





The use of local muscle vibration is a promising technique to improve motor performance in people with movement impairments. Majority of studies have failed to properly describe the used system and its reliability, making it difficult to transfer this promising technique to clinical practice.
ObjectiveTo describe technical details of a custom-made vibratory system (RCVibro System), as well as to determine its reliability and functionality.
MethodsThe vibration frequency and the electric potential difference/vibration frequency curve of six devices were assessed (at the same day and at different days), allowing us to determine the system reliability. In addition, the RCVibro System functionality was analyzed by the center-of-pressure behavior assessment during the tibialis anterior bilateral stimulation in fifteen young people.
ResultsThe RCVibro System showed a very-high reliability between assessments within the same day (ICC(2,6) ranging from 0.95 to 0.99; p<0.01) and between different days (ICC(2,6) ranging from 0.81 to 0.98; p<0.01). We also observed a forward center-of-pressure displacement (p<0.01) and an increase in the center-of-pressure velocity (p<0.01).
ConclusionWe conclude that RCVibro System is a highly reliable system. The results demonstrate the potential usage of RCVibro System in clinical and research settings. Further investigation is needed in people with motor and neurological disorders.
Muscle vibration has been used to investigate the effects of pathological processes in the proprioceptive system1,2 and/or with the intention to improve gait performance in people with motor disabilities.3–5 The main vibratory effect is the sensory intramuscular Ia type fibers firing,6 which leads to an illusory stretching sensation.7 As a result, during upright standing, an involuntary center-of-pressure (CoP) shift toward the receptor-bearing muscle is observed.8,9 Due to its low cost and non-invasive aspect, muscle vibration has been used as an interesting instrument to improve movement of motor impaired people.4,5,10,11 Although muscle vibration could be used as a novel strategy to improve movement,3,12,13 this technique is not well-spread in clinical day-life, possibly due to the inexistence of commercial equipment with high-standard quality.
Multi proposal vibratory devices are commercially available, however they were not designed for research/clinical proposes. Hence, it is suggested that those equipment are not reliable and precise, such as when the vibration frequency and amplitude, are considered. Indeed, in pilot data, we observed very low vibration frequency reliability in these multi proposal vibratory devices. Majority of the studies investigating vibratory effects on movement of impaired people used custom devices.1,4,5,9 However, most of them failed to properly describe the technical features of these devices, making it impossible to replicate their findings. Another important issue with the use of custom devices is that the system reliability is rarely reported.
Thereby, the primary aim of this study was to describe the technical details of a custom-made vibratory system (named RCVibro System) and determine its reliability. The secondary aim was to check the RCVibro System functionality by replicating postural effects already observed by previous studies.7,8,14 We expected that the RCVibro System would be a reliable system.
MethodsVibratory devicesAll vibratory devices, as exemplified in Fig. 1 (left panel) were constructed using steel DC micro devices (model 1319006SR – Faulhaber® – Switzerland) with a maximal nominal tension of 6V, maximal no-load speed of 13,100rpm and weighing 12g each. An eccentric load (weighing 0.5g; 1cm of diameter) was attached to each micro device axis. The rotational velocity of the eccentric mass, and therefore the vibration frequency, is linearly determined by the amount of electrical potential difference given to each micro device (details in the Results section). Hence, electrical wires were fixed to each device using ordinary soldering. The sets (devices plus eccentric masses) were embedded in a custom cylindrical enclosure made of non-toxic polyvinyl chloride (PVC), measuring 4.5cm×2cm×2cm, weighing 12g. In total, each vibratory device weighed between 27g and 31g. The designed configuration allowed vibration only in 2-D directions (X=anteroposterior; Z=mediolateral).
Logical control board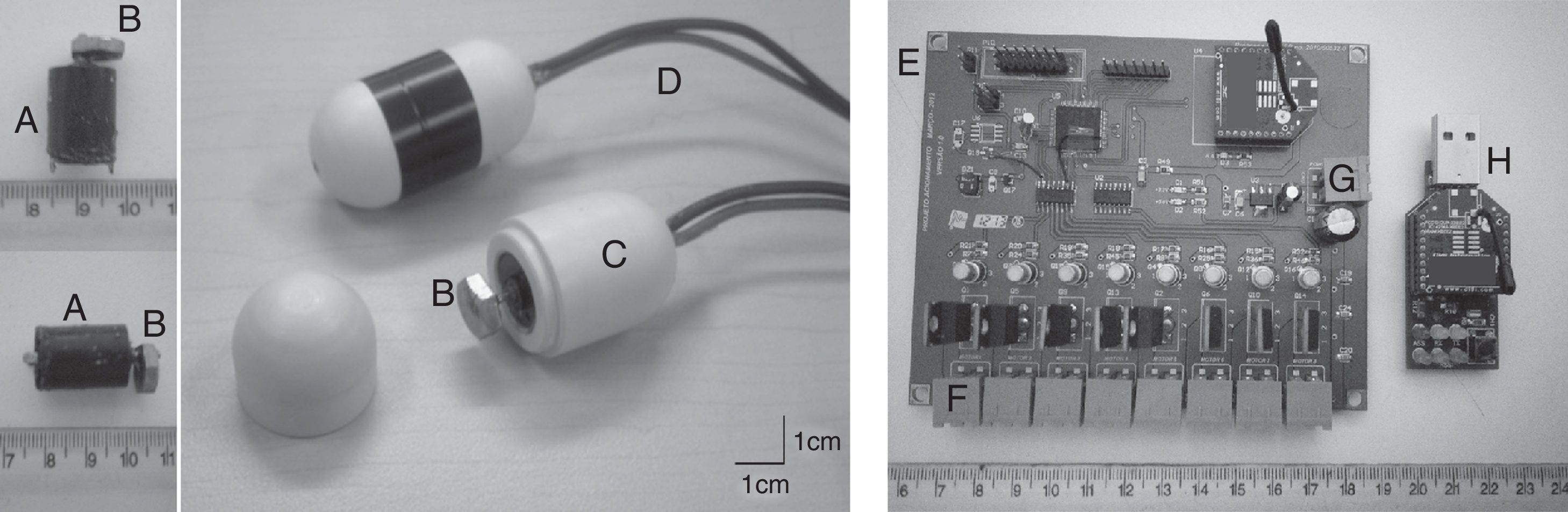
In the RCVibro System, each vibratory device is controlled by a custom electronic board (Fig. 1 – right panel) measuring 12cm×12cm and controlled by a Zigbee network protocol (radio transmission). The Zigbee controller module may be connect to any computer, via USB (Fig. 1). The custom-made board (powered by a 5V AC adapter) can control up to eight different vibratory devices and allows through ordinary hyperterminal software, the manipulation of both vibration onset moment and frequency. This manipulation can be applied to all vibratory devices simultaneously or individually. Also, the vibration frequency of each device is manipulated by the command “at+x=y” in a hyperterminal software, whereas “x” is the target channel and “y” is the percentage of the maximal given electric potential difference (100% is equal to 5V). This board can be attached on a belt or in a backpack, which allows the participant to move freely.
RCVibro System calibration and reliabilitySince the devices axis rotational velocity is dependent on the given electric potential difference, it was necessary, for each vibratory device (six were separately tested), to achieve a percentage of electric potential difference/vibration frequency curve. Therefore, a three-dimensional optoelectronic movement analysis system was used (OPTOPTRAK Certus – NDI®). This system has an accuracy of 0.1mm and a resolution of 0.01mm. Thus, the OPTOPTRAK system is sensitive enough to detect the vibratory movement. Since frequencies higher than 218Hz were not expected (maximal no-load speed of 13,100rpm) and to respect the Nyquist theorem, a sample acquisition rate of 500Hz was used. In each device, an infrared emitter diode (IRED) was fixed using adhesive tape. No emissors movement was observed during the assessments. The vibratory devices were fixed in a vertical position, allowing free movement in two directions (X and Z).
The electric potential difference for each vibratory device was increased in series of 7% of total, resulting in eleven points series (14–84%; lower percentages were excluded, since, in some devices, they did not promote any movement; higher percentages were not used to avoid any mechanical damage on vibratory devices). A 5s vibration period was assessed for each electric potential difference. The position of each marker was offline filtered using a low-pass 4th order Butterworth filter with a 10Hz cut-off frequency. The 5s periods was then split into six 0.5-s periods, with 0.5-s overlap (the first and last second of data collection were excluded): 1–1.5s, 1.5–2.0s, …, 3.0–3.5s, 3.5–4.0s. For each period, the power spectrum of each marker position was determined using power spectral density (PSD) analysis through specific-designed MatLab (MathWorks®) codes. The power spectrum had a resolution of 0.66Hz.
Afterwards, we determined the peak power frequency for each 0.5-s, for all electric potential difference percentages for both X and Z directions. This procedure allowed us to determine: (i) the percentage of electric potential difference/vibration frequency curve for each device (Fig. 2); (ii) the vibration variability within the 5s data-sampling period (through the coefficient of variation ([standard deviation*100]/mean).
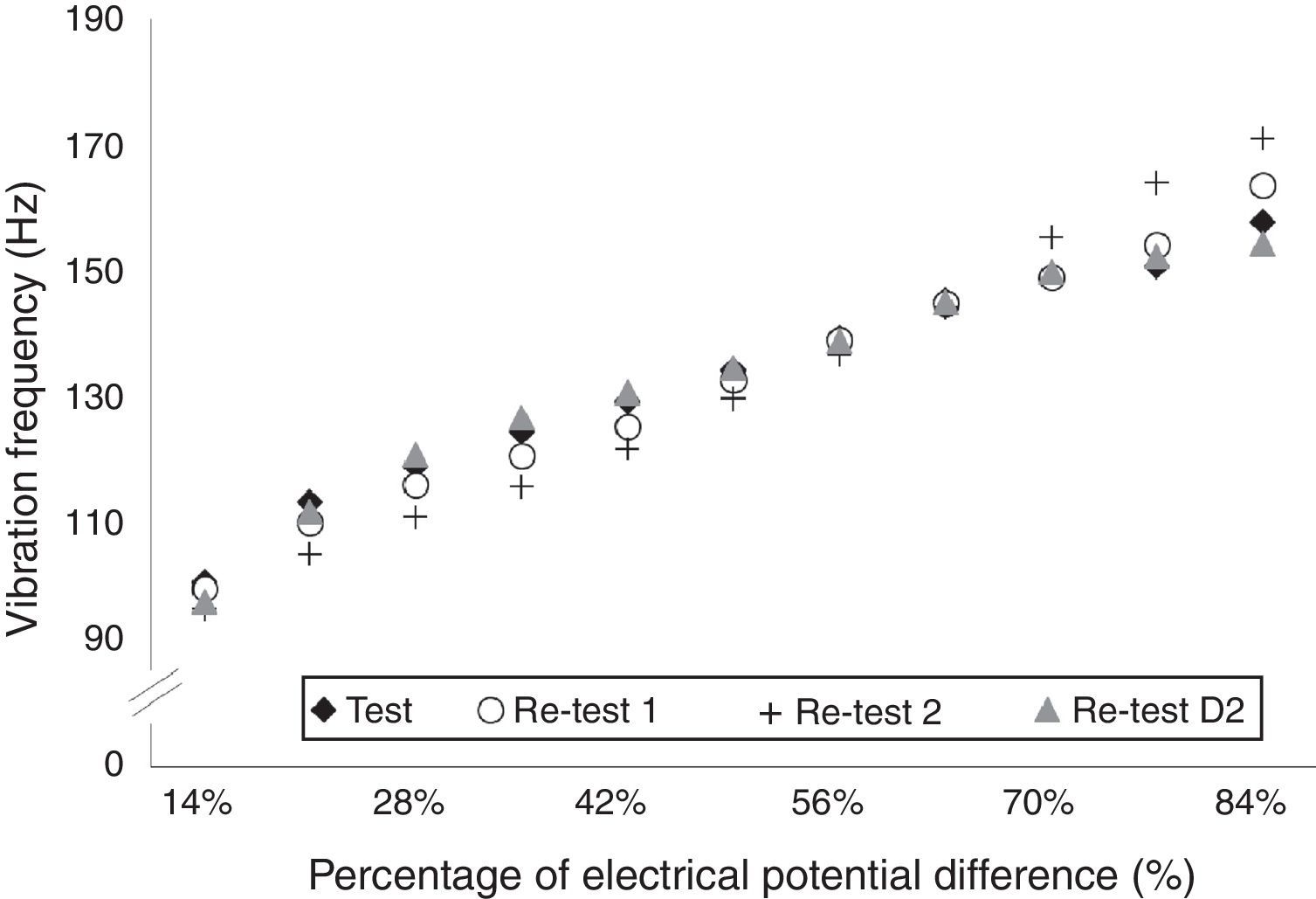
In order to assess the system test–retest reliability in the same day, these procedures were repeated three times, named Test, Re-Test 1 and Re-Test 2. They were performed two hours apart from each order. Additionally, in order to assess the test-retest reliability between different days, a fourth test (named Re-Test D2) was repeated 24h after Test. For the reliability (defined as the extent to which scores have not changed for repeated measurements),15 we considered the mean vibration frequency between the six 0.5-s periods. For each device, to assess the reliability within days, we used ICC(2,6) procedures among Test, Re-Test 1 and Re-Test 2; to assess the system reliability between days, we used the ICC(2,6) procedures between Test and Re-Test D2.16,17 The standard error of measurement (SEM) was also determined. Finally, we verified the Minimal Detectable Change (MDC) for each device using the following formula: MDC=SEM×1.96×√2. The MDC reflects the value needed to be changed at 95% of confidence to be considered a real change and not a difference given by a measurement error.
RCVibro System functioning testIn order to assess the proper functioning of the entire custom-made system and also, to ensure that the same effects observed in previous studies8,9,14 could be replicated by the RCVibro System, we assessed the CoP behavior during upright standing. Undergraduate and graduate students were invited to participate in this study through personal communication. A convenience sample of 15 subjects was determined. The CoP behavior of these fifteen healthy young adults (7 males, 8 females; mean (standard deviation) age of 26.29±6.46 years; 167.71±7.89cm of height; and 68.86±8.76kg of weight) was assessed while standing with eyes closed in two conditions: without and with vibration, applied bilaterally on the tibialis anterior muscle. This research has been approved by the local Ethical Board (Protocol: 083/2010 – Comitê de Ética em Pesquisa em Seres Humanos – IB, Universidade Estadual Paulista (UNESP), Rio Claro, SP) and an informed consent form was signed by all participants.
Two sets of trials were conducted, without randomization, maintaining the order: without (OFF) and with vibration (ON). This order was chosen to avoid any lasting vibration effect in OFF. Since only three trials were used (described ahead) and only healthy young participants were assessed, we do not believe in a fatigue-effect in the second round of trials (ON). During all attempts, the participants were asked to maintain an upright posture for 40s, standing on a force plate (AMTI®) with eyes closed (to enhance the vibratory effect14). The feet position was standardized for each participant and it kept consistent across all trials. The positioning of the CoP in relation to the force plate zero offset was assessed using the Balance Clinic software (AMTI®) with a sample rate of 200Hz. A resting time of 30s was given to participants between attempts. In total, three trials of each condition were performed, and the average of them was considered for analyzes.
For all conditions, the vibratory devices (position detailed below) were switched on at 10th second of data collection and a 30s vibration period was used to elicit postural effects. To investigate the effect of vibration on the CoP behavior, the CoP anteroposterior (A-P) position, CoP area and CoP mean velocity were assessed at two moments: at the close-to-last five seconds without vibration (4–9th seconds of data collection) and at the close-to-last five seconds of vibration (34–39th seconds of data collection). The CoP area was determined using the 95% confidence ellipse.18
Vibration was applied bilaterally on the tibialis anterior muscle belly. The devices used on the functioning test were randomly chosen from the six devices tested previously. All subjects used the same devices. The tibialis anterior muscle was chosen since this muscle is sensitive to local vibration.8,9,19 The devices were distant approximately 4.5cm proximal to the center of the muscle belly (adapted from the SENIAM Project19) and were positioned with the devices axis in parallel to muscle fibers.7,9 To locate the center of the muscle belly, participants seated on a chair and the center of the muscle was considered as the 1/3 of the distance between the head of the fibula and the tip of the medial malleolus.19 The center of the vibratory devices was positioned directly on the target spots. Extra care was taken to ensure that both vibratory devices were exclusively on the tibialis anterior muscle. For better fixation, ordinary elastic bands were used. A 100Hz vibration frequency was used to determine the vibration effects on the CoP dependent variables, since this frequency is successful to induce postural adaptations.7
The Statistica 7.0 (StatSoft®) software for Windows was used for statistical procedures and significant results were considered when p<0.05. Munro's classification for reliability coefficients was used to describe the degree of reliability: 0.26–0.49 reflects low correlation; 0.5–0.69 moderate correlation; 0.7–0.89 high correlation; 0.9–1.00 very high correlation.20 Student t-test for dependent variables was used to assess the difference in CoP behavior between the close-to-last five seconds without vibration and the close-to-last five seconds of vibration.
ResultsRCVibro System calibration and reliabilityFig. 2 shows the percentage of electrical potential difference/vibration frequency curves achieved for one vibratory device on Test, Re-Test 1, Re-Test 2 and Re-Test D2. The curves show a linear increase of vibration frequency with higher percentages of electrical potential differences. A similar pattern was observed for all devices. The vibration amplitude ranged between 0.7 and 1.2mm for different devices.
Table 1 presents the variability (CV), the ICC(2,6), its 95% Confidence Interval, the SEM and also the MDC results for each vibratory device in both X and Z directions. It can be noticed an extremely low variability in the vibration frequency within the five seconds testing period (CV<2.03%). All devices showed a very high level of agreement between the vibration frequencies achieved within the same day (ICC(2,6) ranging from 0.95 to 0.99) and between different days (ICC(2,6) ranging from 0.81 to 0.98) with some exceptions, such as in the device #3 (ICC(2,6), ranging from 0.63 to 0.71), discussed further. The complete results per device can be consulted in Table 2.
Variability and ICC (95% interval of confidence) for each vibratory device.
| Device | CV Test (%) | CV Re-Test 1 (%) | CV Re-Test 2 (%) | ICC(2,6) (95% CI) | F value | p value | SEM (Hz) | MDC (Hz) | CV Re-Test D2 (%) | ICC(2,6) (95% CI) | F value | p value | SEM (Hz) | MDC (Hz) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| #1 | ||||||||||||||
| X | 0.57 | 0.50 | 0.55 | 0.960 (0.996–0.998) | 45.30 | <0.01 | 6.60 | 18.29 | 0.41 | 0.963 (0.928–0.978) | 24.65 | <0.001 | 7.52 | 20.85 |
| Z | 0.56 | 0.49 | 0.57 | 0.960 (0.959–0.987) | 45.30 | <0.01 | 6.60 | 18.28 | 0.41 | 0.963 (0.928–0.978) | 24.67 | <0.001 | 7.52 | 20.85 |
| #2 | ||||||||||||||
| X | 0.35 | 0.39 | 0.40 | 0.986 (0.973–0.992) | 69.87 | <0.01 | 4.32 | 11.96 | 0.40 | 0.881 (0.968–0.995) | 56.34 | <0.001 | 3.35 | 9.28 |
| Z | 0.37 | 0.39 | 0.40 | 0.986 (0.973–0.992) | 69.91 | <0.01 | 4.32 | 11.96 | 0.40 | 0.997 (0.992–0.997) | 318.20 | <0.001 | 1.42 | 9.93 |
| #3 | ||||||||||||||
| X | 2.03 | 0.95 | 0.56 | 0.712 (0.784–0.929) | 7.75 | <0.01 | 4.32 | 11.96 | 0.56 | 0.635 (0.495–0.804) | 3.01 | 0.004 | 9.28 | 25.72 |
| Z | 2.03 | 0.95 | 0.57 | 0.712 (0.783–0.928) | 7.74 | <0.01 | 4.70 | 13.02 | 0.57 | 0.634 (0.494–0.803) | 3.01 | 0.004 | 9.28 | 25.74 |
| #4 | ||||||||||||||
| X | 0.80 | 0.96 | 0.95 | 0.994 (0.991–0.997) | 216.40 | <0.01 | 2.96 | 8.20 | 1.01 | 0.959 (0.954–0.986) | 39.02 | <0.001 | 5.57 | 15.43 |
| Z | 0.81 | 0.95 | 0.96 | 0.994 (0.991–0.997) | 217.80 | <0.01 | 2.95 | 8.18 | 1.01 | 0.959 (0.954–0.986) | 39.28 | <0.001 | 5.55 | 15.39 |
| #5 | ||||||||||||||
| X | 0.74 | 0.77 | 0.64 | 0.953 (0.925–0.977) | 23.53 | <0.01 | 4.65 | 12.89 | 0.78 | 0.812 (0.674–0.886) | 4.97 | 0.009 | 9.56 | 26.49 |
| Z | 0.74 | 0.77 | 0.63 | 0.953 (0.925–0.977) | 23.50 | <0.01 | 4.65 | 12.90 | 0.78 | 0.812 (0.675–0.886) | 4.97 | 0.009 | 9.55 | 26.48 |
| #6 | ||||||||||||||
| X | 0.30 | 0.38 | 0.37 | 0.993 (0.991–0.997) | 211.30 | <0.01 | 2.51 | 6.97 | 0.38 | 0.982 (0.966–0.989) | 53.85 | <0.001 | 3.98 | 11.03 |
| Z | 0.30 | 0.38 | 0.37 | 0.993 (0.991–0.997) | 213.60 | <0.01 | 2.50 | 6.93 | 0.38 | 0.982 (0.966–0.989) | 54.12 | <0.001 | 3.97 | 11.00 |
CV, coefficient of variation; SEM, standard error of measurement; MDC, minimal detectable change.
Vibration frequency per device, electric potential difference and test.
| X | Z | |||||||
|---|---|---|---|---|---|---|---|---|
| Test | Re-Test 1 | Re-Test 2 | Re-Test D2 | Test | Re-Test 1 | Re-Test 2 | Re-Test D2 | |
| Device #1 | ||||||||
| 14% | 128.32 | 120.08 | 117.15 | 113.43 | 128.32 | 120.08 | 117.15 | 113.43 |
| 21% | 136.75 | 127.11 | 124.45 | 113.36 | 128.21 | 119.90 | 117.02 | 113.36 |
| 28% | 142.62 | 138.85 | 135.97 | 127.16 | 142.18 | 139.68 | 136.08 | 127.16 |
| 35% | 144.61 | 143.23 | 139.52 | 135.14 | 144.84 | 143.67 | 139.85 | 135.14 |
| 42% | 146.05 | 145.94 | 141.40 | 140.85 | 146.05 | 145.94 | 141.40 | 140.85 |
| 49% | 151.04 | 155.25 | 148.27 | 158.36 | 151.04 | 155.25 | 148.27 | 158.36 |
| 56% | 157.80 | 176.20 | 159.02 | 173.87 | 157.80 | 176.20 | 159.13 | 173.87 |
| 63% | 168.33 | 189.61 | 163.56 | 179.96 | 168.33 | 189.61 | 163.56 | 179.96 |
| 70% | 180.52 | 199.14 | 170.55 | 186.17 | 180.52 | 199.02 | 170.43 | 186.17 |
| 77% | 189.94 | 200.35 | 178.19 | 191.05 | 189.94 | 200.35 | 178.19 | 191.05 |
| 84% | 195.59 | 197.25 | 185.95 | 195.59 | 195.70 | 197.25 | 185.84 | 195.59 |
| Device #2 | ||||||||
| 14% | 99.73 | 98.63 | 95.30 | 96.52 | 99.73 | 98.52 | 95.30 | 96.52 |
| 21% | 112.59 | 109.26 | 104.17 | 110.93 | 112.59 | 109.26 | 104.17 | 110.93 |
| 28% | 118.35 | 115.36 | 110.04 | 120.12 | 118.35 | 115.36 | 110.04 | 120.12 |
| 35% | 123.78 | 120.01 | 115.03 | 126.11 | 123.78 | 120.01 | 115.03 | 126.11 |
| 42% | 128.66 | 124.78 | 121.12 | 130.10 | 128.66 | 124.78 | 121.12 | 130.10 |
| 49% | 133.64 | 131.98 | 128.99 | 133.87 | 133.64 | 131.98 | 128.99 | 133.87 |
| 56% | 138.85 | 138.52 | 136.08 | 138.30 | 138.96 | 138.52 | 136.08 | 138.30 |
| 63% | 144.84 | 144.39 | 143.73 | 144.50 | 144.73 | 144.28 | 143.73 | 144.50 |
| 70% | 148.38 | 148.60 | 155.03 | 149.38 | 148.38 | 148.60 | 155.03 | 149.38 |
| 77% | 150.38 | 153.70 | 163.67 | 151.93 | 150.38 | 153.70 | 163.67 | 151.93 |
| 84% | 157.47 | 163.34 | 170.88 | 153.92 | 157.47 | 163.34 | 170.88 | 153.92 |
| Device #3 | ||||||||
| 14% | 141.95 | 141.29 | 129.99 | 130.65 | 141.95 | 141.29 | 129.88 | 130.65 |
| 21% | 146.17 | 149.60 | 139.18 | 138.74 | 146.17 | 149.60 | 139.18 | 138.74 |
| 28% | 151.82 | 153.92 | 143.95 | 141.18 | 151.82 | 153.92 | 143.95 | 141.18 |
| 35% | 155.92 | 156.36 | 136.97 | 139.85 | 155.92 | 156.47 | 136.97 | 139.85 |
| 42% | 160.90 | 158.24 | 138.96 | 141.40 | 160.90 | 158.24 | 138.96 | 141.40 |
| 49% | 164.89 | 159.35 | 143.73 | 145.83 | 164.89 | 159.35 | 143.73 | 145.83 |
| 56% | 166.22 | 162.34 | 147.94 | 150.93 | 166.22 | 162.34 | 147.94 | 150.82 |
| 63% | 165.45 | 159.24 | 154.03 | 155.36 | 165.45 | 159.24 | 154.03 | 155.36 |
| 70% | 166.78 | 158.47 | 154.81 | 172.87 | 166.78 | 158.47 | 154.81 | 172.87 |
| 77% | 163.34 | 158.58 | 160.35 | 175.53 | 163.34 | 158.58 | 160.35 | 175.53 |
| 84% | 158.91 | 161.68 | 162.12 | 178.19 | 158.91 | 161.68 | 162.12 | 178.19 |
| Device #4 | ||||||||
| 14% | 60.84 | 61.61 | 65.71 | 72.25 | 60.84 | 61.61 | 65.60 | 72.14 |
| 21% | 81.56 | 86.77 | 88.98 | 85.11 | 81.56 | 86.77 | 88.98 | 85.11 |
| 28% | 99.18 | 95.41 | 102.84 | 92.20 | 99.18 | 95.41 | 102.84 | 92.20 |
| 35% | 113.92 | 106.38 | 112.81 | 95.52 | 113.92 | 106.38 | 112.81 | 95.52 |
| 42% | 123.23 | 116.25 | 119.57 | 113.70 | 123.23 | 116.25 | 119.57 | 113.70 |
| 49% | 129.21 | 124.45 | 123.89 | 119.02 | 129.21 | 124.45 | 123.89 | 119.02 |
| 56% | 132.98 | 130.54 | 128.77 | 126.00 | 132.98 | 130.54 | 128.77 | 126.00 |
| 63% | 139.41 | 132.76 | 131.65 | 128.77 | 139.41 | 132.76 | 131.65 | 128.77 |
| 70% | 138.52 | 137.19 | 134.53 | 132.76 | 138.41 | 137.08 | 134.53 | 132.76 |
| 77% | 143.73 | 139.07 | 136.41 | 134.20 | 143.73 | 139.07 | 136.41 | 134.20 |
| 84% | 143.06 | 139.07 | 139.18 | 133.98 | 143.06 | 139.07 | 139.18 | 133.98 |
| Device #5 | ||||||||
| 14% | 122.23 | 127.33 | 125.00 | 125.89 | 122.23 | 127.33 | 125.00 | 125.89 |
| 21% | 137.97 | 142.29 | 139.30 | 139.07 | 137.97 | 142.29 | 139.30 | 139.07 |
| 28% | 149.93 | 151.15 | 150.04 | 145.94 | 149.93 | 151.15 | 150.16 | 145.94 |
| 35% | 157.25 | 158.69 | 154.37 | 149.49 | 157.25 | 158.69 | 154.37 | 149.49 |
| 42% | 162.57 | 158.13 | 156.14 | 150.82 | 162.57 | 158.13 | 156.14 | 150.82 |
| 49% | 170.21 | 157.36 | 156.14 | 153.37 | 170.21 | 157.36 | 156.14 | 153.37 |
| 56% | 168.44 | 160.24 | 157.80 | 154.48 | 168.44 | 160.24 | 157.80 | 154.48 |
| 63% | 169.44 | 160.24 | 159.13 | 158.02 | 169.44 | 160.24 | 159.13 | 158.02 |
| 70% | 166.00 | 160.90 | 159.46 | 169.88 | 166.00 | 160.90 | 159.46 | 169.77 |
| 77% | 161.79 | 165.67 | 162.57 | 180.96 | 161.79 | 165.67 | 162.57 | 180.96 |
| 84% | 162.90 | 181.63 | 168.00 | 187.83 | 162.90 | 181.63 | 168.00 | 187.83 |
| Device #6 | ||||||||
| 14% | 97.74 | 103.61 | 104.39 | 104.39 | 97.74 | 103.61 | 104.39 | 104.39 |
| 21% | 114.58 | 121.79 | 123.45 | 122.23 | 114.69 | 121.79 | 123.45 | 122.23 |
| 28% | 127.11 | 134.53 | 136.19 | 133.64 | 127.11 | 134.53 | 136.19 | 133.64 |
| 35% | 138.08 | 144.28 | 145.06 | 141.18 | 138.08 | 144.28 | 145.06 | 141.18 |
| 42% | 146.39 | 151.71 | 151.60 | 146.72 | 146.39 | 151.71 | 151.60 | 146.72 |
| 49% | 153.48 | 156.91 | 155.59 | 151.26 | 153.48 | 156.91 | 155.59 | 151.26 |
| 56% | 158.36 | 159.80 | 157.91 | 153.81 | 158.36 | 159.80 | 157.91 | 153.81 |
| 63% | 161.02 | 162.57 | 160.13 | 155.25 | 161.02 | 162.57 | 160.13 | 155.25 |
| 70% | 163.90 | 164.45 | 161.13 | 157.69 | 163.90 | 164.45 | 161.13 | 157.69 |
| 77% | 166.33 | 165.56 | 162.12 | 159.80 | 166.33 | 165.56 | 162.23 | 159.80 |
| 84% | 168.88 | 170.77 | 166.22 | 163.90 | 168.88 | 170.77 | 166.22 | 163.90 |
The CoP position behavior of one participant during one trial with and without vibration is shown in Fig. 3. It can be observed a forward CoP displacement after the vibration onset. On the other hand, Fig. 3 shows a CoP position maintenance without the use of vibration. The Student t-test results confirmed this observation, showing a mean of 1.10cm forward CoP displacement with vibration (OFF: −0.77±0.62cm and ON: 0.32±0.67cm; t(14)=3.34, p<0.01; effect size: 1.41; power: 0.999). Furthermore, vibration increased the CoP mean velocity (OFF: 1.21±0.30cm/s and ON: 1.46±0.46cm/s; t(14)=2.27, p<0.01; effect size: 0.40; power: 0.40). None influence of vibration was observed for CoP area (OFF: 1.20±0.91cm2 and ON: 1.41±1.04cm2; t(14)=1.16; p=0.26).
Discussion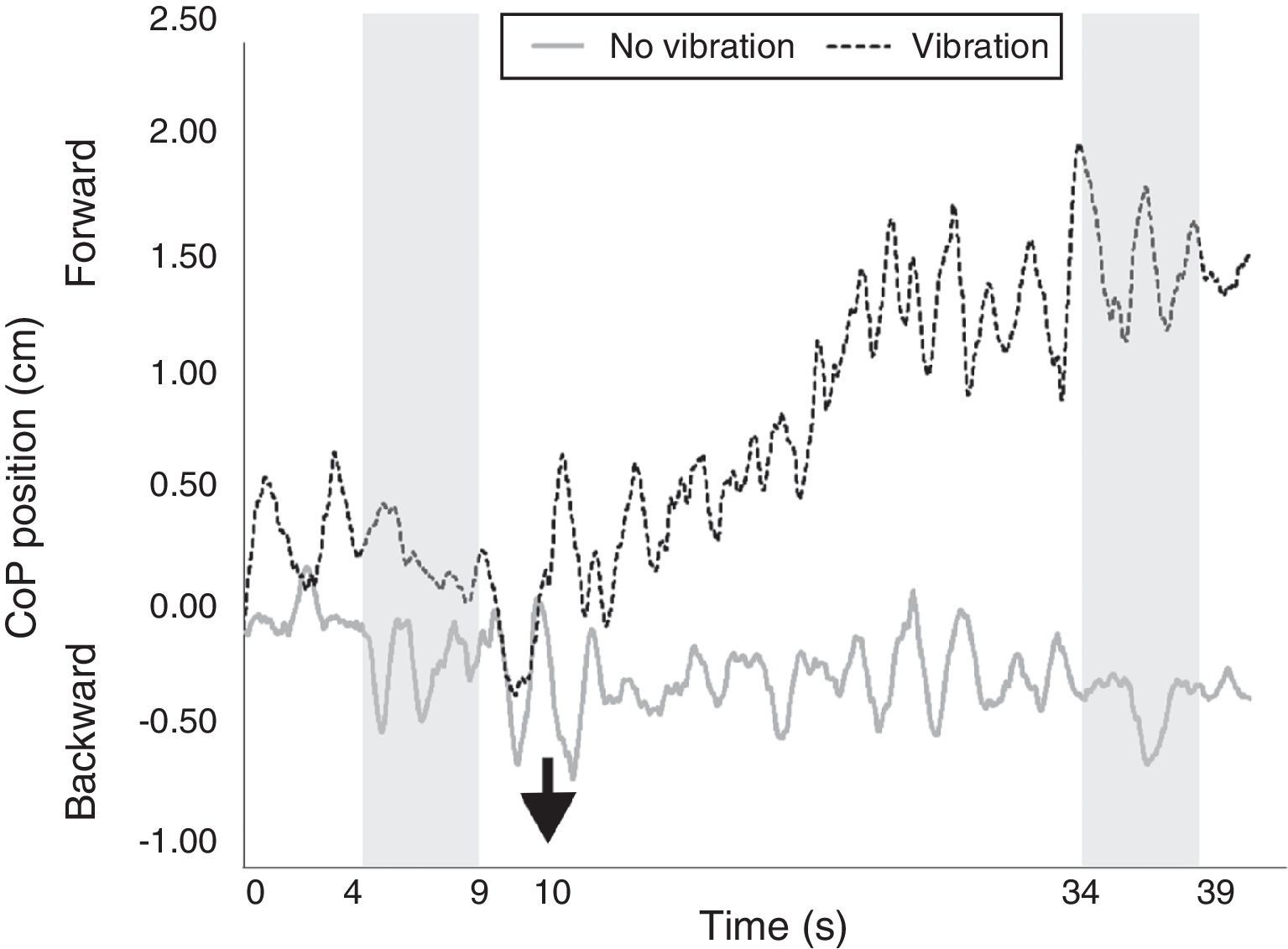
The aim of this study was to describe the technical details and the reliability and functionality of a custom-made system designed to apply muscle vibration. It was shown that the RCVibro System is a highly reliable system and can replicate previous observations.
RCVibro System is one of the first vibratory systems to have its technical aspects and reliability fully demonstrated. The system reliability is extremely important, since different vibration frequencies can lead to diverse motor effects.9 Therefore, a reliable system guarantees that the same frequency is being applied for all participants across all trials and conditions. We demonstrated that the RCVibro System is a high reliable system, with the exception of one device – that showed a moderate level of agreement (device #3). The reason for the low level of agreement for device #3 can be linked to the higher variability observed in Test (2.03%). It is important to bring it out that Test was used to assess the device reliability within the same day and between different days. Hence, a new series of ICC(2,6) tests was conducted for device #3 considering both Re-Test 1 and Re-Test 2 (for reliability within the same day) and also Re-Test 1 and Re-Test D2 (for reliability between different days). As result, very high agreement levels were found (within the same day: ICC(2,6)=0.92, F=13.89 and p<0.01; between days: ICC(2,6)=0.95, F=23.50 and p<0.01). One possible source of variability observed for device #3 during Test could be related to a small IRED movement, resulting in higher variability. We do not believe in other sources of variability, since during all posterior assessments very low (and similar) variability were recorded. However, even with these results, it should be noted that regular actions have been taken to assure that sources of variability (especially with Device #3) would not be presented for other devices. For example, we have redone the procedures used here 5 times in different locations and using different optoelectronic systems (data not published); in addition, the devices are regularly checked for malfunctioning. In all cases, the variability observed during Test in device #3 was not observed again for any devices. Nevertheless, this issue seemed to be solved.
The MDC results reinforce the reliability of our system: all changes in vibration frequencies observed within or between days could not be considered real changes, but are consistent with the measurement error. Additionally the statistical approach in this study allowed us to warrantee the correct reliability test for the RCVibro System. Herein we analyzed the absolute consistency considering scores of individuals (each device). Also, we used the SEM which is an indication of the precision of a score and its use allows to construct confidence intervals for each score (different devices).21 Another important feature of the RCVibro System is related to its wireless control configuration. This is an important issue, mainly in experimental environment where the participant should not be aware when the devices will be switched on. Additionally, this configuration allows the examiners to control the device online.
This study also demonstrated the RCVibro System potential clinical usage, since similar results observed by previous studies were replicated by this system. Previous studies have already demonstrated a forward CoP displacement8,9,22 when local vibration is applied on the tibialis anterior. Additionally, Capicikova et al.14 found an increase of CoP velocity (∼50%) when calf muscles were stimulated by local vibration, although none statistical significance was reached.14 Therefore, we can argue that RCVibro System induces corresponding postural effect that has already been reported by the literature, since an increase in CoP velocity and a forward CoP displacement were observed in this study.
However, two issues should be further discussed. We believe that the short period used to analyze the CoP behavior (5s) could explain the lack of statistical significance for area.7 This is a study limitation and future research should consider longer periods to analyze the CoP behavior. Moreover, shorter CoP A-P displacements were observed in comparison to previous findings. Among previous studies that had vibratory-stimulated the tibialis anterior, Courtine et al.8 found a ∼4cm forward CoP displacement and Ivanenko et al.22 found a displacement ∼4.9cm. Clearly, the results of the current study indicate a slighter CoP forward displacement (1.10cm). This could be due to the higher vibration frequency used here to elicit the postural effects: we used 100Hz, a difference of 20Hz in comparison to Courtine et al.8 and Ivanenko et al.22 studies – 80Hz. Physiological studies have already showed that vibration frequencies higher than 100–120Hz could induce muscle spindles to discharge in subharmonic frequencies,23 reducing the effectiveness of local vibration.24 This could be the reason for lower vibration effects observed here. However, in the study of Polonyova et al.9 greater body displacements were found whilst the tibialis anterior was stimulated by higher vibration frequencies (100Hz vs 80Hz).9 Hence, the reasons for the slighter influence of tibialis anterior vibration on CoP displacement found by this study has not been completely understood; we suggest that the influence of different vibration frequencies in postural adjustments should be further investigated by future research.
Further, other three study limitations should be considered: (i) investigating the ICC values into every frequency for each device (i.e. considering the six 0.5-s periods) would assure that the same frequency is being applied between different occasions for every electrical potential difference. However, this analysis would not be feasible. ICC is dependent on between-subjects variability and the number of subjects assessed.21 Hence, since for this analysis a low number of repetitions would be used (six 0.5s periods) with a very low variability among them, assessing the ICC into every vibration frequency would not be feasible; (ii) a larger variability between days was observed when the devices worked close to the their electric potential difference limit. This behavior was not unexpected since the fabricant advices that devices cannot work properly close their limit. Therefore, we recommend the devices usage until 70% of their capacity in order to avoid any overload; (iii) we assessed the RCVibro System functionality only in healthy young adults. However, our system was developed mainly to be used in disable individuals. Hence, its functionality in individuals with motor impairments should be further explored. Despite this issue, our group have already shown the potential usage of the RCVibro System in clinical day-life: healthy young people and people with Parkinson's disease showed faster gait initiation with the use of muscle vibration.25,26 In addition, people with Parkinson's disease exhibiting freezing of gait presented a reduction of motor blocks severity using the RCVibro System.5 Finally, the RCVibro System was used to demonstrate the role of proprioception on the performance of sit-to-walk in healthy young individuals.27
In conclusion, this paper fully described a custom-made vibratory system. The full description of this system as demonstrated here is important to base future researchers and clinicians whom aim to use this technique as an alternative rehabilitation strategy for motor impaired people. This study also demonstrated that the RCVibro System is highly reliable and is able to replicate previous researches findings.
Conflicts of interestThe authors declare no conflicts of interest.
The authors thank Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) [Grant number: 2010/50532-0] and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) [Grant number: BEX 2194/15-5] for PhD scholarships.



