



Scales to assess the quality of life and return-to-sport after reconstruction of the anterior cruciate ligament (ACL) may help the clinical decision-making process.
ObjectiveTo cross-culturally adapt and determine the validity of the Brazilian versions of the Anterior Cruciate Ligament Return to Sport after Injury (ACL-RSI) and the Quality of Life Questionnaire (ACL-QoL).
MethodsThe process of translation and cross-cultural adaptation followed the recommendations of international guidelines. One hundred participants filled out the Brazilian versions of these instruments, the Tampa Scale for Kinesiophobia (TSK), the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, and the 36-Item Short Form Health Survey (SF-36). The measurement properties of reliability, internal consistency and construct validity were measured.
ResultsThe ACL-RSI and the ACL-QoL were successfully translated and cross-culturally adapted. Both questionnaires showed good test–retest reliability (ICC2,1=0.78, 95% CI=0.67–0.85 for the ACL-RSI; and ICC2,1=0.84, 95% CI=0.76–0.90 for the ACL-QoL) and good internal consistency (Cronbach's alpha=0.87 for the ACL-RSI; and Cronbach's alpha=0.96 for the ACL-QoL). A reasonable correlation was found between both questionnaires and the TSK, and a low to reasonable correlation was found between the questionnaires and the SF-36 in terms of validity. Compared to the IKDC Subjective Knee Evaluation Form, the ACL-RSI had a reasonable correlation and the ACL-QoL had a good correlation.
ConclusionThe Brazilian versions of the ACL-RSI and the ACL-QoL have adequate measurement properties and may be used in assessing Brazilians after ACL reconstruction.
Anterior cruciate ligament (ACL) injuries are typically severe and occur mainly during sports practices involving contact, jumps, and pivot movements.1 These are common orthopedic injuries, with an annual incidence of 68.6 per 100,000 people.2 It is estimated that in the United States there are approximately 200,000 cases annually,3 of which a high percentage require surgical reconstruction to restore the functional stability of the knee, thus allowing the resumption of recreational and sports activities.3,4
Although one of the main objectives of ACL reconstruction surgery is to make it possible for patients to return to sport and perform at the pre-injury level, a high percentage does not reach that goal.5–8 A systematic review8 revealed that 81% of individuals who sustained an ACL injury returned to sports, but only 65% performed at the pre-injury level and only 55% reached the competitive level. The reasons for this are multifactorial and may include issues relating to the surgery and rehabilitation that have repercussions in terms of physical function and demographic, social, or psychological factors, such as fear, anxiety, and self-confidence.8 The latter reasons are often neglected. Several studies have investigated the function of the knee after ACL reconstruction, but few have reported the psychological impact upon returning to sports after surgery.9–11
Another aspect of ACL injury is related to quality of life (QoL). A recent systematic review with meta-analysis showed that ACL-deficient individuals have impaired QoL compared to the normal population and that there is no difference between the QoL of individuals who are chronically ACL-deficient and those who have undergone surgical reconstruction.12 Therefore, scales capable of evaluating the QoL of patients with ACL injuries and the psychological factors involved in the return to sport after reconstruction surgery can facilitate clinical decision making for each patient.
The Scale to Measure the Psychological Impact of Returning to Sport After Anterior Cruciate Ligament Reconstruction Surgery (ACL-RSI) is a self-report scale containing 12 items subdivided into 3 domains: emotions, performance and risk assessment.10 The Quality of Life Outcome Measure (Questionnaire) for Chronic Anterior Cruciate Ligament Deficiency (ACL-QoL) is an instrument developed with the objective of evaluating the quality of life of patients with chronic injury ACL and it contains 31 items that are subdivided into 5 domains: Symptoms and Physical Complaints, Work-Related Concerns, Recreation Activities and Sport Participation or Competition, Life Style and Social and Emotional Aspects.13 Both instruments have been translated, adapted and have their measurement properties tested into several languages14–18 and have shown to have good reliability and responsiveness, but there are no versions adapted into Brazilian–Portuguese. Therefore, the objectives of this study were the translation and cross-cultural adaptation of these tools and the verification of their validity and reliability.
MethodsStudy designThis study was divided into two stages. In the first, the translation and cross-cultural adaptation of the ACL-RSI and the ACL-QoL were performed. In the second stage, the measurement properties of both instruments were verified, following a longitudinal prospective study model.
The study was conducted at the Laboratory of Analysis of Human Movement at the Universidade Federal do Ceará (UFC), Fortaleza, CE, Brazil, between November 2014 and June 2016.
The sample consisted of 100 participants with ACL injuries who underwent reconstructive surgery at least three months prior to the study and who practiced some sporting modality. The sample size was determined according to Terwee et al.,19,20 which suggests that at least 50 patients are required for an appropriate analysis of construct validity, reproducibility and ceiling and floor effects, and a minimum of 100 patients to analyze the internal consistency.
We included those aged 16–50 who had unilateral lesions of the ACL and excluded those with grade 3 collateral ligament injuries, bilateral rupture of the ACL, and posterior cruciate ligament injuries.
This study was approved by the Research Ethics Committee of the UFC (Protocol Number: 838.253). All participants were educated about the procedures and gave informed consent to participate in the study. All participants had the right to withdraw at any time.
Translation and cross-cultural adaptation procedureThe process of translation and cross-cultural adaptation of the ACL-RSI and ACL-QoL tools for Brazilian Portuguese was authorized by the authors of the original questionnaires and followed the pre-established recommendations of international guidelines.21,22 The ACL-RSI and ACL-QoL were translated from English into Brazilian Portuguese by two native translators fluent in English; one is a professional in the health field with experience in traumatology and orthopedics and the other is a professional translator. The translations were discussed by the translators and the authors of the study, and first drafts were agreed upon. These versions were translated into English by two native-speaking professional translators with no prior knowledge of the original versions. The translations, back-translations, and original versions were reviewed by a committee of experts to establish a consensus. These versions were administered to 30 subjects with ACL injuries to determine any difficulties in understanding the items (uncertainties reported by 20% or more of the sample indicate the need for revision of the questionnaire). Thus, third and final versions were obtained.
Assessment of the measurement propertiesTest–retest reliability and agreementAll subjects were evaluated at the first clinic visit and after 5–8 days. This range was chosen to minimize the likelihood of significant changes in the clinical condition of the patient and to minimize the likelihood of patients memorizing the answers.
The test–retest reliability was tested using the intraclass correlation coefficient (ICC2,1). Values lower than 0.69 indicated poor reliability; values between 0.70 and 0.79 were considered acceptable; values between 0.80 and 0.89 indicated good reliability and from 0.90 to 1.0 excellent reliability.23
We used two measures of agreement: Standard Error of the Measurement (SEM) and Smallest Detectable Change (SDC). The SEM was calculated by multiplying the standard deviation of the mean differences between the two measurements by the square root of 1 minus ICC (SD differences*√1−ICC) and the SDC was calculated using the formula SDC=1.96×√2×SEM. The SEM reflects the absolute error of the instrument and the SDC reflects the smallest within person change in a score that can be interpreted as a “real” change, above the measurement error one of an individual.
The ratio between the SEM and the total score of the instrument was used to indicate agreement as follows: less than or equal to 5%, very good agreement; greater than 5% and 10% or less, good agreement; greater than 10% and 20% or less, doubtful agreement; and greater than 20%, negative agreement.
Internal consistencyInternal consistency was measured using the Cronbach's alpha. An alpha value between 0.70 and 0.90 was considered good and greater than 0.90 was considered excellent.19
Construct validityThe ACL-RSI contains 12 items subdivided into 3 domains: emotions, performance and risk assessment.10 All items are scored by superimposing a 20-point grid over the line. Values are assigned in increments of 5 ranging from 0 to 100. A value of 0 indicate extremely negative psychological responses whilst a value of 100 represent no negative psychological responses.10
The ACL-QoL contains 31 questions that are subdivided into 5 domains: Symptoms and Physical Complaints, Work-Related Concerns, Recreation Activities and Sport Participation or Competition, Life Style and Social and Emotional Aspects.13 The final score ranges from 0 to 100 points, and the higher the score the better the quality of life.
The instruments used to test the validity of the Brazilian versions of ACL-RSI and ACL-QoL were the Tampa Scale for Kinesiophobia (TSK), the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, and the Short Form (36) Health Survey (SF-36).
Tampa Scale for Kinesiophobia (TSK) consists of a self-administered questionnaire, composed of 17 questions that address the pain and intensity of symptoms. The final score ranges from 17 to 68 points, and the higher the score the higher the degree of kinesiophobia.24
The Subjective Knee Evaluation Form (IKDC) is an instrument composed of 10 items that are divided into three domains: symptoms, sports activities and function.25 The final score is calculated by summing the scores for individual items and then transformed to a scale that ranges from 18 to 100. The higher score indicate no limitation with activities of daily living or sports activities and the absence of symptoms.25
The Short Form (36) Health Survey (SF-36) includes 36 items that are combined in 8 subscales: functional capacity, physical aspects, pain, general health, vitality, social aspects, emotional aspects and mental health. The score ranges from 0 (worst possible) to 100 (best possible) and is independently produced in each subscale.26
The construct validity was determined by testing the following pre-defined hypotheses involving correlations between the ACL-RSI and ACL-QoL and questionnaires used to assess similar constructs:
- (1)
Patients who obtain higher scores on the ACL-RSI have lower scores on TSK.
- (2)
Patients with higher scores on the ACL-RSI will score higher on the ACL-QoL.
- (3)
There is a positive correlation between ACL-QoL and the SF-36.
- (4)
There is a positive correlation between ACL-RSI, ACL-QoL, and the IKDC Subjective Knee Evaluation Form.
The construct validity was determined using a Spearman correlation. A correlation coefficient greater than 0.90 was considered excellent; between 0.71 and 0.90 was considered good; between 0.51 and 0.70 was considered reasonable; between 0.31 and 0.50 was considered weak; and less than or equal to 0.30 was considered low.27
Ceiling and floor effectsCeiling and floor effects refer to content validity, and their presence indicates that extreme items are missing in the scales. The percentages of responders who scored the lowest or highest in each separate subscale were documented. Ceiling and floor effects for an entire questionnaire are considered to be present if more than 15% of respondents score the lowest or highest possible score.19
ResultsTranslation and cross-cultural adaptationThe translations of ACL-RSI and ACL-QoL from English to Portuguese underwent no significant changes. In the ACL-QoL, the terms “giving way” and “stiffness” were translated into Portuguese as “falseio” and “rigidez” or “travamento”, respectively. The expression “working in the yard” in question 21 was replaced with “cuidar da casa” (“working in the house”), given that “working in the yard” is not a common activity in Brazil. In question 25, the expression “lifestyle activities” was translated as “atividades diárias” (“daily activities”), and the word “troubled” in question 30 was replaced with “incomodado” (“bothered”) to facilitate understanding of the question. The categories “Complaints related to work” and “Lifestyle” were restructured for better understanding.
To facilitate the choice response, we used an 11-point Likert scale in the form of check boxes. The score was graded from 0 to 10 rather than from 0 to 100, as in the original questionnaires. On the original version of ACL-RSI, Descriptors “extremely” and “not at all”, representing opposite ends of the question continuum, were placed at either end of the scale. To facilitate understanding, the score of the Brazilian version was standardized, with the minimum score equating to the answer “De modo nenhum” (“Not at all”) and the maximum score equating to “Extremamente” (“Extremely”).
The final score of the questionnaire was not affected, given that it presents six questions that highlight positive aspects and six questions that highlight negative aspects, nullifying the score. Therefore, it was necessary that the score for questions 2, 3, 6, 7, 9, and 10 of the Brazilian version were inverted.
All these modifications were performed prior to pretesting with 30 participants. Less than 20% of the participants demonstrated difficulties in understanding the instruments, no further indicated the need for revision.
Study participantsThe study included 100 participants comprising 82 males and 18 females. The mean age was 27.08 years (SD=6), the average weight was 80.1kg (SD=11), and the average height was 1.71m (SD=0.74). The minimum time after surgery among the participants was three months and the maximum was 12 years. The most popular sport among the participants was soccer (52%). Only 45% of the sample returned to the sport, and of those, only 17.7% reported to have returned to the same level as before the injury.
Reliability, internal consistency, construct validity, and ceiling and floor effectsThe intraclass correlation coefficient (ICC2,1) was considered good for the ACL-RSI (ICC2,1=0.78, 95% CI=0.67–0.85) and the ACL-QoL (ICC2,1=0.84, 95% CI=0.76–0.90), demonstrating good test-retesting reliability for both assessment tools (Table 1). The SEM and SDC values are presented in Table 1.
Test–retest reliability of the components of ACL-RSI and ACL-QoL.
| Instruments | ICC* | 95% CI | SEM | SDC | |
|---|---|---|---|---|---|
| Lower | Higher | ||||
| ACL-RSI | 0.78 | 0.67 | 0.85 | 6.5 | 18.1 |
| Overall ACL-QoL | 0.84 | 0.76 | 0.90 | 4.7 | 13.2 |
| QoL-symptoms | 0.66 | 0.51 | 0.77 | 10.4 | 28.9 |
| QoL-work | 0.82 | 0.72 | 0.89 | 6.7 | 18.6 |
| QoL-participation | 0.82 | 0.73 | 0.88 | 6.7 | 18.5 |
| QoL-lifestyle | 0.70 | 0.56 | 0.80 | 9.6 | 26.6 |
| QoL-social and emotional concerns | 0.83 | 0.74 | 0.89 | 6.4 | 17.7 |
Abbreviations: ACL-RSI, Anterior Cruciate Ligament-Return to Sport After Injury; ACL-QoL, Quality of Life Anterior Cruciate Ligament Questionnaire; QoL, quality of life; ICC, intraclass correlation coefficient; CI, confidence interval; SEM, standard errors of the measurement; SDC, smallest detectable change.
Based on the correlation strength among the 12 items, the internal consistency of the ACL-RSI was considered good with a Cronbach's alpha of 0.87 (Table 2). The Cronbach's alpha for the ACL-QoL was 0.96, showing a strong correlation between items. The results of the questionnaire for subdomains ranged from 0.83 to 0.95 (Table 2). The high alpha values found for both questionnaires showed good consistency, indicating the reliability of the data obtained.
Internal consistency of the components of ACL-RSI and ACL-QoL.
| Instruments | Cronbach's α |
|---|---|
| RSI-overall | 0.87 |
| QoL-overall | 0.96 |
| QoL-symptoms | 0.83 |
| QoL-work | 0.86 |
| QoL-participation | 0.95 |
| QoL-lifestyle issues | 0.86 |
| QoL-social and emotional concerns | 0.86 |
Abbreviations: ACL-RSI, Anterior Cruciate Ligament-Return to Sport After Injury; ACL-QoL, Quality of Life Anterior Cruciate Ligament Questionnaire; RSI, Return to Sport After Injury; QoL, quality of life.
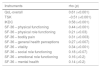
All correlation coefficients showing comparisons between the ACL-RSI, the TSK scale, the IKDC Subjective Knee Evaluation Form, and the SF-36 are shown in Table 3. The correlation coefficients between these questionnaires and the overall score and ACL-QoL domains are shown in Table 4.
ACL-RSI correlation with the results of instruments with similar constructs.
| Instruments | rho (p) |
|---|---|
| QoL-overall | 0.61 (<0.001) |
| TSK | −0.51 (<0.001) |
| IKDC | 0.58 (<0.001) |
| SF-36 – physical functioning | 0.44 (<0.001) |
| SF-36 – physical role functioning | 0.21 (<0.03) |
| SF-36 – bodily pain | 0.31 (<0.003) |
| SF-36 – general health perceptions | 0.27 (<0.007) |
| SF-36 – vitality | 0.34 (<0.001) |
| SF-36 – social role functioning | 0.18 (<0.07) |
| SF-36 – emotional role functioning | 0.16 (<0.2) |
| SF-36 – mental health | 0.14 (<0.2) |
Abbreviations: ACL-RSI, Anterior Cruciate Ligament-Return to Sport After Injury; QoL, quality of life; TSK, Tampa Scale for Kinesiophobia; IKDC, International Knee Documentation Committee; SF-36, Medical Outcomes Study 36-Item Short-Form Health.
ACL-QoL correlation with the results of instruments with similar constructs.
| Instruments | Overall rho (p) | Symptoms rho (p) | Work rho (p) | Participation rho (p) | Lifestyle rho (p) | Social and emotional rho (p) |
|---|---|---|---|---|---|---|
| SF-36 – physical functioning | 0.64 (0.001) | 0.48 (0.001) | 0.54 (0.001) | 0.54 (0.001) | 0.58 (0.001) | 0.54 (0.001) |
| SF-36 – physical role | 0.48 (0.001) | 0.31 (0.003) | 0.48 (0.001) | 0.40 (0.001) | 0.47 (0.001) | 0.46 (0.001) |
| SF-36 – bodily pain | 0.47 (0.001) | 0.38 (0.001) | 0.61 (0.001) | 0.37 (0.001) | 0.43 (0.001) | 0.43 (0.001) |
| SF-36 – general health | 0.24 (0.020) | 0.30 (0.003) | 0.13 (0.200) | 0.14 (0.200) | 0.24 (0.020) | 0.29 (0.004) |
| SF-36 – vitality | 0.29 (0.004) | 0.25 (0.020) | 0.19 (0.07) | 0.29 (0.004) | 0.33 (0.002) | 0.24 (0.020) |
| SF-36 – social role | 0.28 (0.005) | 0.20 (0.050) | 0.24 (0.030) | 0.21 (0.040) | 0.29 (0.004) | 0.34 (0.001) |
| SF-36 – emotional role | 0.47 (0.001) | 0.26 (0.009) | 0.44 (0.001) | 0.41 (0.001) | 0.44 (0.001) | 0.46 (0.001) |
| SF-36 – mental health | 0.20 (0.05) | 0.01 (0.95) | 0.16 (0.2) | 0.20 (0.05) | 0.18 (0.07) | 0.26 (0.01) |
| TSK | −0.57 (0.001) | −0.40 (0.001) | −0.41 (0.001) | −0.55 (0.001) | −0.52 (0.001) | −0.59 (0.001) |
| IKDC | 0.73 (0.001) | 0.65 (0.001) | 0.63 (0.001) | 0.67 (0.001) | 0.63 (0.001) | 0.60 (0.001) |
| ACL-RSI | 0.61 (0.001) | 0.45 (0.001) | 0.31 (0.003) | 0.63 (0.001) | 0.49 (0.001) | 0.57 (0.001) |
Abbreviations: ACL-QoL, Quality of Life Anterior Cruciate Ligament Questionnaire; ACL-RSI, Anterior Cruciate Ligament-Return to Sport After Injury; QoL, quality of life; TSK, Tampa Scale for Kinesiophobia; IKDC, International Knee Documentation Committee; SF-36, Medical Outcomes Study 36-Item Short-Form Health.
All the hypotheses tested in this study were confirmed. Correlations between the ACL-RSI, the TSK (rho=−0.51) and the IKDC Subjective Knee Evaluation Form domains (rho=0.58) were considered reasonable. When compared to the domains of the SF-36, the correlation coefficients were found to be low, ranging between rho=0.14 and rho=0.44.
The correlation coefficient for the ACL-QoL and IKDC Subjective Knee Evaluation Form (rho=0.73) was considered good, and the correlation between the ACL-QoL and TSK (rho=−0.57) was considered reasonable. When compared with the SF-36, the ACL-QoL had reasonable correlation coefficients in relation to the domain Physical Functioning (rho=0.64), weak correlation to the domains Physical Role (rho=0.48), Bodily Pain (rho=0.47) and Emotional Role (rho=0.47), and weak correlation to the domains General Health (rho=0.24), Vitality (rho=0.29), Social Aspects (rho=0.28), and Mental Health (rho=0.20). The correlation between ACL-QoL and ACL-RSI was reasonable (rho=0.61).
There was no ceiling and floor effect for either instrument. This is because less than 15% of the participants were given the lowest or the highest possible score.
DiscussionThe Brazilian versions of ACL-RSI and ACL-QoL proved to be internally consistent, reliable, and valid for patients who underwent reconstruction of the ACL. In relation to the assessment of the measurement properties, the test–retest reliability was analyzed using the ICC and was found to be good for both instruments. Trochim et al.28 stated that reliability tends to be higher when shorter time intervals are used. However, care must be taken so that the time is not short enough to allow the memorization of answers. As the minimum postoperative time for participating in this study was three months, the valuations were made after 5–8 days to minimize the likelihood of significant changes in the clinical condition of the patients. As the number of questionnaire items is high, it was not possible for the answers to be memorized.
In the validation study of the Turkish version of ACL-QoL, the time interval between the evaluation and reassessment was 7–15 days, and the values for the domains were found to be excellent (ICC=0.94–0.98).17 Although limited by the relatively long time between the conclusion of the first and second questionnaire (approximately 40 days), the Swedish version of ACL-RSI showed good reliability, with an ICC=0.89.14
The analysis of internal consistency using the Cronbach's alpha showed that both the ACL-RSI and the ACL-QoL had good consistency between items. In the validation study of the French version of ACL-RSI, the Cronbach's alpha was 0.96,15 while the Swedish14 and Dutch18 versions had a Cronbach's alpha of 0.94. All studies reinforce the strong correlation between the 12 items of the scale, demonstrating that despite being divided into three subdomains (emotions, confidence in the performance, and risk assessment), they are closely interrelated and cannot be scored separately. A recently published study29 found that lack of trust and fear of re-injury are the leading reasons for athletes not to return to sports. Another study30 reported similar results and found that functional deficits are associated with each other. These factors justify the need for an instrument to assess these aspects together. In the validation study of the Turkish version of the ACL-QoL,17 the Cronbach's alpha for this instrument was 0.93, while for the individual areas the values ranged between 0.66 and 0.89. This corroborates the results of the present study and shows the strong relationship between all the items of the questionnaire.
The construct validity was tested through of the correlation between ACL-RSI and ACL-QoL with the TSK, the IKDC Subjective Knee Evaluation Form, and SF-36. In validating the ACL-RSI and ACL-QoL for other languages, most studies14,15,17 used the Knee Injury and Osteoarthritis Outcome Score (KOOS). However, this instrument was not translated into Brazilian Portuguese and was therefore not used in this study.
Regarding the pre-defined hypotheses, it was expected that patients with less psychological impact upon their return to sport would have better QoL scores, demonstrated by increased scores on the ACL-RSI and ACL-QoL, respectively; would have lower scores for the TSK; and would have higher scores on the IKDC Subjective Knee Evaluation Form and the SF-36. For ACL-QoL, all hypotheses tested showed statistically significant correlations. As for the ACL-RSI, except for some domains of the SF-36 (Social Aspects, Emotional Aspects, and Mental Health), all other assumptions showed significant correlations. According to Terwee et al.,19 the recommended level of correlation between the instruments is greater than 0.70; however, lower results are acceptable, considering that similar questionnaires may assess different constructs.
Regarding the comparison of the ACL-RSI with the TSK, the IKDC Subjective Knee Evaluation Form, and the ACL-QoL, the results showed a reasonable correlation coefficient. This can be explained by the fact that these instruments, although they have some similarity in regards to some items, do not specifically evaluate psychological impact upon the return to sport, as does the ACL-RSI.
When compared with the SF-36, the results revealed weak or low correlation coefficients. The domains of Social Aspects, Emotional Aspects, and Mental Health showed no statistically significant correlations. Items relating to these areas assess emotional problems such as anxiety and depression and their consequences in terms of daily activities but not in terms of sports, which explains the lack of correlation with ACL-RSI. A systematic review published in 201431 revealed that in order to assess the QoL after ACL reconstruction using a more specific instrument, such as the KOOS-QoL, the results tend to be more reliable compared to when using generic instruments, such as the SF-36. This study corroborates the results in the Swedish validation of ACL-RSI, which found a correlation coefficient of 0.71 when compared to the KOOS-QoL.14 Whereas the SF-36 is an instrument that evaluates the QoL in broad terms and diverse populations, the ACL-RSI evaluates emotions and confidence in sports performance in a specific population, and the results here can be considered acceptable.
Regarding the comparison of the ACL-QoL and IKDC, the correlation coefficient was considered good. When compared to the TSK scale and the Functional Capacity, Limitation for Physical Aspects, Pain and Emotional Aspect of the SF-36, the results were reasonable, but the correlation was weak for the other domains of the SF-36. The results of the validation of the Turkish version of ACL-QoL were similar. The authors suggest that the specificity of these questionnaires explains the difference in the strength of association between them.17
ConclusionThe Brazilian versions of ACL-RSI and ACL-QoL were shown to be consistent, reliable, and valid. These tools can be used on a large scale to assess the psychological impact and QoL of Brazilians who have undergone surgical reconstruction of the ACL upon their return to sport.
Conflicts of interestThe authors declare no conflicts of interest.
Ethical Committee of Federal University of Ceará number: 838.253.



