
Patient's satisfaction level is considered an indicator that interferes with interventions effectiveness. There is evidence from other health professionals that patients with higher satisfaction level recover faster. However, benefits toward physical therapy intervention is poorly known.
ObjectiveTo measure the inpatient satisfaction level receiving physical therapy care and to evaluate which aspects of these treatments are flawed.
MethodsPatients admitted to hospital were evaluated using MedRisk Instrument for Measuring Patient Satisfaction with Physical Therapy Care (MRPS) that scores from 1 to 5 (higher values indicate higher satisfaction) for each item. Patients clinical and demographic characteristics and the Global Perceived Effect (GPE) were also collected. Exploratory factor analysis was conducted.
Results200 patients were evaluated (50.9±18.81 years, 58% male). Most of MRPS items were above 4. The highest scoring item (4.75) was physical therapist's respect to the patient. The lowest scoring item (1.82) was in relation to physical therapy guidelines at hospital discharge. Mean MRPS total score and GPE were 46.09±4.93 and 2.18±1.18, respectively.
ConclusionThe majority of patients are satisfied and showed improvement after physical therapy treatment. There is the need for advances and intervention in relation to physical therapy guidelines at hospital discharge. MRPS instrument proved to be appropriate to measure inpatient's satisfaction level with physical therapy care.
Patient satisfaction is considered greatly important for health sectors from government to private hospitals. Its importance is not as a health care indicator quality, but also to understand how the therapy can help and increase treatment success.1 It is subjectively related to each individual's sociopsychological state and directly related to patients’ credibility with service provided and how it meets all his or her expectations.2–5
The satisfaction level in health area has been considered an excellent care quality indicator and an essential element that intimately affects treatments potential and effectiveness.1–4 Peiris et al.6 suggested that patient's perception and attitude directly influence rehabilitation outcome process.6
Physical therapy aims to promote early patient recovery and rehabilitation, as well as their independence, autonomy and quality of life.7,8 Reducing patient hospitalization time is a high priority and efficiency indicator, with potentially significant implications for each individual, health service and community.7,8 Currently the patient professional ratio can be highly disproportionate, which is evidenced mainly in public sectors and this fact may have satisfaction level impact.9 It would be necessary that professionals prioritize patients who need more attention and to consider patient's point of view which often results in a compromise on service quality provided.9,10 However, in hospital environment satisfaction level with physical therapy care remains poorly known.
Therefore, the aim of this study is to measure inpatient satisfaction level receiving physical therapy care and to evaluate which aspects of these treatments are flawed.
MethodsParticipantsObservational cross-sectional study was previously approved by Ethics and Research Committee (CAAE 06343112.0.0000.0064) of Universidade Cidade de São Paulo (UNICID), São Paulo, São Paulo, Brazil.
This study was based on a consecutive non-probabilistic convenience sample that it were included patients receiving physical therapy care at tertiary-level school hospital, both sexes, older than 18 years and with preserved cognitive level, from August 2016 to July 2017. Patients who were admitted to intensive care unit, sedated, and/or assessed as having a lower consciousness level were not included.
ProceduresParticipants who agreed to participate signed an informed consent form and were approached prior to hospital discharge. Therefore, there was no researcher interference during physical therapy treatments received by patients.
Patients’ characteristics were collected through an evaluation form with questions regarding demographic data, information about hospitalization sector, and amount of physical therapy sessions received per day.
MedRisk Instrument for Measuring Patient Satisfaction with Physical Therapy Care (MRPS) aims to measure the variables associated with overall patient satisfaction.11–13 Originally, it is an instrument with 20 items11,12 and when it was translated and validated to the Brazilian Portuguese some items were removed from the exploratory and confirmatory analysis. These items did not significantly correlate to global measures due cultural aspects, differences in clinical settings and patient expectation. Therefore the Brazilian Portuguese version of the MRPS has 13 items with a score from 13 to 65 points and it was subdivided into three domains.5,13 The first domain, called interpersonal, contains six items that address therapist-patient relationship and patient's interactions with staff.5,13 The second domain, called convenience and efficiency, is composed of three items.5,13 The third domain, called patient education, includes two items referring to physical therapists’ commitment to raise awareness and educate their patients.5,13 Finally, the instrument consists of two more items: “Overall, I am completely satisfied with the services I received” and “I would return to this clinic for future care” not allocated to specific factors, which are considered global items.5,13 Through a consensus among authors we included four questions from the original instrument (20 items) considered relevant for hospital setting application: “I waited too long to see my therapist”, “My therapist did not spend enough time with me”, “The therapists assistant/aide was respectful” and “My therapist did not listen to my concerns”.
Patients gave their satisfaction level for each item using a Likert scale ranging from 1 (“completely disagree”) to 5 (“completely agree”). In addition, a “not applicable” option is available for some items. Therefore, the higher the score, the greater the patient's satisfaction.11–13
This instrument also presents a Global Perceived Effect (GPE), which measures overall patient's current recovery impression, comparing beginning of treatment with current health condition.5,12,13 This is a 9-point Likert scale ranging from 1 (“very much better”) to 9 (“very much worse”), where lower scores represent patients who are better and higher scores represent those who worsen after initiating treatment in comparison to onset of their symptoms.5,13
Statistical analysisData processing and analysis were performed using SPSS statistical program version 19.0 for Windows (IBM SPSS Inc., Chiacago, IL) and a 0.05 statistical significance was considered. Patients’ characteristics were submitted to descriptive analysis. Continuous variables with normal distribution were summarized by mean and standard deviation and categorical variables by frequency and proportion.
For evaluation and to explore how the patients understand MRPS items, factorial exploratory analysis14,15 was performed, considering four extra items from original instrument and excluding the “not applicable” item. Principal component analysis with varimax rotation was performed.14,15 This approach was used to test potential factor total, confirmed by visual hit Chart14,15 inflection point inspection. Item allocation for each factor was performed by inspecting component matrix and rotating load Charts.14,15 Items that loaded high on a factor in component matrix and were visually grouped together were allocated to that factor.14,15 Factors were named by evaluation and synthesis.14,15
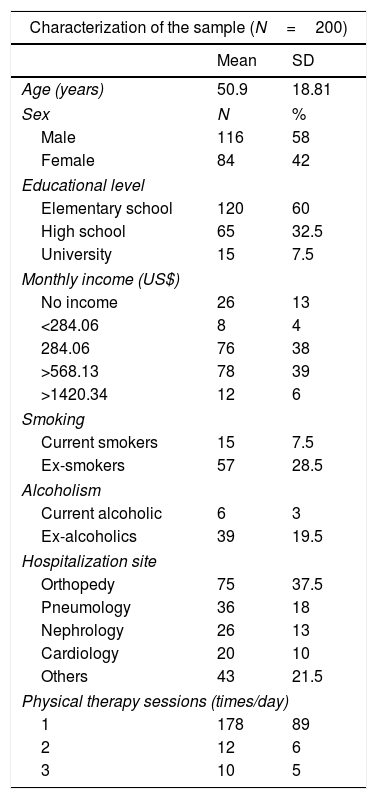
ResultsA total of 200 patients were evaluated; 58% were male, 60% had only elementary education and 39% had a higher monthly income than $568.13 (equivalent to more than two Brazilian minimum wages). Regarding hospitalization sector, 37.5% of patients were hospitalized in orthopedic sector, and most of them (89%) received only one physical therapy session per day. Patients’ detailed characteristics are presented in Table 1.
Descriptive characteristics of the study population.
| Characterization of the sample (N=200) | ||
|---|---|---|
| Mean | SD | |
| Age (years) | 50.9 | 18.81 |
| Sex | N | % |
| Male | 116 | 58 |
| Female | 84 | 42 |
| Educational level | ||
| Elementary school | 120 | 60 |
| High school | 65 | 32.5 |
| University | 15 | 7.5 |
| Monthly income (US$) | ||
| No income | 26 | 13 |
| <284.06 | 8 | 4 |
| 284.06 | 76 | 38 |
| >568.13 | 78 | 39 |
| >1420.34 | 12 | 6 |
| Smoking | ||
| Current smokers | 15 | 7.5 |
| Ex-smokers | 57 | 28.5 |
| Alcoholism | ||
| Current alcoholic | 6 | 3 |
| Ex-alcoholics | 39 | 19.5 |
| Hospitalization site | ||
| Orthopedy | 75 | 37.5 |
| Pneumology | 36 | 18 |
| Nephrology | 26 | 13 |
| Cardiology | 20 | 10 |
| Others | 43 | 21.5 |
| Physical therapy sessions (times/day) | ||
| 1 | 178 | 89 |
| 2 | 12 | 6 |
| 3 | 10 | 5 |
US$ – American dollars.
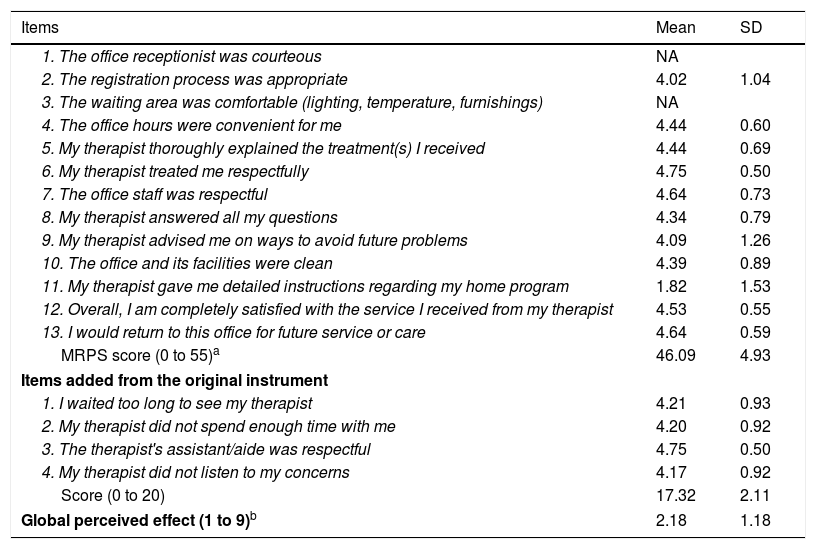
Table 2 summarized patients’ satisfaction mean (SD) for each MRPS instrument evaluated item (including four items from original instrument) and its total score, as well as the GPE. In general, patients were satisfied with physical therapy care, presenting an average of more than 4 in all items, except for items where the physical therapist would give home instructions, which obtained an average of 1.82 (1.53).
MRPS applied to study population.
| Items | Mean | SD |
|---|---|---|
| 1. The office receptionist was courteous | NA | |
| 2. The registration process was appropriate | 4.02 | 1.04 |
| 3. The waiting area was comfortable (lighting, temperature, furnishings) | NA | |
| 4. The office hours were convenient for me | 4.44 | 0.60 |
| 5. My therapist thoroughly explained the treatment(s) I received | 4.44 | 0.69 |
| 6. My therapist treated me respectfully | 4.75 | 0.50 |
| 7. The office staff was respectful | 4.64 | 0.73 |
| 8. My therapist answered all my questions | 4.34 | 0.79 |
| 9. My therapist advised me on ways to avoid future problems | 4.09 | 1.26 |
| 10. The office and its facilities were clean | 4.39 | 0.89 |
| 11. My therapist gave me detailed instructions regarding my home program | 1.82 | 1.53 |
| 12. Overall, I am completely satisfied with the service I received from my therapist | 4.53 | 0.55 |
| 13. I would return to this office for future service or care | 4.64 | 0.59 |
| MRPS score (0 to 55)a | 46.09 | 4.93 |
| Items added from the original instrument | ||
| 1. I waited too long to see my therapist | 4.21 | 0.93 |
| 2. My therapist did not spend enough time with me | 4.20 | 0.92 |
| 3. The therapist's assistant/aide was respectful | 4.75 | 0.50 |
| 4. My therapist did not listen to my concerns | 4.17 | 0.92 |
| Score (0 to 20) | 17.32 | 2.11 |
| Global perceived effect (1 to 9)b | 2.18 | 1.18 |
MRPS, MedRisk Instrument for Measuring Patient Satisfaction; NA, not applicable.
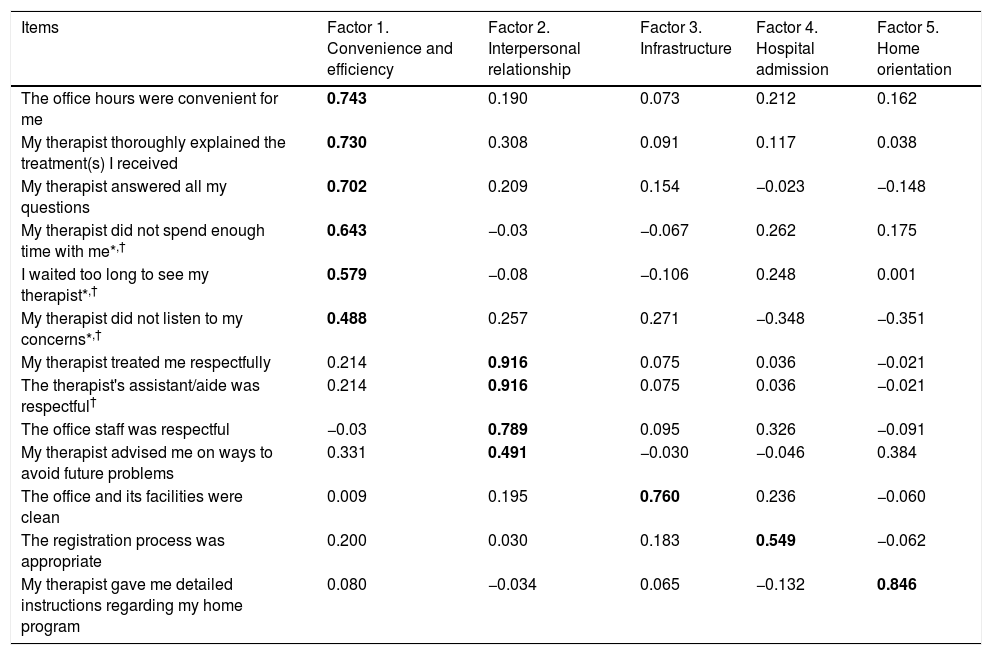
In Table 3, factorial exploratory analysis of five components was performed with 9 items (two items were considered “not applied” and two global items were not allocated to specific factors). Factor 1 is related to convenience and efficiency, factor 2 is about interpersonal relationship between patient and therapist, factor 3 is related to hospital infrastructure, factor 4 is referring to administrative hospital process (admission) and factor 5 is about home guidelines provided by physical therapist. All components (factors) explain 63.10% of total variation.
MRPS factor analysis applied to sample.
| Items | Factor 1. Convenience and efficiency | Factor 2. Interpersonal relationship | Factor 3. Infrastructure | Factor 4. Hospital admission | Factor 5. Home orientation |
|---|---|---|---|---|---|
| The office hours were convenient for me | 0.743 | 0.190 | 0.073 | 0.212 | 0.162 |
| My therapist thoroughly explained the treatment(s) I received | 0.730 | 0.308 | 0.091 | 0.117 | 0.038 |
| My therapist answered all my questions | 0.702 | 0.209 | 0.154 | −0.023 | −0.148 |
| My therapist did not spend enough time with me*,† | 0.643 | −0.03 | −0.067 | 0.262 | 0.175 |
| I waited too long to see my therapist*,† | 0.579 | −0.08 | −0.106 | 0.248 | 0.001 |
| My therapist did not listen to my concerns*,† | 0.488 | 0.257 | 0.271 | −0.348 | −0.351 |
| My therapist treated me respectfully | 0.214 | 0.916 | 0.075 | 0.036 | −0.021 |
| The therapist's assistant/aide was respectful† | 0.214 | 0.916 | 0.075 | 0.036 | −0.021 |
| The office staff was respectful | −0.03 | 0.789 | 0.095 | 0.326 | −0.091 |
| My therapist advised me on ways to avoid future problems | 0.331 | 0.491 | −0.030 | −0.046 | 0.384 |
| The office and its facilities were clean | 0.009 | 0.195 | 0.760 | 0.236 | −0.060 |
| The registration process was appropriate | 0.200 | 0.030 | 0.183 | 0.549 | −0.062 |
| My therapist gave me detailed instructions regarding my home program | 0.080 | −0.034 | 0.065 | −0.132 | 0.846 |
The findings of this study indicate that patients in physical therapy care were very satisfied with convenience and efficiency, interpersonal relationship with therapist, hospital infrastructure and administrative hospital process. However, home orientation provided by professionals needs to be improved. Most of obtained items averaged near or above 4 on a 1 to 5 scale (best answer). Among 200 evaluated patients, the majority (89%) received only one physical therapy care visit per day. Considering that 60% of patients had only elementary school education we can infer that lesser educated patients despite representing a substantially higher demand, become satisfied even when they receive the minimum care. These results can corroborate with Peiris et al. 6which affirmed that interpersonal relationship between therapist and patient seems to be a more important factor for patients in hospital settings than amount of therapy sessions received.6
The item with highest score was in reference to physical therapist/patient respect. Due to university hospital settings, patients received physical therapy care performed by undergraduate students and residents who are always oriented to be respectful to patients and their relatives. In contrast, item with the lowest score dealt with home guidelines. This may be attributable to the fact that not all patients were evaluated at the exact discharge moment. Also, hospital does not have an oriented and multidisciplinary discharge program, so several times physical therapists were not informed about patient's discharge, preventing professional from passing on appropriate home guidelines. In addition, university hospitals tend to have high resident turnover rates, and patients rarely have physicians or physical therapists who can treat them with regularity and address all their complaints.9
For evaluation and to explore how our patients understand MRPS items, a factorial analysis was performed. We found a factorial load that explains 63.10% of total variation with five factors, different from previous studies. The original MRPS study12 was performed with musculoskeletal patients and found three factors in factorial analysis and it explains 57.03% of total variation. Oliveira et al.13 evaluated the satisfaction level of musculoskeletal patients also and found three factors in their validation study in Brazilian Portuguese: “interpersonal”, “convenience and efficiency” and “patient education” that explains 53.8% of total variation. What we can observe is that some items could be not only in a single factor, such as “My therapist advised me on ways to avoid future problems”. It has a higher load in factor 2 (interpersonal relationship), but could also be allocated in factor 5 (home orientation), which presents only one item. However, we believe that it is a very important item for evaluation in hospital environments, since this is the lowest score and that it should be improved both in physical therapeutic treatment and in new learning strategies and interprofessional education in hospital scope.
Different population studies have shown that home guidelines are essentially important to patients and to those who live with them, since they help prevention and rehabilitation.16,17 By broadening people's knowledge about rehabilitation indications and contraindications in relation to presented disease, some continuity can be given to home treatment, which can help prevent negative attitudes from forming that may cause complications in patient's health status and even possible readmission.16,17
Medeiros et al. evaluated patient satisfaction with musculoskeletal conditions under physical therapy treatment in Brazil's southeast region through MRPS instrument and also observed a high satisfaction level with service provided.5 In addition to this study, Casserley-Feeney et al.18 evaluated physical therapy satisfaction in patients having musculoskeletal conditions, however, this study took place in a developed country where a high satisfaction level with physical therapy services was noted.18
Almeida et al. evaluated satisfaction level in patients under care at a public university hospital in Brazil (as well as in this study) and reported that patients were satisfied even under public health service care.19 In a public university hospital, patients are often admitted where vacancy is available at that moment, e.g. patients can present a cardiologic disease and can be hospitalized in a nephrology ward. Results observed in this study showed us that this condition was not important to patient satisfaction. This suggests that studies that evaluate patients’ satisfaction under physical therapeutic care tend to present a positive result (ceiling effect), independent of whether physical therapy service provided is public or private.5,18,19
As a limitation of this study, we can point out that MRPS instrument was not directly validated for physical therapy care in hospital settings and that evaluations (instrument application) were done close to hospital discharge moment, but not exactly on discharge day. This situation may have contributed to a lower score on items that evaluate how patients were instructed to continue treatment in home environment. In addition, we should point out that perhaps results obtained in this study cannot be generalized to less developed cities and states. As a strong point, even with all limitations found, including lack of human resources, infrastructure, and materials, professionals are committed to respect and care for patients, dedicating and committing themselves to obtain better results.
This study makes it possible to inform physical therapists working in hospitals how to improve their delivery services, especially concerning home guidelines and need to reeducate multidisciplinary teams in relation to patients’ discharge, thus facilitating future investments for local improvements regarding patient perceptions. We also suggest future studies that can validate and adapt MRPS for patients in hospital setting. Given results obtained, we can conclude that hospital patients in this study were satisfied with physical therapy service provided.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to specially thank to Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq, Scholarship Program and to physical therapists Mariana Mestieri, Marley Cintra and Pedro Gabriel Barbosa for all support during this study.



