



Physical performance tests provide a more complete picture of the functional status of the athlete's upper extremity.
ObjectivesThe primary purpose was to evaluate the reliability of the Modified Closed Kinetic Chain Upper Extremity Stability Test (MCKCUEST) in adolescent volleyball and basketball players. The secondary objective was to evaluate the relationship between the MCKCUEST and shoulder rotation isometric strength in this population.
MethodsSeventy-three healthy basketball (n=39) and volleyball (n=34) players participated to establish the reliability and correlations of the MCKCUEST. We used a two-session measurement design to evaluate the reliability of the MCKCUEST. Shoulder rotation isometric strength was performed to determine relationships with the MCKCUEST.
ResultsThe intraclass correlation coefficients (ICC2,1) for intra-session reliability of the MCKCUEST ranged from 0.86 to 0.89, and the between days test–retest reliability (ICC3,1) was 0.93. The standard error of measurement (1 touch) and the minimal detectable change (3 touches) showed clinically acceptable absolute reliability values. A weak correlation was found between the MCKCUEST power score and shoulder rotation isometric strength (r values between 0.3 and 0.4).
ConclusionsResults demonstrated good to excellent relative reliability and clinically acceptable absolute reliability values for the MCKCUEST on adolescent basketball and volleyball athletes. Performances on the MCKCUEST were weakly associated with shoulder rotation strength.
The increase in adolescent sport participation over the past years and the specialization in a single sport with intensive repetitive activity at younger ages increase the risk of sustaining an overuse injury.1–3 This risk is nearly twice higher compared to adolescents with low specialization.1–3 In total, 30% of sports-related injuries among throwing young athletes occur in the shoulder.3 Consensus statements released by healthcare and sports organisations recognize the importance of upper limb screening examination as part of the periodic young athlete's health evaluation.4–6
Physical performance tests are a part of this screening examination, provide a more complete picture of the functional status of the athlete's upper extremity, and are routinely used for performance enhancement or post-rehabilitation outcome measures.7–10 Furthermore, physical performance tests are, most of the time, easily performed in many different environments and contexts with minimal material,5,11 and are thus, very popular. The Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) is one of the most popular physical performance tests to assess upper body function.11 Despite reliable and valid results within the adult population,9,12–16 data about the CKCUEST on adolescents is scarce.17 Moreover, results on adults should not be generalized to young athletes because of the differences in anthropometric characteristics. In previous studies, the CKCUEST was performed in accordance with the guideline described by Tucci et al.9 and Goldbeck and Davies14 with participants adopting a push-up position with a fixed 91.4cm distance between hands. However, this standardized distance may not be appropriate for adolescents by being too wide for some young individuals or too narrow for others.12,17,18 Other studies performed the test with participants adopting a push-up position with their hands located directly under their shoulders12,19 or with hands placed at a width 50% of the participant's height.12
Overuse injuries have been associated with strength impairments affecting the balance between shoulder internal and external rotator muscles.20–22 To the best of our knowledge, only a few studies have examined the relationship between the CKCUEST and shoulder rotation strength.23,24 Lee and Kim23 reported a high correlation between the CKCUEST mean touches and isokinetic shoulder rotation strength while Decleve et al.24 showed moderate correlations between the CKCUEST mean touches and power score and shoulder rotation strength. However, normalizing the hand spacing at shoulder width may influence the relationship found in these previous studies.
The primary purpose of our study was to determine the relative and absolute reliability of the Modified CKCUEST (MCKCUEST)12 in a population of healthy adolescent volleyball and basketball players. We hypothesized that normalizing the hand spacing at shoulder width may be an alternative to improve the consistency in the CKCUEST on adolescent athletes. The secondary purpose of our study was to examine if performance on the MCKCUEST was correlated with the isometric shoulder rotation strength of adolescent volleyball and basketball players.
MethodsStudy design and participantsThis cross-sectional study was performed following the STROBE recommendations.25 The study was conducted from September to December 2019. Participants were recruited from local basketball and volleyball settings in Brussels and Charleroi (Belgium). Participants were included if they were aged between 12 and 17 years, were in good general health, and played at competitive level minimum 3h per week. The exclusion criteria for both groups were a history of orthopaedic surgery of the upper quadrant or spine or reports of pain in these regions within a 6-month period before the study. All participants provided written informed consent signed by the legal guardians. The study was approved by the Ethical Committee of the Cliniques Universitaires Saint-Luc, Brussels, Belgium 2018/04JUL/275 – No. B403201837036.
Sample sizeBased on a pilot study on 12 adolescents, sample size was calculated based on our primary purpose using the G*power 3.1.7 program and considering: α=0.05; β=0.10 (90%); power correlation ratio to null hypothesis (ρH0)=0.35; correlation ratio for alternative hypotheses (ρH1)=0.80, and a potential loss of 20%.26,27 At least 34 participants were needed for the study.
ProcedureThe participants attended two assessment sessions conducted by the same investigators properly trained for the test (four fourth-year physical therapy students under supervision of a physical therapist with over 14 years of clinical experience). Two investigators were responsible for counting the touches and the timing and two others were responsible for the test performance.
To evaluate test–retest reliability and to avoid possible memory recall, the MCKCUEST was performed on two sessions (day 1 and day 2), separated by seven days. Participants were not informed about the scores obtained during the first assessment to minimize the motivational effects. In addition, on day 1, we performed strength assessment using the Self-Assessment Corner.24 The testing order was randomized on day 1 by instructing participants to choose cards to determine which test would be done first.
Modified Closed Kinetic Chain Upper Extremity Stability Test (MCKCUEST)Participants adopted a push-up position with a flat back parallel to the floor (Fig. 1).9,14 Previous studies have suggested that females should assume a modified push-up position, with knees on the ground, when performing the CKCUEST.9,17 However, we decided to test the female participants with the same push up position that was used to test the male participants to standardize the procedure for both sexes. To avoid the influence of the anthropometric characteristics of individuals,18 we used the inter-acromial distance, measured with a tape measure from the tip of the right acromion to the tip of the left acromion of each participant, instead of the standardized between hands distance of 91.4cm.9,12,14 Two parallel and aligned lines with the inter-acromial distance of the individual were marked on the floor to determine the position of the hands. For 15s, participants were instructed to move one hand to touch the dorsum of the opposite hand and then return the hand to the starting position. Subsequently, the same movement was performed with the other hand. Participants were instructed to perform as many alternating touches as possible. The number of touches was recorded. After instructions and demonstration, a familiarization trial was performed, consisting of 5 repetitions. Verbal cues were given during familiarization when necessary. Finally, three test trials were performed. Every trial lasted 15s with 45s rest in between.14 The MCKCUEST provides 3 scores: (1) the number of touches the participant performed in 15s; (2) the normalized score that is obtained by dividing the number of touches by height, and (3) the power score is calculated by multiplying the average number of touches by 68% of the participant's body mass in kilograms (which corresponds to the mass of the upper extremity, head, and trunk), and then divide that score by 15.14
Self-Assessment Corner procedure Starting position. (B) Ending position.")
The procedure was performed following the guidelines as described by Decleve et al.24,28 We started with verbal instructions from the investigators. Participants were instructed to stand up straight, barefoot, with the non-tested hand on the back at the level of the 4th and 5th lumbar vertebrae and the opposite foot of the tested arm placed forward (Fig. 2). The forearm was placed against the hand-held dynamometer (MicroFET2 HHD, Hoggan Health industries Inc, West Jordan, UT, USA) 2cm proximal of the ulnar styloid process on the dorsal or ventral forearm for strength assessment for external and internal rotation, respectively. Both external rotation and internal rotation were assessed in 90° of shoulder abduction in the frontal plane, 90° of shoulder external rotation, and 90° of elbow flexion with neutral rotation of the forearm. This shoulder position allows to test in a more overhead functional position. Three repetitions of 5 seconds of maximal voluntary effort were performed with 10s of rest between trials. Participants had to build their force gradually to a maximum voluntary contraction over a 2-s period and had to keep the maximal voluntary contraction for 5s.29 The Self-Assessment Corner test has good to excellent reliability.24 The absolute isometric strength data were expressed in Newton (N).
Statistical analysis
Means and standard deviations were calculated across participants for all dependent variables. The MCKCUEST (mean number of touches, normalized score, and power score) and shoulder external and internal rotation strength were analyzed. The Shapiro–Wilk test was first used to evaluate the normality of the distribution within all measurements. All data were normally distributed.
To assess relative reliability, intraclass correlation coefficients (ICC) were calculated with the corresponding 95% confidence intervals (CI).30 To assess intra-session reliability between trials within day 1 and day 2, we calculated ICC2,1. To assess test–retest reliability between day 1 and day 2 we calculated ICC3,1. Interpretation was based on the guidelines by Shrout and Fleiss,31 with values >0.90 reflecting excellent reliability; values between 0.80 and 0.89, good reliability; between 0.70 and 0.79, moderate reliability; and values <0.70, low reliability. To examine the absolute reliability of the MCKCUEST, the standard error of measurement (SEM) and the minimal detectable change (MDC) were calculated using between days measurements. The SEM was calculated as SD×√1−ICC, where SD is the SD of all scores of the participants.32 The SEM was used for calculating the MDC95, which was calculated as SEM×1.96×√2.
To analyze a possible correlation among the performance on the MCKCUEST (mean number of touches, normalized score, and power score) and the strength variables, we used the Pearson product moment correlation (r). The r value was categorized as weak (<0.499), moderate (0.5–0.707), or strong (>0.707).33 The Alpha was set at 0.05. All statistical analyses were performed using SPSS (version 23; IBM Corp, Armonk, NY, USA).
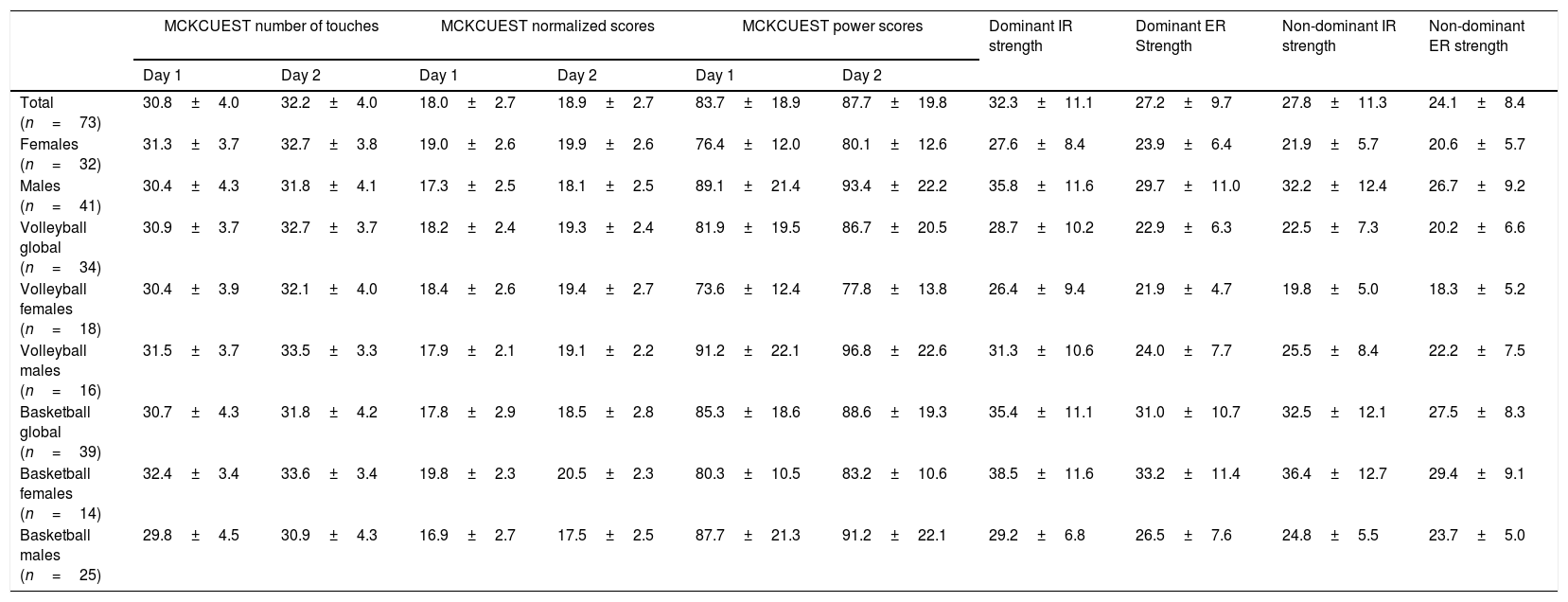
ResultsSeventy-three adolescent healthy basketball and volleyball players completed the study. Demographic characteristics of all participants are presented in Table 1. Results of the MCKCUEST and isometric shoulder rotation strength stratified by sex and sports for day 1 and day 2 are summarized in Table 2.
Demographic characteristics of the total sample and stratified by sports.
| Total sample (n=73) | Basketball (n=39) | Volleyball (n=34) | |
|---|---|---|---|
| Age (years) | 14.7±1.4 | 14.9±1.4 | 14.4±1.4 |
| Body mass (kg) | 60.2±12 | 61.6±11.5 | 58.6±12.5 |
| Height (m) | 1.7±0.1 | 1.7±0.1 | 1.7±0.1 |
| Sex (male/female) | 41/32 | 25/14 | 16/18 |
| Hours a week | 7.4±3.9 | 8.8±4.5 | 5.8±1.9 |
Data are presented as mean±standard deviation.
Descriptive analysis for the MCKCUEST and isometric internal and external rotation strength stratified by total, sex, and sports between day 1 and day 2.
| MCKCUEST number of touches | MCKCUEST normalized scores | MCKCUEST power scores | Dominant IR strength | Dominant ER Strength | Non-dominant IR strength | Non-dominant ER strength | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Day 1 | Day 2 | Day 1 | Day 2 | Day 1 | Day 2 | |||||
| Total (n=73) | 30.8±4.0 | 32.2±4.0 | 18.0±2.7 | 18.9±2.7 | 83.7±18.9 | 87.7±19.8 | 32.3±11.1 | 27.2±9.7 | 27.8±11.3 | 24.1±8.4 |
| Females (n=32) | 31.3±3.7 | 32.7±3.8 | 19.0±2.6 | 19.9±2.6 | 76.4±12.0 | 80.1±12.6 | 27.6±8.4 | 23.9±6.4 | 21.9±5.7 | 20.6±5.7 |
| Males (n=41) | 30.4±4.3 | 31.8±4.1 | 17.3±2.5 | 18.1±2.5 | 89.1±21.4 | 93.4±22.2 | 35.8±11.6 | 29.7±11.0 | 32.2±12.4 | 26.7±9.2 |
| Volleyball global (n=34) | 30.9±3.7 | 32.7±3.7 | 18.2±2.4 | 19.3±2.4 | 81.9±19.5 | 86.7±20.5 | 28.7±10.2 | 22.9±6.3 | 22.5±7.3 | 20.2±6.6 |
| Volleyball females (n=18) | 30.4±3.9 | 32.1±4.0 | 18.4±2.6 | 19.4±2.7 | 73.6±12.4 | 77.8±13.8 | 26.4±9.4 | 21.9±4.7 | 19.8±5.0 | 18.3±5.2 |
| Volleyball males (n=16) | 31.5±3.7 | 33.5±3.3 | 17.9±2.1 | 19.1±2.2 | 91.2±22.1 | 96.8±22.6 | 31.3±10.6 | 24.0±7.7 | 25.5±8.4 | 22.2±7.5 |
| Basketball global (n=39) | 30.7±4.3 | 31.8±4.2 | 17.8±2.9 | 18.5±2.8 | 85.3±18.6 | 88.6±19.3 | 35.4±11.1 | 31.0±10.7 | 32.5±12.1 | 27.5±8.3 |
| Basketball females (n=14) | 32.4±3.4 | 33.6±3.4 | 19.8±2.3 | 20.5±2.3 | 80.3±10.5 | 83.2±10.6 | 38.5±11.6 | 33.2±11.4 | 36.4±12.7 | 29.4±9.1 |
| Basketball males (n=25) | 29.8±4.5 | 30.9±4.3 | 16.9±2.7 | 17.5±2.5 | 87.7±21.3 | 91.2±22.1 | 29.2±6.8 | 26.5±7.6 | 24.8±5.5 | 23.7±5.0 |
Data are presented as mean±standard deviation; MCKCUEST data are expressed as number of touches; strength data are expressed in Newton, MCKCUEST, Modified Closed Kinetic Chain Upper Extremity Stability Test.
Intra-session reliability between trials within day 1 and day 2 showed good reliability with ICC2,1 values ranging from 0.86 (95% CI=0.80, 0.90) on day 2 to 0.89 (95% CI=0.81, 0.93) on day 1. The test–retest reliability between day 1 and day 2 showed excellent reliability with ICC3,1 value of 0.93 (95% CI=0.63, 0.97). The SEM was 1.1 touches and the MDC95 was 3.04 touches.
Results of the correlation analysis are summarized in Table 3. Weak non-significant correlations were found for all variables except for the MCKCUEST power score that showed significant weak correlation with shoulder strength variables (r ranging from 0.3 to 0.4).
Results for correlations analysis between the Modified Closed Kinetic Chain Upper Extremity Stability Test (mean touches and normalized and power scores) and the dominant and nondominant shoulder isometric external and internal rotation strength (N=73).
| MCKCUEST mean touches | MCKCUEST normalized score | MCKCUEST power score | ||||
|---|---|---|---|---|---|---|
| Pearson product moment correlation coefficient (r) | ||||||
| Dominant | Non dominant | Dominant | Non dominant | Dominant | Non dominant | |
| External rotation isometric strength | 0.09 | 0.05 | −0.11 | −0.12 | 0.31* | 0.33* |
| Internal rotation isometric strength | 0.05 | 0.10 | −0.15 | −0.10 | 0.43* | 0.40* |
The primary purpose of our study was to evaluate the intra-session and test–retest reliability of the MCKCUEST on adolescent athletes. This test was modified from the original testing procedure proposed by Goldbeck and Davies14 by spacing hands at shoulder width using the inter-acromial distance to adapt the starting position to the anthropometric characteristics of the individuals.12,18
The MCKCUEST displayed good to excellent intra-sessions and test–retest reliability on the adolescent athletes which is in contrast to the study of Oliveira et al.17 that found weak ICC value (ICC=0.68) on adolescents using the initial push-up position with hands placed 91.4cm apart. The initial standardized hands distance may be a factor that contributes negatively to their results.17,18 Spacing hands at shoulder width using the inter-acromial distance placed adolescent athletes at an advantage when performing the MCKCUEST compared to the original CKCUEST. Anthropometric characteristics of individuals such as narrower shoulder width and/or shorter arm length may interfere with the results by increasing effort needed to stabilize the upper body when the initial standardized hands distance is applied.34 In our study, both sexes used a push-up position while Oliveira et al.17 adopted a knee push-up position for adolescent females. If we compare our results to other reliability studies performed on adults (ICC range: 0.77–0.96; SEM range: 0.9–2.8; MDC95 range: 2.6–7.8),9,12–16,23,35 we show similar results. However, a variety of testing procedures used in the literature, makes comparisons between these studies difficult regarding the average number of touches, SEM, and MDC.7,9,12–17,19,23,35 The CKCUEST as originally described by Goldbeck and Davies14 was performed by athletic male students in a push-up position with their hands touching parallel pieces of tape placed 91.4cm apart. They reported an ICC of 0.92 and number of touches of 27.814 while Lee and Kim23 reported on adults an ICC of 0.97 and an average number of touches of 13. In the study of Sciascia and Uhl13 on symptomatic and asymptomatic participants they reported an ICC ranging from 0.85 to 0.86, an average of touches of 22, a SEM of 2, and MDC of 4.
Some other studies adopted a modified knee push-up position for female participants.9,17 Tucci et al.9 evaluated the test–retest reliability of the CKCUEST in sedentary and active individuals with or without shoulder injury. They demonstrated an ICC ranging from 0.82 to 0.96, an average number of touches ranging from 11 to 30, a SEM of 1.4 to 2.8, and an MDC of 2 to 4.9 De Oliveira et al.17 studied the reliability of the CKCUEST on male and female adolescents using a knee push-up position for female participants. They reported an ICC of 0.68, an average number of touches of 26.8, a SEM of 2.2, and MDC of 6.
Other studies adapted the starting positions of the hands.12,19,34,36 Tarara et al.36 instructed the participants to assume a push-up position with hands located directly under the shoulders to begin the test. The parallel pieces of tapes remained 91.4cm apart. They reported on active college students an ICC ranging from 0.73 to 0.78 and SEM from 7 to 8. Hollstadt et al.19 reported on college basketball players an average of touches ranging from 25 to 32 and Taylor et al.34 reported a range from 23 to 25 on collegiate athletes. Callaway et al.12 evaluated the reliability of 4 variations of hand starting position on adult males. The first variation was the standard test described by Golbeck and Davies.14 The second adaptation spaced hands at shoulder width using the inter-acromial distance similar to our testing procedure. The third variation started with hands at shoulder width and reached the 91.4cm distance, and the last variation placed the hands at 50% of the participant's height. They determined an ICC from 0.84 to 0.93, a SEM ranging from 1.5 to 2.8, and MDC ranging from 4.1 to 7.8 touches. The second variation from Callaway et al.12 is of interest because it is similar to our testing position and comparisons can be drawn. Even though our study shows similar good ICC values compared to our mean scores, the SEM and MDC95 are slightly lower. Our mean score is 30.8 touches on day 1 and 32.2 touches on day 2 while they found 34.2 touches on adult male population. We obtained a SEM of 1 and MDC95 of 3 compared to 2.8 and 7.8, respectively. These SEM and MDC95 values enhance sensitivity to change. Our MDC95 value suggests that a change of 3.04 touches (approximately 10% of the mean score) is indicative of a true change while their study12 shows a %MDC95 of 23%.
From a clinical perspective, the CKCUEST as originally described14 may not be appropriate for assessing all athletes interchangeably. Our study demonstrates that the MCKCUEST is a reliable alternative to CKCUEST that enables to standardize the test to any adolescent population regardless of individual anthropometric difference or sex.
Our results showed only weak correlation between the MCKCUEST power score and shoulder strength variables. Previous studies23,24 have examined the relationship between the CKCUEST and isokinetic or isometric shoulder rotation strength. Lee and Kim23 found a high correlation with the isokinetic shoulder external and internal rotation strength at angular speed of 60°/s and 180°/s (r range=0.87–0.94) while Decleve et al.24 showed moderate correlation with isometric shoulder external and internal rotation strength (r range=0.49–0.65). In their studies23,24 participants performed the initial CKCUEST with the standardized between hands distance of 91.4cm in a push-up position23 or a knee push-up position for female.24 The body position when performing the initial CKCUEST requires a substantial amount of coordination between scapular, glenohumeral, elbow, and forearm muscles and also trunk strength and stability.16 In our study, the modification of hands spaced at shoulder width using the inter-acromial distance might influence the results with adolescents relying more on other upper limb or trunk muscles to perform the MCKCUEST.
Limitations and future perspectiveThe interpretation of our results is limited to reporting the reliability and relationships of the MCKCUEST in a sample of healthy adolescent basketball and volleyball players. Extrapolation of these results to other overhead athletes should be done with caution. The increase in the MCKCUEST mean score between days might be attributed to a learning effect. One limitation of the CKCUEST or MCKCUEST is that it might not be suitable for initial or mild-level stages of shoulder rehabilitation due to its challenging requirements. The development of new shoulder functional tests that are less demanding should be investigated.
ConclusionsRelative reliability of the test was good to excellent and absolute reliability was clinically acceptable in adolescent basketball and volleyball players. Finally, a weak correlation was found between the MCKCUEST power score and isometric shoulder internal and external rotation strength.
Conflicts of interestThe authors declare no conflict of interest.



