



Psychosomatic symptoms seem to influence both the onset and development of pain. There is lack of Brazilian-Portuguese questionnaires that measure psychosomatic symptoms in children and adolescents.
ObjectiveTo translate and cross-culturally adapt the Psychosomatic Questionnaire for Children and Adolescents into Brazilian-Portuguese and English and test the measurement properties of the Brazilian-Portuguese version.
MethodsThe translation and cross-cultural adaptation (from Dutch to Brazilian-Portuguese and English) followed six steps. Interviews were conducted in 33 Brazilian children and adolescents. We also recruited 107 children and adolescents with musculoskeletal pain from schools to test the measurement properties of the Brazilian-Portuguese version. The questionnaire was completed twice with a 7-day interval. Ceiling and floor effects, missing data, internal consistency, reliability, measurement error and construct validity were assessed.
ResultsWe recruited 140 children and adolescents from public and private schools. During the cross-cultural adaptation process, no major difficulty answering and understanding the questionnaire were reported by children and adolescents. The questionnaire did not show ceiling or floor effects and had minimal missing data (0.37%). Internal consistency by the Cronbach's Alpha was 0.69. Test-retest reliability by the Intraclass Correlation Coefficient was 0.75 (95% CI: 0.64, 0.84). The smallest detectable change was 6.5 points out of 18 points. We observed a moderate correlation of 0.54 (p<0.01) with the Spence Children's Anxiety Scale, consistent with our a-priori hypothesis.
ConclusionThe Brazilian-Portuguese version of the Psychosomatic Questionnaire for Children and Adolescents has acceptable measurement properties and is a good option for assessing psychosomatic symptoms in clinical practice and research.
Musculoskeletal pain is common in children and adolescents with prevalence ranging from 4 to 40%.1,2 This represents an important disability burden in this population. According to the Global Burden of Disease Study, back and neck pain ranks 5th in terms of years lived with disability in children aged 10 to 19 years old.3 Musculoskeletal pain in this population can also have important impacts such as school absenteeism and negative effects on physical and social activities.4 In addition, pain in children and adolescents may lead to development of persistent pain in adulthood.5-7
Musculoskeletal pain is associated with psychosomatic factors (e.g., headache, stress, sleep problems),8,9 which can be defined as physical symptoms that arise from or are influenced by the mind and emotions rather than a specific anatomical cause.10 Conceptually, this differs from psychological aspects, which relate to the mental state only. Sleep problems are also highly associated with musculoskeletal pain onset and persistent musculoskeletal pain in children and adolescents.11,12 A better understanding of psychosomatic factors is important to improve knowledge and design clinical strategies for musculoskeletal pain in children and adolescents.
Psychosomatic symptoms is a subjective construct and should be assessed by Patient Reported Outcomes Measures (PROMs).13 There are few PROMs suitable for children and adolescents available to measure psychosomatic symptoms.14-16 In Brazil, the only translated, cross-culturally adapted, and validated instrument aimed at measuring psychosomatic symptoms is the Spence Children's Anxiety Scale (SCAS-Brazil).17 The SCAS-Brazil specifically measures anxiety symptoms17,18 with some items on physical symptoms such as stomach ache, tachycardia, and tremor. However, given the broader determinants and impacts of musculoskeletal pain, scales that measure other psychosomatic symptoms are needed.8
Although some questionnaires are available to measure psychosomatic symptoms, most of them are lengthy, and measure only physical or psychological symptoms.18-21 The Psychosomatic Questionnaire for Children and Adolescents was developed to measure psychosomatic symptoms generally,22 and has nine items. Its brevity and face validity support applicability in clinical and research.22 The Psychosomatic Questionnaire for Children and Adolescents was specifically developed for children and adolescents and was used in previous studies with this population.9,23 In this study we aim to: (1) translate, and cross-culturally adapt the Psychosomatic Questionnaire for Children and Adolescents to both Brazilian-Portuguese and English22 and 2) measure ceiling and floor effects, rate of missing data, and measurement properties in Brazilian children and adolescents with musculoskeletal pain (Brazilian-Portuguese version).
MethodsStudy designThe methods of this study were based on the taxonomy, terminology, and definitions of measurement properties of the COnsensus-based Standards for the selection of health status Measurement INstruments (COSMIN)24 and was conducted in two steps. First, we translated and cross-culturally adapted the Psychosomatic Questionnaire for Children and Adolescents22 from Dutch into Brazilian-Portuguese and also English. Second, we tested the ceiling and floor effects, rate of missing data, measurement properties related to reliability (internal consistency, test-retest reliability, and measurement error) and construct validity of the Brazilian-Portuguese version.
This study was approved by the Human Ethics Committee of Universidade Cidade de São Paulo (UNICID), São Paulo, SP, Brazil (CAAE: 18,752,219.0000.0064) and was conducted in accordance with the Declaration of Helsinki and human's rights.
Participants and proceduresWe recruited children and adolescents aged 8–18 years old with disabling musculoskeletal pain. We chose musculoskeletal pain because it is associated with psychosomatic symptoms.8,9 Participants had to be able to read and understand Brazilian-Portuguese and were recruited from six public and private schools in three cities (Sao Paulo, Itu, and Salto) in Sao Paulo state in Brazil. Itu and Salto are cities with 100,000 to 175,500 residents and Sao Paulo is the most populous city in Brazil with a population of 12.3 million.25 Musculoskeletal pain that impacts daily life was considered as any pain with musculoskeletal origin that interfered with normal (everyday) activities, physical activities, or that caused school absence. A participant was considered to have disabling musculoskeletal pain if they answered “yes” to the question “Did you feel some pain in your back, neck, arms (including hands), or legs (including feet) in the last month?” and “yes” to at least one of the questions: i) “Did you miss school due to pain in your back, neck, arms, or legs in the last month?”, ii) “Has your pain in your back, neck, arms, or legs interfered with your normal activities in the past month?” or iii) “Does your pain in your back, neck, arms, or legs interfered with your recreational activities (e.g., sport, walking, cycling, etc.) in the last month?”.4 Children and adolescents with pain due to surgery or any other specific pathology (e.g., cancer, infection, fracture, inflammatory diseases) were excluded.
Participants were included in the study after parents or guardians signed the consent form. Children and adolescents were also invited to sign the assent form. The questionnaire was completed in the classroom, during school period, by all children and adolescents. Children and adolescents answered the questionnaire by themselves and could ask questions about interpretation to their teachers. Data collection was undertaken during March 2020 to July 2021. Children and adolescents completed the questionnaire on two occasions with a 7-day interval to test the reliability and measurement error of the instrument.
Instruments- •
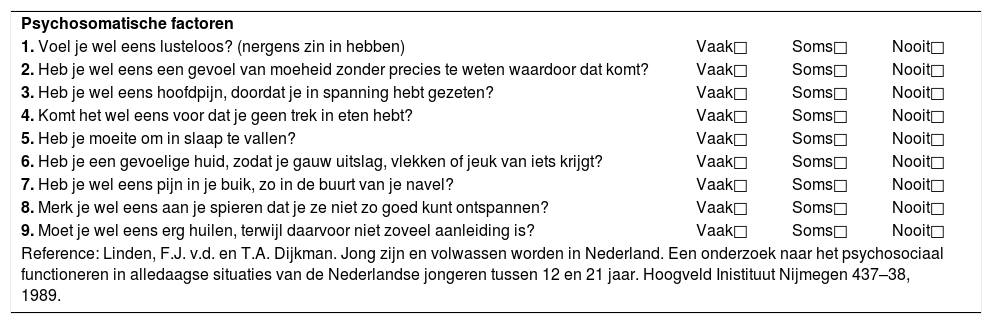
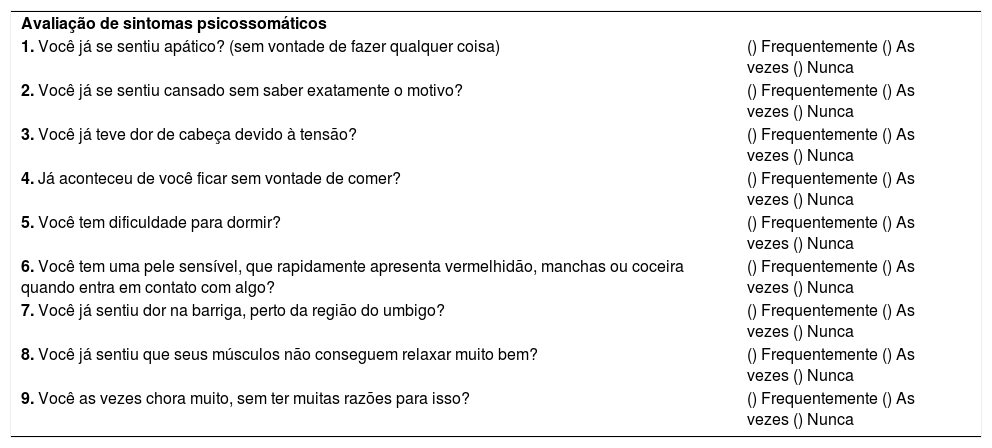
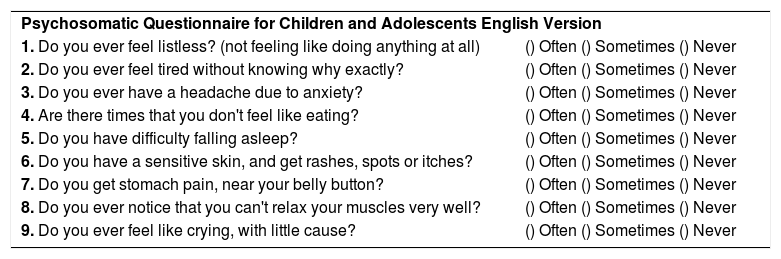
Psychosomatic Questionnaire for Children and Adolescents: The questionnaire was developed by Van der Linden and Dijkman22 in Dutch. The Psychosomatic Questionnaire for Children and Adolescents includes questions on: 1) feeling listless, 2) feeling tired, 3) headache, 4) lack of appetite, 5) sleep disturbance, 6) skin sensitivity, 7) stomach ache, 8) muscle tension, and 9) crying without a specific reason. The nine items are scored as: often (2 points); sometimes (1 point); never (0 points). The total score ranges from 0 (never for all items) to 18 (often for all items) points, higher scores mean higher negative psychosomatic symptoms (Appendix A). The questionnaire has been previously tested in 500 adolescents and younger adults, with a Cronbach's Alpha of 0.57 and has a unidimensional construct. This questionnaire was also used in a previous study9 to investigate the association between neck and/or shoulder and back pain complaints and the weight of schoolbags and other physical and psychological factors in young adolescents.
- •
SCAS-Brazil: The SCAS-Brazil measures anxiety through 44 items. Of these, 38 measure specific symptoms of anxiety, grouped in seven subscales: separation anxiety (6 items), social phobia (6 items), obsessive-compulsive disorder (6 items), panic (6 items), agoraphobia (6 items), generalized anxiety (6 items), and fear of physical injury (5 items). Six items of the questionnaire are positively rated to reduce bias of negative responses. There is also an open-ended question to allow the respondent to report any other fear not otherwise cited. Response options to each question are; never (0 points), sometimes (1 point), often (2 points), and always (3 points). The total score ranges from 0 to 114 points and the higher scores mean higher anxiety level.17 The SCAS-Brazil17,18 has adequate internal consistency, with Cronbach's Alpha coefficient of 0.88.18
We expected that the SCAS-Brazil would have a moderate to strong correlation (r ≥ 0.50) with the Psychosomatic Questionnaire for Children and Adolescents because anxiety is one domain of psychosomatic symptoms.26,27 According to the COSMIN recommendations, instruments measuring similar constructs should have a correlation ≥ 0.50.28
Translation and cross-cultural adaptationWe translated and cross-culturally adapted the Psychosomatic Questionnaire for Children and Adolescents following the Guidelines by Beaton et al. for the Process of Cross-cultural Adaptation of Self-Report Measures.29 Translation and cross-cultural adaptation for the Brazilian-Portuguese and English versions involved six independent steps29:
- 1.
Initial translation of the Psychosomatic Questionnaire for Children and Adolescents from Dutch to Brazilian-Portuguese and English by two independent translators (two with first language Portuguese and two with first language English, all researchers fluent in Dutch);
- 2.
Consensus of both translators from step 1;
- 3.
Back-translation of the questionnaire from Brazilian-Portuguese and English to Dutch by two independent back-translators (with first language in Dutch) – translators did not have previous knowledge of the study objectives or previous knowledge of the instrument;
- 4.
Consensus of both back-translators from step 3;
- 5.
A committee of experts (i.e., researchers and language professionals) revised and reached consensus on the final version of both the Brazilian-Portuguese and English questionnaires taking into consideration its original version, the translated version, and the back-translated version;
- 6.
The translation and adaptation process finished with pilot data collection to identify any difficulty in answering and understanding the questionnaire and to test the distribution of responses (by ceiling and floor effects), and the rate of missing data in 33 children and adolescents. During the interview process children and adolescents were asked about: 1) their understanding of the questions and 2) if they had any difficulty while answering the questionnaire. We also asked if children and adolescents had any difficulty to understand any item, word, or meaning of the questions. This step was conducted only for the Brazilian-Portuguese version, and further studies should test the pre-final version of the English version in a population of children and adolescents’ English speakers.
We calculated the following measurement properties:
- •
Reliability: whether repeated measurements (test-retest) in stable individuals (who are not expected to have any change in their condition) present similar scores.30 According to the COSMIN, reproducibility comprises three different metrics24:
- •
Internal consistency: whether the items of an instrument (or sub-scale) are inter-correlated (homogeneous), i.e., the items of an instrument measure the same construct30,31;
- •
Reliability: whether the proportion of total variance is due to “true” differences between participants30,32;
- •
Measurement error: it is the systematic and random error of participant's scores that is not related to true differences in the construct24,30,32;
- •
- •
Construct validity: the degree to which a test measures what it is supposed to measure, usually comparing the total score of a specific instrument with another similar (convergent validity) or different instrument (divergent validity).33 The result of this comparison needs to be consistent with a priori hypothesis of the relationship.30,32 We used only convergent validity to estimate the relationship between two related instruments (Psychosomatic Questionnaire for Children and Adolescents and Spence Children's Anxiety Scale (SCAS-Brazil)).33
- •
Ceiling and floor effects: the proportion of individuals who get the maximum or minimum score from a questionnaire, respectively.24,34
We used descriptive analysis to summarize the characteristics of the sample. For continuous variable (age) we used mean ± standard deviation (SD) and for categorical variables (school year) we used absolute frequencies and percentage. The distribution was evaluated through visual inspection of histogram.
Ceiling and floor effects were defined as the percentage of individuals who scored the maximum or the minimum score on the questionnaire. Ceiling or floor effects are potentially present when this percentage is 15% or more.30 Rate of missing data was measured by the proportion of missing data related to total possible items to be answered. Internal consistency was measured using Cronbach's Alpha coefficient. This coefficient ranges from zero to 1, scores between 0.70 and 0.95 are considered appropriate.30,31 Reliability was measured using Intraclass Correlation Coefficients (ICC) (Two-way mixed effects, absolute agreement, single rater/measurement) and their respective 95% confidence interval (CI).35 ICC is interpreted as follows: <0.40 – low reliability; 0.40–0.75 – moderate reliability; 0.75–0.90 – substantial reliability; and >0.90 – excellent reliability.32
Measurement error was measured by the Standard Error of Measurement (SEM), calculated by square root of error variance from ANOVA within group analyses.30,36 The smallest detectable change (SDC) was calculated with the formula SDC= 1.96√2SEM. The ratio between the SEM and the total score of the questionnaire was used to classify agreement: ≤5% - very good agreement; >5% and ≤ 10% - good agreement; >10% and ≤20% - doubtful agreement; and >20% - negative agreement.30,32 Reliability (reliability and measurement error) was tested over a 7-day interval. Reliability related to reliability and measurement error was conducted in two situations, in the complete sample size and in the sample containing only the stable participants – self-reported disabling musculoskeletal pain in baseline and follow-up.
Construct validity was measured through a Pearson correlation (r) between final scores of psychosomatic questionnaire and the SCAS-Brazil.37 Pearson correlation (r) is interpreted as follows: ≥ 0.70 – strong convergence; 0.50 to 0.69 – moderate convergence; 0.20 to 0.40 – moderate divergence; and ≤ 0.20 strong divergence.26,27 We hypothesized that scores on the questionnaires would have a positive, moderate to strong convergent correlation; r ≥ 0.50.26,27 All analysis was performed through SPSS statistical package (version 20).
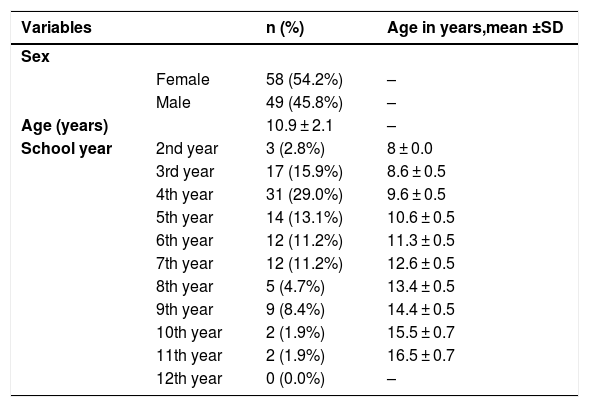
ResultsWe screened 618 children and adolescents from public and private schools, of which 107 self-reported disabling musculoskeletal pain and were included in this study (Fig. 1). Table 1 shows the characteristics of the 107 included children and adolescents. Fifty-four percent of the participants were girls, mean age was 10.9 ± 2.1 years, and the highest proportion of participants were in the fourth year of elementary school (29%). We also collected data on 33 children and adolescents for the interviews with mean age of 11.3 ± 1.8 years.

Characteristics of 107 children and adolescents included in the study.
SD: standard deviation.
n (%): absolute number and percentage.
During the translation and cross-cultural adaptation, only one change was necessary. For item 6 of the instrument, the committee of experts judged that the term “uitslag” (rash) was a complex term for children and adolescents, so the term “redness” was used in the translated version (Appendices B and C).
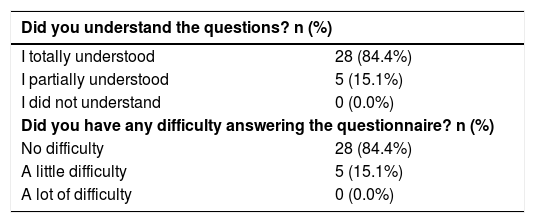
The interviews (step 6) to test the pre-final version were only performed with the Brazilian-Portuguese version. Table 2 shows the answers from children and adolescents for the interviews, around 85% of participants had no troubles with the questionnaire. One child reported difficulty understanding item 5 and another child had difficulty understanding the word “apathetic.” Only 1 (0.9%) child scored the minimum possible score on the questionnaire. No ceiling and floor effects were observed (Fig. 2) and there was minimal missing data (0.37%).
Reliability
We observed slightly lower than acceptable levels of internal consistency, substantial levels of reliability, and high levels of measurement error, in all participants and in the subsample of stable participants (post-hoc analysis). Table 3 shows all these results.
Reliability of questionnaire.
ICC: Intraclass Correlation Coefficients.
CI: Confidence Interval.
SEM: Standard Error of Measurement.
SDC: Smallest Detectable Change.
There was a moderate, positive correlation of 0.54 (p<0.01) between the Psychosomatic Questionnaire for Children and Adolescents and the SCAS-Brazil.
DiscussionThe Brazilian-Portuguese version of the Psychosomatic Questionnaire for Children and Adolescents adequately measures psychosomatic symptoms in children and adolescents with disabling musculoskeletal pain. The process of translation and cross-cultural adaptation to Brazilian-Portuguese produced a version with minimal changes necessary from the original version. While an English version of The Psychosomatic Questionnaire for Children and Adolescents was provided in this study, we did not test its measurement properties in English-speaking children and adolescents.
The Brazilian-Portuguese version of questionnaire did not show ceiling and floor effects and had a minimal rate of missing data. Reliability was substantial and construct validity adequate, however internal consistency was slightly less than expected and there were high levels of measurement error. The high levels of measurement error (SDC of 6.48) is a limitation of this questionnaire. It is necessary caution to use the questionnaire to measure change scores in clinical trials as it would require a change of 6.48 out of 18 points to identify changes in the construct. However, the Psychosomatic Questionnaire for Children and Adolescents showed adequate construct validity in accordance with our prior hypothesis.
The Psychosomatic Questionnaire for Children and Adolescents had their measurement properties previously tested by the original authors (Dutch version).22 They have tested the internal consistency and the structural validity of the questionnaire. The authors found the questionnaire to be unidimensional and with internal consistency of 0.57 by the Cronbach Alpha.22 The internal consistency found in this study is higher than the original testing (0.69), and indicates that items of the questionnaire are not strongly inter-related.9,22 In Brazilian-Portuguese, the SCAS-Brazil is available, and it has been reported with an internal consistency of 0.88 in Brazilian children and adolescents.18 The authors found a higher internal consistency compared to our study probably because the SCAS-Brazil only measure symptoms of anxiety, instead of all psychosomatic symptoms.18
We believe the questionnaire can measure psychosomatic symptoms in clinical practice. The substantial reliability of the Psychosomatic Questionnaire for Children and Adolescents means that the proportion of the total variance in the measurements is explained by ‘true’ differences between patients. Although this questionnaire was tested broadly in children and adolescents with musculoskeletal pain, we recommend caution for extrapolating the findings to other conditions, such as Juvenile Idiopathic Arthritis and pediatric fibromyalgia.23 We do not know if the measurement properties would be acceptable in different conditions.
The questionnaire had its measurement properties tested based on the taxonomy, terminology, and definitions of COSMIN recommendations.24 Another strength is that the study was done in Sao Paulo state, which is the most populous state in Brazil and a target of great migration flow,38 which suggests good external validity for using the questionnaire in the Brazilian population. Nevertheless, our assessment of construct validity was limited as we tested only one hypothesis and used only convergent validity with one instrument.
Additional studies are needed to confirm our findings. Future studies are necessary to test the pre-final English version of the Psychosomatic Questionnaire. We recommend that more in-depth analyses of this questionnaire should be performed, such as exploratory factor analysis, responsiveness, and further tests of construct validity.
ConclusionThe Brazilian-Portuguese version of the Psychosomatic Questionnaire for Children and Adolescents had adequate construct validity, no ceiling or floor effects and substantial reliability. However, the questionnaire has borderline internal consistency, and high levels of measurement error.
The authors would like to thank to São Paulo Research Foundation (FAPESP-Brazil) for all financial grant support and to Universidade Cidade de São Paulo (UNICID) for all resources and structure to conduct this study. This study is supported by the Sao Paulo Research Foundation (FAPESP 2017/17484–1); Dr Yamato is supported by the Sao Paulo Research Foundation (FAPESP 2019/10330–4); Ms Souza holds a PhD scholarship from the Sao Paulo Research Foundation (FAPESP 2019/12049–0); and, Ms Leite holds a PhD scholarship from the Sao Paulo Research Foundation (FAPESP 2020/03629–0).
Psychosomatic Questionnaire for Children and Adolescents Original version
Psychosomatic Questionnaire for Children and Adolescents Brazilian-Portuguese Version
Psychosomatic Questionnaire for Children and Adolescents English Version



