
Measurements of respiratory muscle strength are widely used for assessment in children; however, clearly defined predictive equations for the Brazilian pediatric population have yet to be established.
ObjectiveTo determine the prediction equations for maximal respiratory pressures in healthy children.
MethodCross-sectional observational study with normal-weight students aged 7–10 years (n=399, 198 boys) with health attested by the (International Study of Asthma and Allergies in Childhood) questionnaire and medical history. Biometric data were evaluated (weight, height, and body mass index) as predictors. Spirometry and maximal expiratory pressure values were measured according to the recommendations of the American Thoracic Society. To verify data normality, the Shapiro–Wilk test was applied, and Pearson's test was used to verify the correlation between variables. The models were developed using simple linear regression and multivariate analyses. For all tests, the significance level was p<0.05.
ResultsBoys showed higher values of maximal respiratory pressures than girls, both increasing with age. For boys, these values had moderate correlation with age, weight, and height and weak correlation with body mass index. For girls, maximum inspiratory pressure had a weak correlation with age and moderate correlation with biometric data. Maximum expiratory pressure had a moderate correlation with age and biometric measures. The best predictive models were found in boys: Log(MIP)=1.577+0.006×weight (kg) (R2aj=14.1%) and Log(MEP)=1.282+0.409×height (m) (R2aj=13.9%); and for girls: Log(MIP)=1.548+0.006×weight (kg) (R2aj=15.0%) and Log(MEP)=1.524+0.012×age (years)+0.005×weight (kg) (R2aj=21.6%).
ConclusionPrediction equations for maximal respiratory pressures were developed for boys and girls. The biometric measurements were shown to have a weak influence on the results.
The evaluation and monitoring of respiratory function in children have improved significantly in the last 30 years. Technological advances, more reliable studies, and the recognition of the importance of monitoring in clinical practice have all contributed to a better understanding of lung function in the pediatric age range.1,2
The parameters often analyzed for respiratory function are maximal respiratory pressures (MRP), which are synonymous with respiratory muscle strength (RMS).3,4 The respiratory muscles are responsible for generating the pressure differences that ensure ventilation. Strength is considered an essential measure in the evaluation of various health conditions and monitoring of respiratory muscle weakness in different illnesses.5–7
The MRP test consists of a non-invasive method and simple measurements; however, it requires the subject's cooperation for its proper implementation. The MRP test is a useful tool to assess the response to outpatient physical therapy procedures, respiratory rehabilitation programs, and hospital treatment. It is also useful for assessing ventilatory muscle function in pre- and postoperative situations and assessing the possibility of weaning from mechanical ventilation.4
The MRP test can be used to measure the severity of symptoms and for follow-up in neuromuscular and lung diseases, to guide procedures, and to prevent complications and exacerbations of lung diseases that result in respiratory muscle weakness. The indications of the MRP tests involve differential diagnosis of dyspnea and restrictive disorders without apparent cause. It is also part of diagnostic confirmation of dysfunction of the respiratory muscles in cases such as neuromuscular diseases, chest deformities, and diaphragmatic paralysis.8
The instrument commonly used to measure the MRP is the manometer. This device is considered useful because it is a simple, non-invasive form of measurement that involves compact and easily transportable devices.
Despite these conveniences, the reference values for MRP vary greatly,9–13 possibly due to a lack of standardization of instruments and different collection techniques.14 Moreover, measuring MRP requires the subject's full cooperation, which could underestimate the values of MRP even in the absence of muscle weakness.15
In children, there was an increase in the MRP values with increasing age.16–18 While there are no categorical statements about the size of the contribution of anthropometric variables on RMS, some authors observed a positive correlation between the MRP and weight9,18,19 and height.18,19 Other studies11,12,19 indicate the need for regional research on reference values for MRP because of the territorial dimensions and ethnic diversity of the Brazilian population. To date, there is no consensus on the MRP reference values nor on the contribution of the variables that correlate in the equations. There are indications that local differences have a strong influence on these results.
Determining reference equations allows the comparison between different populations and assists in gathering more accurate information on respiratory disorders that are related to changes in the parameters evaluated. For Brazilian children, there are few recent papers on reference values and prediction equations for schoolchildren between aged 7 and 10.8,20–23
The aim of this study was to determine predictive equations for MRP in children aged 7–10 and to compare normal MRP values established by different studies (including those the present study) with the values obtained for children aged 7–10.
MethodsThis is a cross-sectional observational study conducted in the school district of Florianópolis, SC, Brazil from February to April 2013. The study was approved by the Human Research Ethics Committee of Universidade do Estado de Santa Catarina (UDESC), Florianópolis, SC, Brazil (CAAE 01821712.6.0000.0118/opinion 63455). The participating schools were nominated by the Continued Training Department of the State of Santa Catarina (SC) and included two municipal schools and one state school. The three public schools were contacted and agreed to take part in the study. All schoolchildren in the proposed age group were invited to participate in the study. All those who gave written consent and had approval from the parents/guardians underwent assessment. Only the schoolchildren who met the previously established inclusion criteria were included in the final sample.
The study included healthy students of both sexes, aged 7–10 years, between the 3rd and 85th percentile according to the Brazilian Health Ministry,24 able to understand and complete all tests. The exclusion criteria were as follows: presence or history of respiratory disease identified by the International Study of Asthma and Allergies (ISAAC), questionnaire,25,26 cardiac, neuromuscular, neurological, or rheumatologic disease, acute disease at the time of data collection, inability to perform any of the assessments properly, and dubious answers in the questionnaires. Underweight, overweight, or obese children and children with forced expiratory volume in one second (FEV1) less than 80% predicted by Polgar and Weng27 were also excluded.
The children's health was investigated using the ISAAC questionnaire administered by the parent or guardian. This questionnaire measures respiratory symptoms and it is used to assess the prevalence of asthma, rhinitis, and eczema, with questions relating to symptoms in the last 12 months. Modules 1 and 2, relating to asthma25 and rhinitis,26 were applied. The parents/guardians also answered a questionnaire prepared by the researchers with questions related to physical activity, use of medication (especially those that affect muscles), previous surgery and reasons for hospital admissions, previous and current illnesses, and hospital admissions, as well as gestational and neonatal history. The children in the study showed no hearing or sight problems and no musculoskeletal deformities, including chest deformities.
For the day of data collection, the parents/guardians were instructed to dress the children in comfortable clothing (school uniform) and follow their usual school day routine. Students were allowed to have the meals provided by the school, which were considered balanced, and to practice the normal physical activities of their school. To ensure that the children did not show any signs of fatigue before the assessment, they had 15min of rest before the start of the data collection.
First, weight (accuracy 0.1kg) and height (accuracy 0.5cm) were measured with a scale and stadiometer (Welmy, W-200/5, Brazil). These measures were taken with the child standing with bare feet, upright and aligned body, and with heels, calves, buttocks, shoulder blades, and occipital region touching the stadiometer. Subsequently, the weight of the uniform (150g for the shirt and shorts or 250g for the pants) were subtracted from the weight value measured on the scale. The weight and height values were used to calculate the body weight index (BMI) in the pediatric BMI calculator of the Ministry of Health.24 The child's sex and age were also inserted to obtain a health diagnosis and percentile.
After the anthropometric assessment, FEV1% (percentage of forced expiratory volume in one second compared to predicted) was measured using a digital monitor (Piko-1, nSpire Health, USA), according to ATS guidelines and criteria.28 The child sat with their back against the back of the chair, aligned and neutral head, and upper limbs resting on the lower limbs. Making use of a nose clip, the child was asked to perform maximal inspiration, then forced and maximum expiration, with verbal encouragement. Three measurements were taken with a 30-s interval between them (the two largest values had to be within 0.15L of each other) and the highest value was used in the analysis. A maximum of five maneuvers was allowed, and if no acceptable and reproducible measurements were obtained, the test was disregarded.
Next, RMS was measured using a digital manometer with a unidirectional valve (MVD300, L-MED, Brazil) and considering a pressure of ±300mmHg. After providing instructions and demonstrations of the test, the evaluator gave verbal encouragement to the child who was performing the respiratory maneuvers. The child wore a nose clip and breathed into a mouthpiece connected to a 1.5mm diameter tube. The measurements were conducted according to ATS recommendations for the evaluation of RMS.3 To obtain the maximum inspiratory pressure (MIP), the child exhaled to near residual volume and then performed a maximal inspiration. Maximal expiratory pressure (MEP) was measured from inspiration close to total lung capacity, followed by maximum expiration. The child performed a minimum of three and a maximum of seven maneuvers for each of the measurements of MIP and MEP. The measurements were considered satisfactory when the maximum value of three maneuvers was acceptable (no leaks and lasting for at least 2s) and reproducible (varying less than 20% of each other). Regarding the measurements of maximal inspiratory and expiratory pressures, we only considered the peak pressures.
To avoid fatigue during the test, a 30–40-s interval was allowed after each maneuver of each measurement and a 3-min interval was allowed between the MRP measurements. The highest value for MIP and MEP was recorded, excluding the last maneuver, to control for a possible learning effect. All evaluations were conducted by the same examiner.
For the regression analysis, we considered a specific model for each sex given that sexual dimorphism plays an important role in muscle strength.13 In this model, we determined four predictor variables: age, weight, height, and BMI. According to Freund and Simon,29 at least 20 individuals are required for each predictor variable, therefore 80 students of each sex were required for analysis.
For data analysis and statistical processing, we used SPSS version 16.0 for Windows. Initially, we used descriptive statistics and frequencies, and the data were expressed as mean and standard deviation. The Shapiro–Wilk test was used to test the normality of the distribution of the variables. Based on this result, the MRP values were normalized by base-10 logarithm transformation due to the non-normal distribution of the dependent variables (MIP and MEP). Wilcoxon's non-parametric test was used to compare the results of MIP and MEP obtained by applying the equations available in the literature using data from the sample according to sex and age. The correlations between MRP and possible predictor variables were identified using Pearson's correlation coefficient and, as a result, the predictive MIP and MEP equations for each sex were developed using multiple linear regression. Age, weight, height, and BMI were considered predictor variables. Multivariate models were generated by linear regression incorporating these variables by the stepwise method. The multicollinearity between the predictor variables age, weight, height, and BMI was assessed by examining tolerance and the variance inflation factor (VIF). To assess the goodness-of-fit of the model, we performed an analysis of the residuals, which should have zero mean and normal distribution. The significance adopted in all tests was 5% (α=0.05).
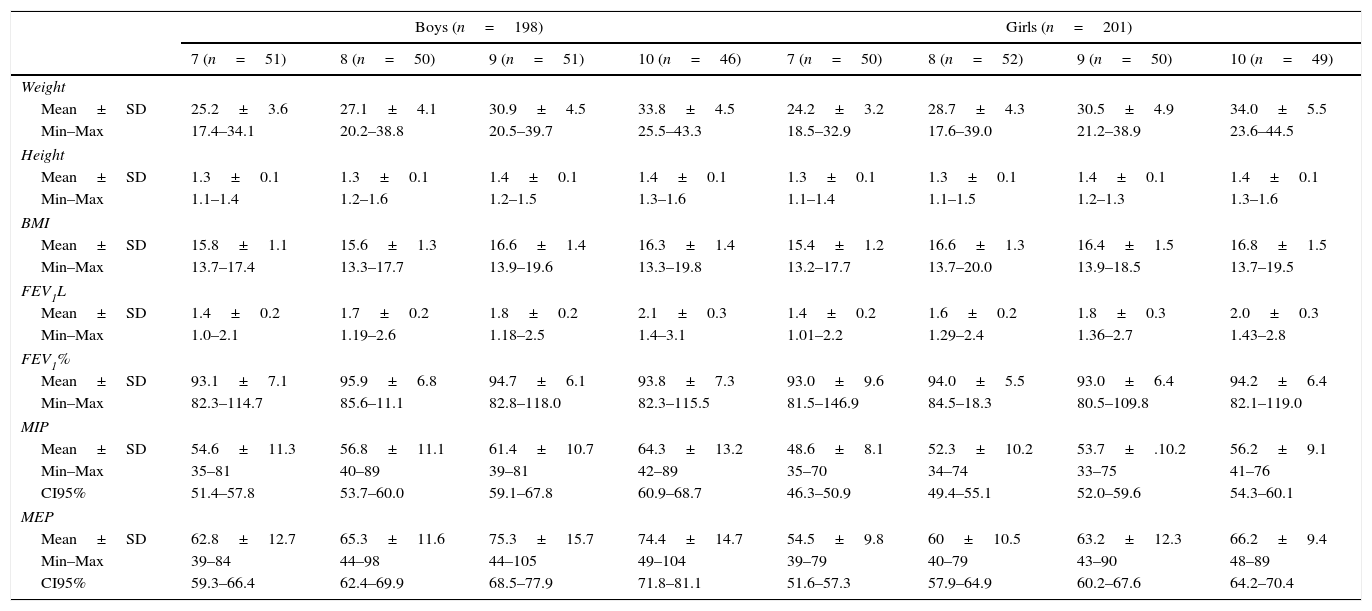
Results625 children were evaluated. Of these, 119 were excluded due to low weight (n=2), overweight (n=83), or obesity (n=34) and 73 due to history of disease or FEV1 below 80% predicted. Twelve were unable to perform the test according to the established criteria, 8 refused to participate, and 9 were not present on the day of collection. The records of 404 students remained, which were used to identify outliers in the dependent variables (MIP and MEP) and in the biometric variables (weight, height, and BMI). Next, the data of 399 students were analyzed, including 101 students aged 7 (51 boys), 102 aged 8 (50 boys), 101 aged 9 (51 boys), and 95 aged 10 (46 boys). The descriptive data for the observed variables according to sex and age are shown in Table 1.
Anthropometric and ventilatory variables according to sex and age.
| Boys (n=198) | Girls (n=201) | |||||||
|---|---|---|---|---|---|---|---|---|
| 7 (n=51) | 8 (n=50) | 9 (n=51) | 10 (n=46) | 7 (n=50) | 8 (n=52) | 9 (n=50) | 10 (n=49) | |
| Weight | ||||||||
| Mean±SD | 25.2±3.6 | 27.1±4.1 | 30.9±4.5 | 33.8±4.5 | 24.2±3.2 | 28.7±4.3 | 30.5±4.9 | 34.0±5.5 |
| Min–Max | 17.4–34.1 | 20.2–38.8 | 20.5–39.7 | 25.5–43.3 | 18.5–32.9 | 17.6–39.0 | 21.2–38.9 | 23.6–44.5 |
| Height | ||||||||
| Mean±SD | 1.3±0.1 | 1.3±0.1 | 1.4±0.1 | 1.4±0.1 | 1.3±0.1 | 1.3±0.1 | 1.4±0.1 | 1.4±0.1 |
| Min–Max | 1.1–1.4 | 1.2–1.6 | 1.2–1.5 | 1.3–1.6 | 1.1–1.4 | 1.1–1.5 | 1.2–1.3 | 1.3–1.6 |
| BMI | ||||||||
| Mean±SD | 15.8±1.1 | 15.6±1.3 | 16.6±1.4 | 16.3±1.4 | 15.4±1.2 | 16.6±1.3 | 16.4±1.5 | 16.8±1.5 |
| Min–Max | 13.7–17.4 | 13.3–17.7 | 13.9–19.6 | 13.3–19.8 | 13.2–17.7 | 13.7–20.0 | 13.9–18.5 | 13.7–19.5 |
| FEV1L | ||||||||
| Mean±SD | 1.4±0.2 | 1.7±0.2 | 1.8±0.2 | 2.1±0.3 | 1.4±0.2 | 1.6±0.2 | 1.8±0.3 | 2.0±0.3 |
| Min–Max | 1.0–2.1 | 1.19–2.6 | 1.18–2.5 | 1.4–3.1 | 1.01–2.2 | 1.29–2.4 | 1.36–2.7 | 1.43–2.8 |
| FEV1% | ||||||||
| Mean±SD | 93.1±7.1 | 95.9±6.8 | 94.7±6.1 | 93.8±7.3 | 93.0±9.6 | 94.0±5.5 | 93.0±6.4 | 94.2±6.4 |
| Min–Max | 82.3–114.7 | 85.6–11.1 | 82.8–118.0 | 82.3–115.5 | 81.5–146.9 | 84.5–18.3 | 80.5–109.8 | 82.1–119.0 |
| MIP | ||||||||
| Mean±SD | 54.6±11.3 | 56.8±11.1 | 61.4±10.7 | 64.3±13.2 | 48.6±8.1 | 52.3±10.2 | 53.7±.10.2 | 56.2±9.1 |
| Min–Max | 35–81 | 40–89 | 39–81 | 42–89 | 35–70 | 34–74 | 33–75 | 41–76 |
| CI95% | 51.4–57.8 | 53.7–60.0 | 59.1–67.8 | 60.9–68.7 | 46.3–50.9 | 49.4–55.1 | 52.0–59.6 | 54.3–60.1 |
| MEP | ||||||||
| Mean±SD | 62.8±12.7 | 65.3±11.6 | 75.3±15.7 | 74.4±14.7 | 54.5±9.8 | 60±10.5 | 63.2±12.3 | 66.2±9.4 |
| Min–Max | 39–84 | 44–98 | 44–105 | 49–104 | 39–79 | 40–79 | 43–90 | 48–89 |
| CI95% | 59.3–66.4 | 62.4–69.9 | 68.5–77.9 | 71.8–81.1 | 51.6–57.3 | 57.9–64.9 | 60.2–67.6 | 64.2–70.4 |
Age (years); weight (kg); height (m); BMI, weight/height2; FEV1L, forced expiratory volume in first second (L); FEV1%, percentage of forced expiratory volume in 1s compared to predicted; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure; SD, standard deviation; Min, minimum; Max, maximum; CI95%, confidence interval 95%.
The MRP values were higher in boys compared to girls (p<0.05) of all ages except in the MEP of the students aged 8 (p=0.08). In the analysis by age group, the MRP values increased significantly with age in males, except for the comparisons between students aged 7 and 8 (MIP/MEP: p=0.31/0.33) and aged 9 and 10 (p=0.43/0.33). The MIP in females aged 7 and 8 (p=0.06) and both pressures (MIP/MEP) at age 8 and 9 (p=0.22/0.34) and 9 and 10 (0.39/0.14) did not show the same behavior.
When we applied the anthropometric data of this sample to the reference equations available in the literature, we found that the absolute values of MRP were numerically lower but not significantly different than those predicted by the mathematical models, except in relation to the MEP published by Arnall et al.30
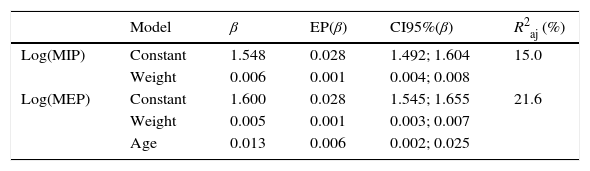
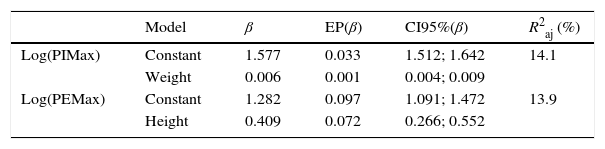
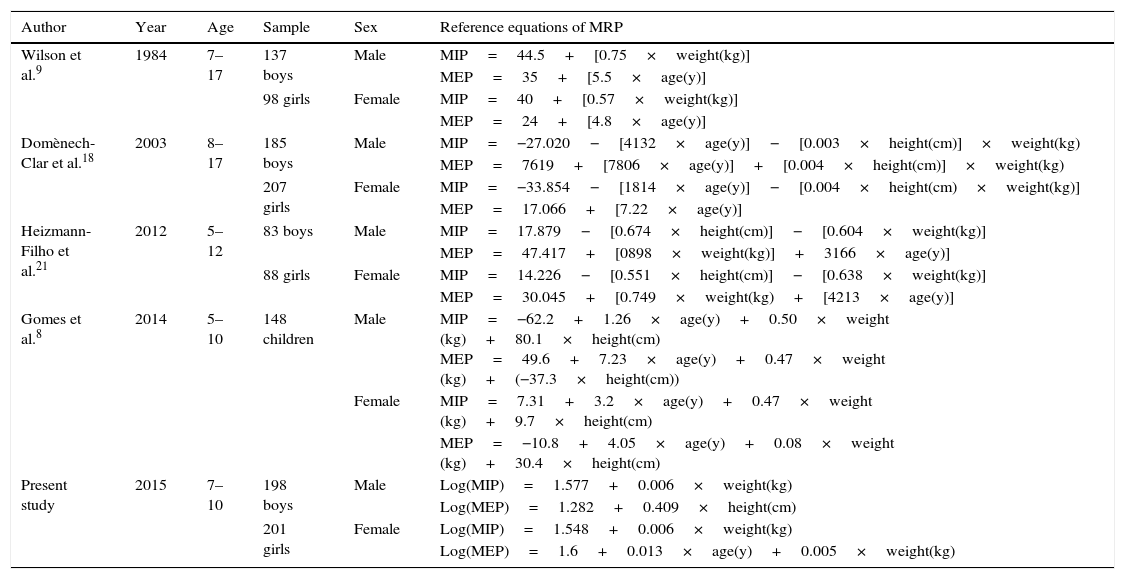
The multivariate models generated by multiple linear regression identified low values for the adjusted coefficients of determination, as shown in Tables 2 and 3. The equations for the proposed MRP were developed separately for boys and girls. For boys: Log(MIP): 1.577+0.006×weight; Log(MEP): 1.282+0.409×height. For girls: Log(MIP): 1.548+0.006×weight; Log(MEP): 1.6+0.013×age×0.005×weight. Table 4 shows the comparison between different predictive equations developed for children, and Table 5 shows the MRP values in different studies, considering the 7–10 age group.
Prediction equations for maximal respiratory pressure for girls.
| Model | β | EP(β) | CI95%(β) | R2aj (%) | |
|---|---|---|---|---|---|
| Log(MIP) | Constant | 1.548 | 0.028 | 1.492; 1.604 | 15.0 |
| Weight | 0.006 | 0.001 | 0.004; 0.008 | ||
| Log(MEP) | Constant | 1.600 | 0.028 | 1.545; 1.655 | 21.6 |
| Weight | 0.005 | 0.001 | 0.003; 0.007 | ||
| Age | 0.013 | 0.006 | 0.002; 0.025 |
MRP, maximal respiratory pressures; Log(MIP), logarithm of maximal inspiratory pressure; Log(MEP), logarithm of maximal expiratory pressure; β, coefficient of regression; EP(β), Standard Error of the coefficient of regression; IC95%(β), confidence interval 95% of the regression coefficients; R2aj, adjusted coefficient of determination.
Prediction equations for maximal respiratory pressure for boys.
| Model | β | EP(β) | CI95%(β) | R2aj (%) | |
|---|---|---|---|---|---|
| Log(PIMax) | Constant | 1.577 | 0.033 | 1.512; 1.642 | 14.1 |
| Weight | 0.006 | 0.001 | 0.004; 0.009 | ||
| Log(PEMax) | Constant | 1.282 | 0.097 | 1.091; 1.472 | 13.9 |
| Height | 0.409 | 0.072 | 0.266; 0.552 |
MRP, maximal respiratory pressures; Log(MIP), logarithm of maximal inspiratory pressure; Log(MEP), logarithm of maximal expiratory pressure; β, coefficient of regression; EP(β), Standard Error of the coefficient of regression; IC95%(β), confidence interval 95% of the regression coefficients; R2aj, adjusted coefficient of determination.
Comparison between the MRP reference equations according to sex.
| Author | Year | Age | Sample | Sex | Reference equations of MRP |
|---|---|---|---|---|---|
| Wilson et al.9 | 1984 | 7–17 | 137 boys | Male | MIP=44.5+[0.75×weight(kg)] |
| MEP=35+[5.5×age(y)] | |||||
| 98 girls | Female | MIP=40+[0.57×weight(kg)] | |||
| MEP=24+[4.8×age(y)] | |||||
| Domènech-Clar et al.18 | 2003 | 8–17 | 185 boys | Male | MIP=−27.020−[4132×age(y)]−[0.003×height(cm)]×weight(kg) |
| MEP=7619+[7806×age(y)]+[0.004×height(cm)]×weight(kg) | |||||
| 207 girls | Female | MIP=−33.854−[1814×age(y)]−[0.004×height(cm)×weight(kg)] | |||
| MEP=17.066+[7.22×age(y)] | |||||
| Heizmann-Filho et al.21 | 2012 | 5–12 | 83 boys | Male | MIP=17.879−[0.674×height(cm)]−[0.604×weight(kg)] |
| MEP=47.417+[0898×weight(kg)]+3166×age(y)] | |||||
| 88 girls | Female | MIP=14.226−[0.551×height(cm)]−[0.638×weight(kg)] | |||
| MEP=30.045+[0.749×weight(kg)+[4213×age(y)] | |||||
| Gomes et al.8 | 2014 | 5–10 | 148 children | Male | MIP=−62.2+1.26×age(y)+0.50×weight (kg)+80.1×height(cm) MEP=49.6+7.23×age(y)+0.47×weight (kg)+(−37.3×height(cm)) |
| Female | MIP=7.31+3.2×age(y)+0.47×weight (kg)+9.7×height(cm) | ||||
| MEP=−10.8+4.05×age(y)+0.08×weight (kg)+30.4×height(cm) | |||||
| Present study | 2015 | 7–10 | 198 boys | Male | Log(MIP)=1.577+0.006×weight(kg) |
| Log(MEP)=1.282+0.409×height(cm) | |||||
| 201 girls | Female | Log(MIP)=1.548+0.006×weight(kg) | |||
| Log(MEP)=1.6+0.013×age(y)+0.005×weight(kg) |
Age (years); weight (kg); height (m); MRP, maximal respiratory pressures; Log(MIP), logarithm of maximal inspiratory pressure; Log(MEP), logarithm of maximal expiratory pressure; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure.
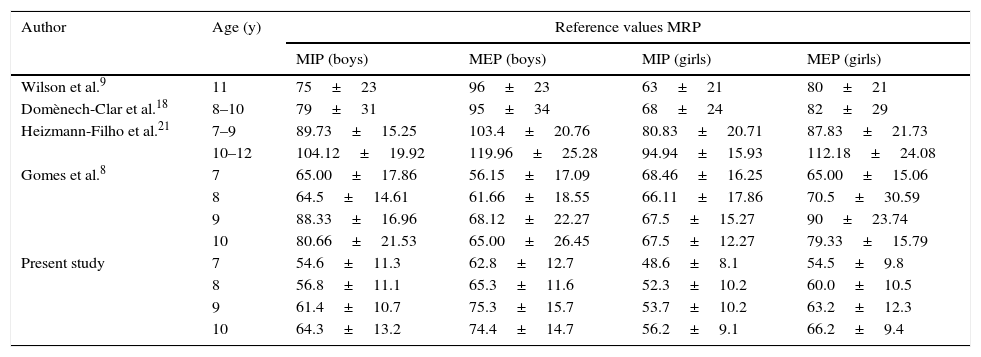
Comparison of the MRP reference values according to age and gender.
| Author | Age (y) | Reference values MRP | |||
|---|---|---|---|---|---|
| MIP (boys) | MEP (boys) | MIP (girls) | MEP (girls) | ||
| Wilson et al.9 | 11 | 75±23 | 96±23 | 63±21 | 80±21 |
| Domènech-Clar et al.18 | 8–10 | 79±31 | 95±34 | 68±24 | 82±29 |
| Heizmann-Filho et al.21 | 7–9 | 89.73±15.25 | 103.4±20.76 | 80.83±20.71 | 87.83±21.73 |
| 10–12 | 104.12±19.92 | 119.96±25.28 | 94.94±15.93 | 112.18±24.08 | |
| Gomes et al.8 | 7 | 65.00±17.86 | 56.15±17.09 | 68.46±16.25 | 65.00±15.06 |
| 8 | 64.5±14.61 | 61.66±18.55 | 66.11±17.86 | 70.5±30.59 | |
| 9 | 88.33±16.96 | 68.12±22.27 | 67.5±15.27 | 90±23.74 | |
| 10 | 80.66±21.53 | 65.00±26.45 | 67.5±12.27 | 79.33±15.79 | |
| Present study | 7 | 54.6±11.3 | 62.8±12.7 | 48.6±8.1 | 54.5±9.8 |
| 8 | 56.8±11.1 | 65.3±11.6 | 52.3±10.2 | 60.0±10.5 | |
| 9 | 61.4±10.7 | 75.3±15.7 | 53.7±10.2 | 63.2±12.3 | |
| 10 | 64.3±13.2 | 74.4±14.7 | 56.2±9.1 | 66.2±9.4 | |
y, years; MRP, maximal respiratory pressure; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure.
The determination of reference values and predictive equations for the MRP of children has been studied by many researchers.9,16–19,21,22 Biometric measurements and ventilatory parameters are set out to establish these values, but there is no consensus on the relationship between these elements and RMS.
This study analyzed the data of 399 students, aged 7–10 years, in order to generate a predictive model of MRP. Among the studies on the subject, this study involved the largest sample in this age group. The other studies, with the exception of one,21 did not conduct their analysis by age but by period of life. Although these equations allow the calculation of predicted values for any age within the age range, the present study classified the participants and presented the mean pressures according to age as in the study of Gomes et al.,8 who evaluated 148 Brazilian children aged 7–10 years. This stratification aimed to identify differences in MRP to avoid possible generalizations of reference values for age and enable comparisons between data from different age ranges. The reason for that is children undergo major morphological changes during their development, making it difficult to establish parallels between children age 6 and adolescents age 12, for example.
As described in the literature,7–9,16,20–22,30–32 higher MRP values were found in males and these values increased over time. The study that evaluated the MRP at each age19 in general also demonstrated this progressive behavior in the values for pressures, as did other studies.16,18,22,30 As expected, correlations were found between MRPs and anthropometric measurements.
Another important point relates to the identification of the participation of each predictor variable that correlated with the logs of the MRPs in the RMS, because it was the basis for the development of the equation models by simple linear regression. It was observed that the biometric measures did little to explain the children's RMS. For boys, the best predictors were weight for Log(MIP) and height for Log(MEP). Weight was also a predictor in the equation for girls for Log(MIP). As for Log(MEP), weight was combined with age.
A possible reason why weight is a predictor variable of these equations is because increases in muscle weight accompany gains in body weight. Four other proposed equations6,16,17,20 also identified the participation of this variable. As in the present study, Domènech-Clar et al.18 noted the presence of height in the equations for MEP. This measure, a predictor of Log(MEP) in the boys studied here, is considered the primary influence in spirometric tests of lung function, whose values increase with height.27,28 Another element pointed out in the equation developed for girls was age. Age is a common variable in some equations for MIP18,30 and MEP9,21 and it was a good predictor in the study of Tomalak et al.32
Most of the studies involving the development of predictive equations for MRP have a common element: the tendency toward low coefficients of determination (R2). Wilson et al.9 found that the R2 for MIP was around 18% for boys and 10.8% for girls. Slightly higher values were observed in girls in the studies of Domènech-Clar et al.18 (MIP/MEP R2=21%/28%) and Barreto22 (R2=26.3%/18.1%) and in boys in the study of Arnall et al.30 (R2=26%/18%). In the study of Gomes et al., the R2 values adjusted for MIP were 0.63 for boys and 0.48 for girls. As for the MEP, the adjusted R2 were 0.25 and 0.55, respectively. Only Heinzmann-Filho et al.21 published better results for both MIP and for MEP in boys and girls: 58.6% and 58.9%; 46.4% and 51.5%, respectively. Schmidt et al.20 did not submit these data.
Despite some methodological differences already pointed out (i.e., the sample size and collection technique widely discussed in the studies22), there was no significant difference between the MRP values and the results of the application of the anthropometric data of this sample in the equations available in the literature. This reflects a certain agreement between the mathematical models generated to date, but does not rule out what has been suggested in the literature on the subject, that is, the need for regional MRP reference values. In line with this, Neder et al.11 presented reference values for adult and elderly subjects from São Paulo, Brazil. These values were compared with a similar sample from Minas Gerais, Brazil, in the study of Parreira et al.,19 however it was not possible to predict the MRP of the participants from that state. In a study similar to Neder et al.,11 Costa et al.12 were also unable to translate their results for MRP using other equations. Likewise, the equations of Wilson et al.,9 Domènech-Clar et al.,18 and Schmidt et al.20 could not predict the values of Barreto,22 and the reference values of Tomalak et al.32 and Domenèch-Clar et al.18 did not correspond to the findings by Heinzmann-Filho et al.21 The most recent study on this topic is by Delgado et al.31, who compared the MIP and MEP of Brazilian children aged 7–11 years with the studies of Gaultier and Zinman16, Szeinberg et al.,17 and Domenèch-Clar et al.18. As in these comparisons, there are still major differences in values between the assessed populations regarding age and ethnicity as well as the measurement of maximal expiratory pressure values involved in the studies.
One of the limitations of this study was its specific and restricted area. Another limitation is the fact that the degree of motivation and cooperation of the children was not assessed objectively. This factor may have influenced the low coefficients of determination and values in our findings.
Conflicts of interestThe authors declare no conflicts of interest.



