



Physical activity levels seem to play a role in patellofemoral pain (PFP); however, few studies have been conducted to confirm this hypothesis.
ObjectivesTo determine the reported pain levels of women with and without PFP who maintain different levels of physical activity; to determine the capability of these levels to predict pain; and to test the capability of two stair-negotiation protocols, with and without external load, to equalize pain between groups.
MethodFour groups were divided based on the women's physical activity levels: moderate activity PFP group (28), moderate activity control group (23), intense activity PFP group (22), and intense activity control group (22). All participants were asked to perform 15 repetitions of stair negotiation with and without external load on a seven-step staircase on two separate days. Pain levels were reported using a visual analog scale at five distinct moments: previous month, before stair negotiation, after stair negotiation, before patellofemoral joint (PFJ) loading protocol, and after PFJ loading protocol.
ResultsThe intense activity PFP group showed higher levels of pain than the moderate activity PFP group (F(8,158)=11.714, p=0.000, η2=0.30). The PFJ loading protocol was able to equalize and exacerbate pain in the PFP groups.
ConclusionIntense physical activity seems to have a higher association with knee pain than moderate physical activity. A PFJ loading protocol may be an alternative to equalize pain in women with PFP during clinical assessments.
Patellofemoral pain (PFP) is a common and costly musculoskeletal disorder that affects men, women, and adolescents, albeit women are 2.23 times more likely to develop PFP than men.1 PFP is characterized by pain around and behind the patella and is aggravated by activities causing repetitive and high patellofemoral compressive forces such as squatting and running.2 Although this disorder accounts for 25–40% of all knee complaints in sports medicine,3 its underlying mechanisms remain unclear.4
The importance of physical activity levels and the overuse of activity have been discussed in some studies and it appears that the stimulus for developing and/or exacerbating PFP may be related to increased physical activity and mechanical overloading.5 Thomeé et al.6 found that individuals with PFP tend to report an insidious onset of symptoms associated with temporary overuse or a period of increased physical activity. Furthermore, Fairbank et al.7 reported that individuals with PFP stated that both their maximal level of pain and average highest level of daily pain were associated with increased physical activity.
Nevertheless, a large number of PFP studies have been performed without taking into account the level of physical activity of the sample.7–9 Likewise, clinicians tend to assess individuals with PFP without considering their physical activity levels.6 However, when all of these subjects are placed in one PFP group, potential misunderstandings might arise. Changes in the type, frequency, duration, and intensity of physical activities may cause a variation in the level of reported pain.5 As musculoskeletal pain has the potential to influence biomechanical characteristics,11 it is possible that different levels of pain may produce distinct mechanical strategies in women with PFP during biomechanical analyses and clinical assessments.12,13 For instance, some studies14,15 have verified a difference in onset timing between the vastus medialis and lateralis among women with and without PFP, while other studies have not.16,17 Recently, Briani et al.11 found that these controversial results may be related to the different levels of physical activity of the women in the samples. Therefore, there seems to be different reports of pain in women with PFP who maintain distinct levels of physical activity. Yet, to date, no study has been conducted to confirm this hypothesis.
Therefore, the first objective of this study was to determine the pain levels reported by women with and without PFP who maintain different levels of physical activity during 5 distinct moments: previous month, before stair negotiation, after stair negotiation, before PFJ loading protocol, and after PFJ loading protocol. The second objective was to determine the capability of different activity levels to predict pain. We hypothesized that: (1) women with PFP who maintained higher levels of physical activity would present higher levels of pain and; (2) higher levels of physical activity would better predict the pain. Given such hypotheses, we proposed a stair negotiation and a PFJ loading protocol in an attempt to equalize the pain between women with PFP who maintain different levels of physical activity. Our hypothesis was that (3) the PFJ loading protocol would equalize the pain in the women with PFP, while the stair negotiation would not.
MethodSubjectsFifty women with PFP and forty-five asymptomatic women were recruited via advertisements placed at the university, parks, and gyms. Based on calculations made in Sample-power using Statistical Software for Social Sciences (SPSS) version 18.0 (SPSS Inc. Chicago, IL, USA) with preliminary data (pilot study), a minimum sample size of 22 women would be needed to evaluate the Visual Analogue Scale (VAS) values with a statistical power of 80%, observing a minimum difference of 1.2cm between means and a standard deviation of 1.6cm and assuming a significance level of 5% and β=0.20. Prior to the data collection, all participants provided written informed consent and the experimental protocol was approved by the Human Research Ethics Committee of the Estadual Paulista “Júlio de Mesquita Filho” (UNESP), Presidente Prudente, SP, Brazil (approval no. 306.729).
Diagnosis of PFP was completed following consensus from two experienced clinicians (>5 years’ experience) and based on definitions used in previous studies.18,19 The inclusion criteria were (1) anterior knee pain during at least two of the following activities: prolonged sitting, squatting, kneeling, running, climbing stairs, and jumping; (2) pain during patellar palpation; (3) symptoms of insidious onset and duration of at least 1 month; (4) worst pain level in the previous month of at least 3cm on a 10-cm VAS; and (5) three or more positive clinical signs in the following tests: Clarke's sign, McConnell test, Noble compression, Waldron test, and patellar pain on palpation. The participants were required to fulfill all five requirements to be included in the study as women with PFP. The presence of the following conditions were carefully screened as exclusion criteria: events of patellar subluxation or dislocation, lower limb inflammatory process, patellar tendon or meniscus tears, bursitis, ligament tears, or the presence of neurological diseases. Those who had undergone knee surgery or received oral steroids, opiate treatment, acupuncture, or physical therapy during the preceding six months were excluded from this study. On the other hand, the participants could not present any signs or symptoms of PFP or other diseases to be admitted in the study as asymptomatic women.
After the screening process, the women with and without PFP were divided into groups according to physical activity level. This division was done using the self-administered International Physical Activity Questionnaire – long form (IPAQ), a valid and reliable form for classifying physical activity levels.20 The levels were determined by the total amount of physical activity in the previous week involving the lower limbs that generate high PFJ stress and classified according to Craig et al.20 With respect to our sample, four groups were formed: moderate activity patellofemoral pain group (MAPFPG=28), moderate activity control group (MACG=23), intense activity patellofemoral pain group (IAPFPG=22) and intense activity control group (IACG=22).
ProcedureThe experimental design of this study was carried out on two separated days in order to avoid influences between protocols. On the first day, right after arriving at the laboratory, all participants were asked to rate their knee pain by putting a mark along a 10-cm linear scale (VAS) indicating the intensity of pain in the previous month (previous month's pain) and the intensity of pain at that moment (before stair-negotiation pain). This rating was then converted to a numerical value.21 This scale has been validated and it is reliable for assessing women with PFP.21 Subsequently, each participant was asked to perform 15 repetitions of stair negotiation on a 7-step staircase at their natural comfortable speed. After the 15 repetitions, the VAS measures were retaken (after stair-negotiation pain). Data collection was obtained for each participant's symptomatic limb (those with unilateral symptoms) or most symptomatic limb (in those with bilateral symptoms).
On the second day, the participants were asked again to rate their knee pain at arrival (pre-PFJ loading protocol pain) and after PFJ loading protocol (post-PFJ loading protocol pain). For this protocol, the participants performed 15 repetitions of stair negotiation with an external load22 of 35% of the subject's body mass allocated in a backpack. This percentage was chosen based on the findings of Wallace et al.,22 who reported 44% and 19% increase of the PFJ stress during the eccentric and concentric phase of knee flexion using this amount of external load, respectively. The pain protocol was conducted to exacerbate the PFP symptoms and thus equalize pain in the women with PFP. This was necessary due to the known characteristic of intermittent periods of pain in individuals with PFP.13 A metronome was used on both days at 96 steps/minute to standardize the cadence of stair negotiation.23 The investigators were blinded concerning the groups and the interval between the two collection periods was 2 to 7 days.16
Enhancing methodological controlIn order to ensure that the PFJ loading protocol did not generate neuromuscular fatigue in the participants, electromyographic data of approximately 30% of the sample (16 controls and 16 women with PFP) were analyzed comparing the signal before and after the PFJ loading protocol. The parameter extracted from the electromyographic data was the median frequency (Fmed) of the vastus medialis (VM) and vastus lateralis (VL), a commonly used parameter in the study of neuromuscular fatigue24,25 in two muscles highly related with this disorder.26 Data collection and processing were done according to previous literature.24,25 As shown in Table 1, no differences were found in the VM or VL for either the control groups or the PFP groups. Therefore, it seems that the PFJ loading protocol did not generate neuromuscular fatigue.
Mean and standard deviation values of electromyographic data before and after the patellofemoral joint loading protocol for both control and PFP groups.
| Parameters | MACG | IACG | MAPFPG | IAPFPG | ||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Fmed VM | 54.5±12.5 | 54.1±11.2 | 57.6±8.2 | 53.5±7.6 | 54.8±10.2 | 52.2±8.3 | 56.2±2.8 | 58.9±5.5 |
| Fmed VL | 53.7±4.8 | 51.0±6.00 | 55.6±7.0 | 58.1±9.7 | 56.4±5.6 | 51.4±6.9 | 56.3±3.6 | 61.2±7.4 |
MACG, moderate activity control group; IACG, intense activity control group; MAPFPG, moderate activity patellofemoral pain group; IAPFPG, intense activity patellofemoral pain group. Pre, before patellofemoral (PFJ) loading protocol; Post, after PFJ loading protocol; Fmed, median frequency; VM, vastus medialis muscle: VL, vastus lateralis muscle.
Descriptive estimates (mean and SD) were obtained using SPSS (version 18.0, SPSS Inc., Chicago, IL, USA). The data were analyzed with respect to their distribution, variance homogeneity, and sphericity using the Shapiro–Wilk W test, Levene's test, and Mauchly's sphericity test, respectively. The independent t-test was used to identify differences in symptom duration between PFP groups. Dependent t tests were used to compare electromyographic data before and after the PFJ loading protocol. The VAS values were compared among moments of pain evaluation within each group (previous month, before stair negotiation, after stair negotiation, before PFJ loading protocol, and after PFJ loading protocol) and among groups (MACG, IACG, MAPFPG, IAPFPG) using a 5-by-4 analysis of variance (ANOVA) (5 moments and 4 groups). The Bonferroni post hoc test was performed for multiple pairwise comparisons where appropriate. The data reported from ANOVA were F values (with degrees of freedom), p values, and eta squared (η2). A linear regression model was developed for both groups with PFP to determine which group had the best prediction of pain. The pain reported in the previous month was used in the regression models (dependent variable) in accordance with other studies.16 Overall performance of the final models was evaluated using Nagelkerke's r2, which estimates explained variation of the model. For all statistical tests, an alpha level of <0.05 was used.
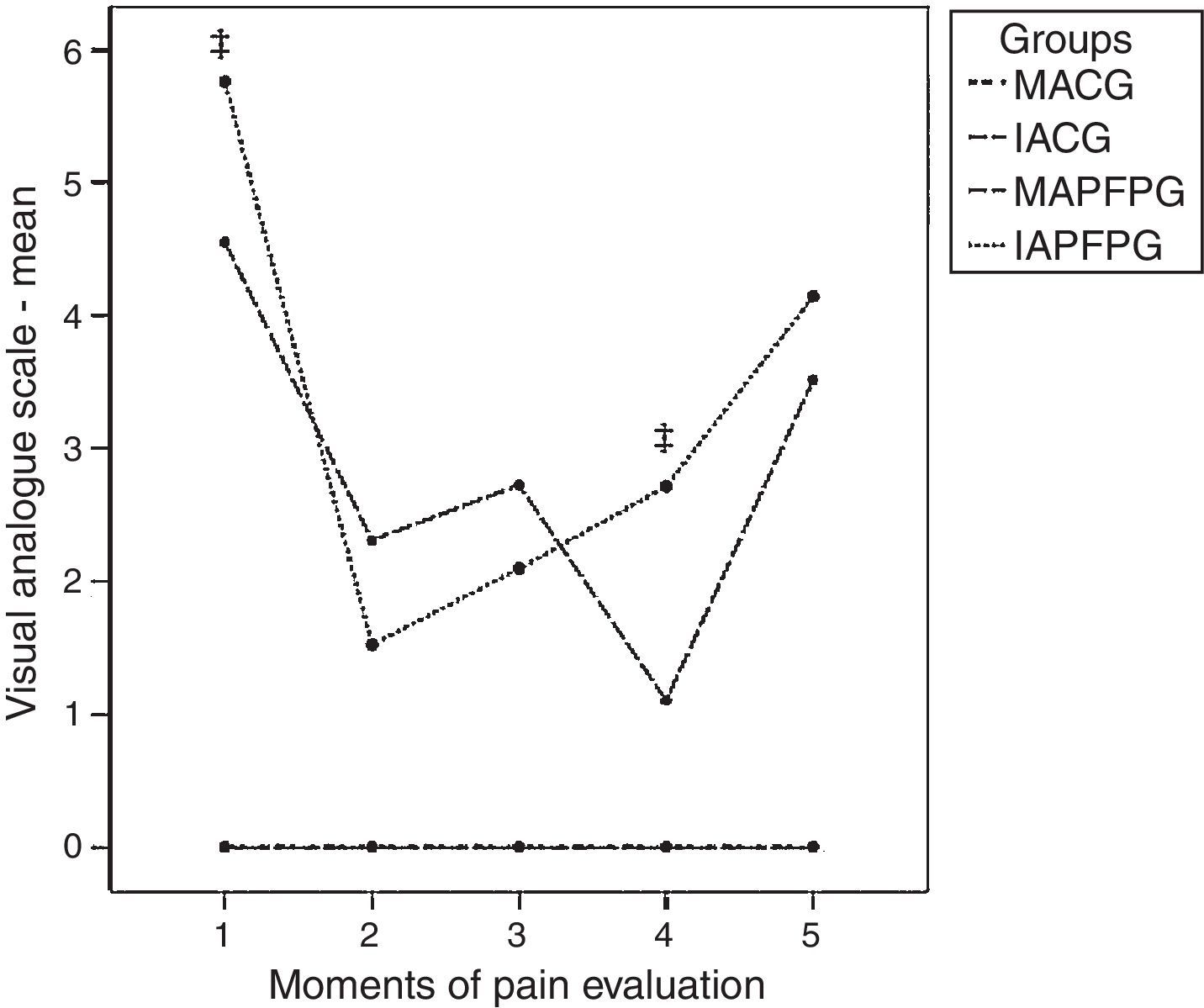
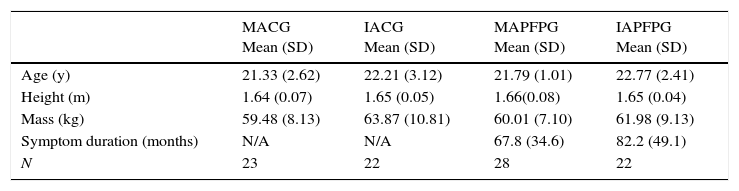
ResultsTable 2 summarizes the demographic characteristics of the groups. The independent t-test for duration of symptom revealed no differences between both groups with PFP (p=0.34). A significant group-by-time interaction was found among the levels of pain and groups (F(8,158)=11.714, p=0.000, η2=0.30) (Fig. 1). Concerning post hoc analysis, the control groups did not differ from each other in any moment of pain evaluation and were different from both PFP groups in all moments. In turn, the MAPFPG and IAPFPG presented different levels of pain in the moments ‘previous month’ and ‘before the PFJ loading protocol’ (mean difference=1.2cm, p=0.000; mean difference=1.6cm, p=0.000; respectively). In contrast, there were no differences between the PFP groups in the moments ‘before stair negotiation’, ‘after stair negotiation’, or ‘after PFJ loading protocol’.
Anthropometric data of the subjects.
| MACG Mean (SD) | IACG Mean (SD) | MAPFPG Mean (SD) | IAPFPG Mean (SD) | |
|---|---|---|---|---|
| Age (y) | 21.33 (2.62) | 22.21 (3.12) | 21.79 (1.01) | 22.77 (2.41) |
| Height (m) | 1.64 (0.07) | 1.65 (0.05) | 1.66(0.08) | 1.65 (0.04) |
| Mass (kg) | 59.48 (8.13) | 63.87 (10.81) | 60.01 (7.10) | 61.98 (9.13) |
| Symptom duration (months) | N/A | N/A | 67.8 (34.6) | 82.2 (49.1) |
| N | 23 | 22 | 28 | 22 |
MACG, moderate activity control group; IACG, intense activity control group; MAPFPG, moderate activity patellofemoral pain group; IAPFPG, intense activity patellofemoral pain group; SD, standard deviation.

Pain variation throughout the moments of evaluation for all groups.
MAPFPG, moderate activity patellofemoral pain group; IAPFPG, intense activity patellofemoral pain group; MACG, moderate activity control group; IACG, intense activity control group; 1: previous month; 2: before stair negotiation; 3: after stair negotiation; 4: before patellofemoral joint loading protocol; 5: after patellofemoral joint loading protocol. As the control groups had zero pain in all moments of pain evaluation, the lines representing these two groups are overlapped. ‡ Significant difference between the MAPFPG and the IAPFPG.
Our results revealed significant effects of time comparing reported pain levels among moments within each group (F(4,79)=26.587, p=0.000, η2=0.25) (Table 3). Post hoc analysis revealed no differences between the moments of the MACG and the IACG, that is, both control groups presented zero pain during all moments of pain evaluation. In the MAPFPG, the moments ‘previous month’, ‘before PFJ loading protocol’ and ‘after PFJ loading protocol’ differed from all moments; the moment ‘before stair negotiation’ was different from all moments except ‘after stair negotiation’ (mean difference=0.41, p=0.10). Similarly, in the IAPFPG the moments ‘previous month’ and ‘after PFJ loading protocol’ differed from all other moments; ‘before stair negotiation’ was different from all moments except ‘after stair negotiation’ (mean difference=0.57, p=0.09); the moment ‘before PFJ loading protocol’ was different from all moments except ‘after stair negotiation’ (mean difference=0.61, p=0.07).
Mean and standard deviation values of VAS for both control and PFP groups.
| Groups | Previous month | Before stair negotiation | After stair negotiation | Before PFJ loading protocol | After PFJ loading protocol |
|---|---|---|---|---|---|
| MACG | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| IACG | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| MAPFPG | 4.5 (1.3) | 2.3 (1.9) | 2.7 (1.9) | 1.1 (1.3) | 3.5 (1.9) |
| IAPFPG | 5.7 (1.5) | 1.5 (2.2) | 2.0 (2.1) | 2.7 (2.3) | 4.1 (2.3) |
MAPFPG, moderate activity patellofemoral pain group; IAPFPG, intense activity patellofemoral pain group; MACG, moderate activity control group; IACG, intense activity control group; VAS, Visual Analogue Scale; PFP, patellofemoral pain.
Results from the regression analysis also confirmed distinct pain behaviors for different physical activity levels in women with PFP (Table 4). Only 1% of pain was predicted by moderate levels of physical activity with no significance (p=0.61). On the other hand, intense levels of physical activity predicted 32% of pain (p=0.007).
Linear regression model with IPAQ and VAS for PFP groups.
| Models | Groups | R | R2 change | F-ANOVA | β (95% CI) | p-value |
|---|---|---|---|---|---|---|
| Model 1 | MAPFPG | 0.01 | −0.02 | 0.274 | 0.099 (−0.001; 0.001) | 0.605 |
| Model 2 | IAPFPG | 0.32 | 0.29 | 9.183 | 0.571 (0.002; 0.751) | 0.007* |
IPAQ, International Physical Activity Questionnaire; MAPFPG, moderate activity patellofemoral pain group; IAPFPG, intense activity patellofemoral pain group; 95% CI, 95% confidence interval; VAS, Visual Analogue Scale; PFP, patellofemoral pain.
Our findings demonstrated that women with PFP who maintain high levels of physical activity have higher levels of pain than those who maintain moderate levels of physical activity. Moreover, our results showed that the PFJ loading protocol may be a good alternative to exacerbate and equalize the pain in women with PFP.
Increased pain levels were found in the moments ‘previous month’ and ‘before PFJ loading protocol’ for the IAPFPG compared to the MAPFPG. It has been advocated that the higher the levels of physical activity are, the greater the knee pain of individuals with PFP.5 This may occur due to the elevated exposure of the PFJ to excessive joint stress during bodyweight loading activities.22 Excessive joint stress has been linked to articular cartilage degradation and may contribute to knee pathologies such as PFP.27,28 Therefore, our findings support the hypothesis that women with PFP who maintain higher levels of physical activity are more susceptible to elevated levels of pain than those who maintain moderate levels of physical activity.
Regression analysis provided better understanding of the influence of physical activity on pain. Intense levels of physical activity predicted 32% of PFP, whereas only 1% of PFP was predicted by moderate levels of physical activity. Nevertheless, along with the knee pain, alterations in biomechanical characteristics also seem to arise.11 Van Tiggelen et al.14 prospectively accompanied men submitted to 6 weeks of basic military training (BMT) and found that, before the BMT, 57.6% of the men with PFP presented delayed onset of VM activity and, interestingly, after the BMT, 100% of the men with PFP demonstrated that delay. Furthermore, Briani et al.11 found that women with PFP who maintained high levels of physical activity presented delayed onset of VM activity compared to controls, while women with PFP who maintained moderate levels of physical activity did not. Therefore, when women with distinct levels of physical activity are considered in the same sample or are assessed in the same way, discrepancies regarding the levels of pain may cause distinct biomechanical behaviors in this population.
Given the apparent differences in the level of pain and biomechanical characteristics in women with PFP who maintain distinct levels of physical activity, it would be of great value to be able to equalize the levels of pain of these individuals in order to minimize the potential confounding factor during assessments and data collections. Our results demonstrated that after both protocols (stair negotiation with and without external load), the women with PFP who maintained different levels of physical activity did not present distinct levels of pain. However, care should be taken in interpreting these results. Firstly, although no differences were found between the PFP groups after the stair negotiation protocol without external load, the groups were already similar in the moment ‘before stair negotiation’. As such, the stair negotiation protocol did not change the groups from a state of difference to a state of non-difference as the PFJ loading protocol did. Secondly, for both PFP groups, there were no differences when comparing the before and after stair negotiation moments, which demonstrates that 15 repetitions of stair negotiation without an external load were not capable of exacerbating pain in the women with PFP. Therefore, considering these results, the PFJ loading protocol seems an appropriate method of exacerbating and equalizing pain in women with PFP who maintain distinct levels of physical activity.
Our findings raise some relevant points that should be considered by clinicians and researchers. Firstly, the levels of physical activity of the women with PFP should be evaluated in the studies, and groups with the same levels of physical activity should be created rather than grouping all participants in a single group. Secondly, clinicians should give special attention to women with PFP who maintain high levels of physical activity due to their increased exposure to activities that cause excessive PFJ stress. The overload seems an important subject that should be taken into account in clinical assessments of women with PFP. Thirdly, if a sample is composed of women with PFP who maintain distinct levels of physical activity, a PFJ loading protocol should be used in order to equalize the pain among them.
Some limitations of the present study should be acknowledged. Firstly, the sample included only women. Despite the importance of the study of this subgroup given that it is the most likely to suffer from PFP, the results cannot be generalizable to the entire population of people with PFP. Secondly, although PFP is related to physical activity, the study did not include a group of inactive women with PFP, which prevents generalization of the results to those individuals. Thirdly, the order of the protocols was not randomized, which would have enhanced the methodological quality of the study. Therefore, future studies should include men and inactive individuals and compare them to different physical activity level groups in order to observe their response to the PFJ loading protocol in a randomized fashion.
Our results support the premise that women with PFP who maintained intense levels of physical activity have higher pain levels than those who maintain moderate levels of physical activity. Furthermore, high levels of physical activity predict pain in women with PFP better than moderate levels do. Finally, a PFJ loading protocol seems to be a relevant alternative to equalize and exacerbate pain in women with PFP.
Conflicts of interestThe authors declare no conflicts of interest.



