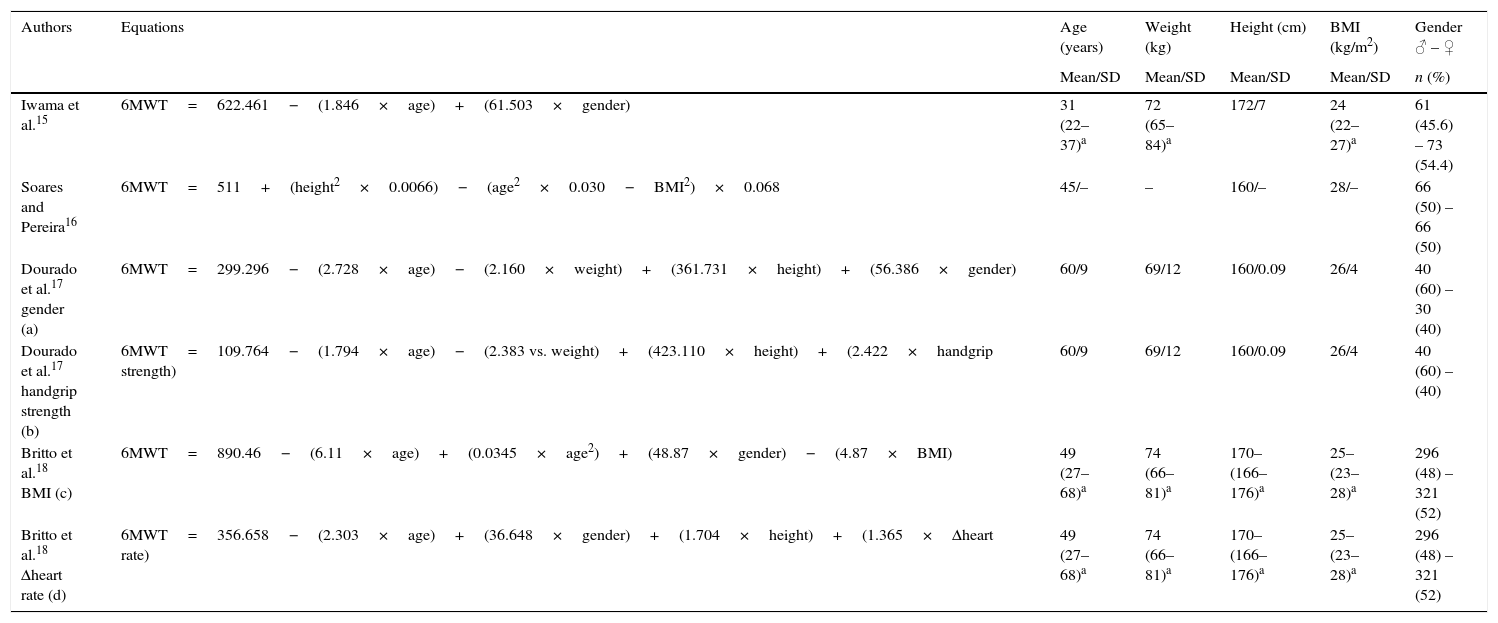
All six reference equations used to predict distance walked and their respective sociodemographic data are presented in Table 1.
Description of Brazilian references equations used and sample characteristics of each equations.
| Authors | Equations | Age (years) | Weight (kg) | Height (cm) | BMI (kg/m2) | Gender ♂ – ♀ |
|---|---|---|---|---|---|---|
| Mean/SD | Mean/SD | Mean/SD | Mean/SD | n (%) | ||
| Iwama et al.15 | 6MWT=622.461−(1.846×age)+(61.503×gender) | 31 (22–37)a | 72 (65–84)a | 172/7 | 24 (22–27)a | 61 (45.6) – 73 (54.4) |
| Soares and Pereira16 | 6MWT=511+(height2×0.0066)−(age2×0.030−BMI2)×0.068 | 45/– | – | 160/– | 28/– | 66 (50) – 66 (50) |
| Dourado et al.17 gender (a) | 6MWT=299.296−(2.728×age)−(2.160×weight)+(361.731×height)+(56.386×gender) | 60/9 | 69/12 | 160/0.09 | 26/4 | 40 (60) – 30 (40) |
| Dourado et al.17 handgrip strength (b) | 6MWT=109.764−(1.794×age)−(2.383 vs. weight)+(423.110×height)+(2.422×handgrip strength) | 60/9 | 69/12 | 160/0.09 | 26/4 | 40 (60) – (40) |
| Britto et al.18 BMI (c) | 6MWT=890.46−(6.11×age)+(0.0345×age2)+(48.87×gender)−(4.87×BMI) | 49 (27–68)a | 74 (66–81)a | 170– (166–176)a | 25– (23–28)a | 296 (48) – 321 (52) |
| Britto et al.18 Δheart rate (d) | 6MWT=356.658−(2.303×age)+(36.648×gender)+(1.704×height)+(1.365×Δheart rate) | 49 (27–68)a | 74 (66–81)a | 170– (166–176)a | 25– (23–28)a | 296 (48) – 321 (52) |
Unit of measurement: × (times); height (cm); age (years); weight (kg); handgrip strength (kgf); BMI (kg/m2); Δheart rate (bpm); ♂, male; ♀, female.
The data are expressed as median (interquartile range 25–75%).
–, values not disclosed by the authors; for all equations, male gender=1 and female gender=0. (a) Dourado et al.17 equation by gender; (b) Dourado et al.17 equation by handgrip strength; (c) Britto et al.18 equation by BMI; (d) Britto et al.18 equation by Δheart rate.
The data from all 103 participants were tested for normality using the Kolmogorov–Smirnov test. The sample size (n=100) to test criterion validity (predictive validity) reflects the gold standard (6MWD) as recommended by COSMIN.27,28 Then, the distances predicted by each reference equation were compared with distance walked (6MWD) by each participant. The Bland–Altman agreement analysis (B&A plot) was used to obtain the agreement interval (95%) to estimate the bias (measurement error) of each of the six reference equations with walked distance in the 6MWT.29,30 The level of significance was set at p<0.05. The software package SPSS 23.0 was used for statistical analysis.
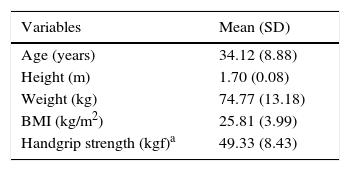
ResultsThe mean age of the 103 subjects was 34.12 (SD=8.88) years, with a range of 18–55 years. Thirty-six subjects were between 18 and 29 years of age, 43 subjects were between 30 and 39, 70 subjects were between 40 and 49, and seven subjects were between 50 and 55. Mean height was 1.70 (SD=0.08)m, where the minimum height was 1.51m and the maximum height was 1.91m. Mean BMI was 25.81 (SD=3.99)kg/m2, where the minimum weight was 51.6kg and the maximum weight was 104kg; 2 were underweight, 41 had normal weight, 49 were overweight, and 11 were obese. The self-reported physical activity level identified 93 (90.2%) individuals as active. All individuals recruited to participate in the study completed the 6MWT with no interruption. The handgrip strength test was performed by 45 participants, and the mean score was 49.33 (SD=8.43)kgf (Table 2).
Descriptive characteristics of the study population (n=103).
| Variables | Mean (SD) |
|---|---|
| Age (years) | 34.12 (8.88) |
| Height (m) | 1.70 (0.08) |
| Weight (kg) | 74.77 (13.18) |
| BMI (kg/m2) | 25.81 (3.99) |
| Handgrip strength (kgf)a | 49.33 (8.43) |
SD, standard deviation; BMI, body mass index.
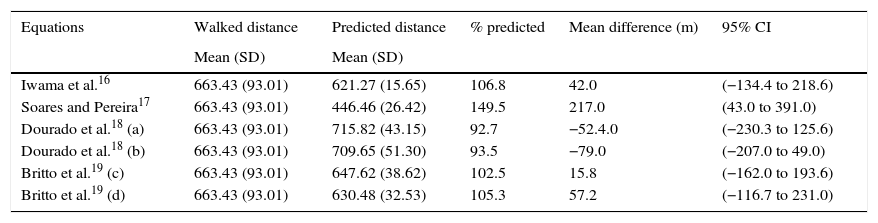
The predictive validity of each reference equation to represent the real distance walked is shown in Table 3. The mean distance walked by the 103 participants was 663.43 (SD=93.01)m.
Agreement between walked distances and predicted values by six reference equations during the 6MWT in healthy adult men (n=103).
| Equations | Walked distance | Predicted distance | % predicted | Mean difference (m) | 95% CI |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | ||||
| Iwama et al.16 | 663.43 (93.01) | 621.27 (15.65) | 106.8 | 42.0 | (−134.4 to 218.6) |
| Soares and Pereira17 | 663.43 (93.01) | 446.46 (26.42) | 149.5 | 217.0 | (43.0 to 391.0) |
| Dourado et al.18 (a) | 663.43 (93.01) | 715.82 (43.15) | 92.7 | −52.4.0 | (−230.3 to 125.6) |
| Dourado et al.18 (b) | 663.43 (93.01) | 709.65 (51.30) | 93.5 | −79.0 | (−207.0 to 49.0) |
| Britto et al.19 (c) | 663.43 (93.01) | 647.62 (38.62) | 102.5 | 15.8 | (−162.0 to 193.6) |
| Britto et al.19 (d) | 663.43 (93.01) | 630.48 (32.53) | 105.3 | 57.2 | (−116.7 to 231.0) |
The distances predicted by the six equations were as follows: (1) Iwama et al.,16 621.27 (SD=15.65)m; (2) Soares and Pereira,17 446.46 (SD=26.42)m; (3) Dourado et al.18 by gender, 715.82 (SD=43.15)m; (4) Dourado et al.18 by handgrip strength, 709.65 (SD=51.30)m; (5) Britto et al.,19 647.62 (SD=38.62)m using age, gender, and BMI; and (6) Britto et al.,19 630.48 (SD=32.53)m using age, gender, height, and heart rate.
The equation proposed by Britto et al.19 using age, gender, and BMI (647.62 [SD=38.62]m) was the closest to the 6MWD (663.43 [SD=93.01]m), confirmed by the Bland–Altman agreement test. The Bland–Altman plots for all six predictive equations are shown in Fig. 1.
Discussion
The result of the comparisons showed that the Brazilian equation proposed by Britto et al.,19 using age, gender, and BMI, came closest to mean distance walked by the participants in the present study. The study participants were active, healthy, and between 18 and 55 years of age, similar to the participants in the studies using the six equations tested.16–19 On average, the participants in the present study were overweight. Their weight seems to have contributed to the closeness of the results of the 6-minute walk test and those predicted by the equations of Britto et al.19 (BMI), which demonstrated a lower mean difference. However, it did not influence the relationship with the other equations, which included BMI, weight, and/or height variables. The equation of Soares and Pereira,17 which also used BMI, underestimated the values of walked distance more than any other equation did. Increased weight can be related to decreased distance in an obese population.31
The equation of Iwama et al.16 is quite simple, using only age for the 6MWD prediction and excluding other relevant anthropometric data, such as height, weight, and BMI, which most of the studies consider fundamental to changes in locomotion.32 Its simplicity might account for the fact that this equation predicted shorter distances than those walked by the subjects in the present study.
The equation of Soares and Pereira17 did not differentiate by gender, instead using a combined variable for both. It could be inferred that differences in physical characteristics between genders might affect the results; thus, a general equation for both genders might be expected to return predicted distances that were much shorter than the walked distance in the present study.
The predicted distance of the equations of Dourado et al.18 overestimated the 6MWD values found in the present study. The equations use anthropometric variables, which might be expected to better represent each individual. One of the two equations included the handgrip strength variable, which may be appropriate because it represents a clinical variable that can establish physical status. The variables age, height, weight, and gender are used as recommended by the American Thoracic Society (ATS) to evaluate functional capacity as variables affecting the 6MWT. We believe that perhaps the use of too many predictive variables may lead to overestimating the distance walked.
The most predictive equation, as determined by the present study, was one of the two proposed by Britto et al.19 for healthy adult Brazilians. The first equation, which used age, gender, and BMI, predicted an average distance of 647.62 (SD=38.62)m. The second equation, which used age, gender, height, and heart rate, predicted an average distance of 630.48 (SD=32.53)m. Thus, the first equation more closely predicted the walked distance, which was 663.43 (SD=93.01)m. This equation was proposed in one of the most recently published studies on this topic, a multicenter study with a large sample of Brazilian participants (n=617) from various states across the country, thereby incorporating physical and cultural demographic variables. Moreover, Britto et al.19 incorporated key elements, such as age, height, gender, BMI, and heart rate, into their equation.
Regarding the other five Brazilian equations,16–19 they showed the largest mean difference between the 6MWD predicted distance and the walked distance. These unsatisfactory results may be explained by the variables of the equations. Despite several predictive factors being used in these equations, other variables should be considered in future studies to improve the agreement with walking distance and create new Brazilian reference equations. On the other hand, all predictive equations tested in this study16–19 have a range of between 46% and 69% remaining in the model to explain the variability in the 6MWT. Therefore, the maximum that an equation can explain or predict in distance walked is 69%, so that a 30% difference would be expected between the real and the predicted distance. This raises the question: how should be the mean difference between the distance walked and predicted distance be understood to ensure that these results do not interfere with the interpretation of the clinical responses of patients?
A recently published systematic review33 reported that the minimal clinically important change to adult subjects with several pulmonary diseases varies from 14 to 30.5m. For healthy individuals, this variation should be even smaller to detect changes in responses to the 6MWT test if they undergo any change in their health condition. However, considering that we might have different results for the same population, we must be careful in interpreting the results, because all equations have possible limitations in predicting the 6MWD. The question is whether such differences are clinically relevant. As noted by Andrianopoulos et al.,10 most of these equations include very similar variables, and the choice of the best equation to use seems to depend more on the characteristics of the subjects, including region and country. The inclusion of other variables, such as level of physical activity, previous diseases, and psychosocial factors, should also be considered to determine if they can improve compliance, since the sociodemographic variables are so widely covered in the equations.
This study was limited by the convenience sample, although the power calculations were based on clinimetric studies.27,28 In addition, handgrip strength was measured only for part of the sample, although we believe the number was sufficient given that it is a direct measurement (n=45).
ConclusionsThe results of the present study showed that, of the six equations tested, the 6MWD predictive equation using age, gender, and BMI proposed by Britto et al.19 for the Brazilian population provided the results that came the closest to predicting the actual results obtained in the present study, demonstrating its suitability for use in clinical practice for healthy Brazilian males.
Conflicts of interestThe authors declare no conflicts of interest.



