








Prevalence of knee osteoarthritis in former athletes is still unclear.
ObjectiveTo investigate prevalence of knee osteoarthritis in former athletes. Moreover, the secondary aim was to investigate whether poor methodological quality of included studies, different diagnosis criteria for knee osteoarthritis, different sports modality or sex impact on overall estimated prevalence of knee osteoarthritis in former athletes.
MethodsSearches on MEDLINE, EMBASE, AMED, SPORTDiscus and CINAHL from the earliest record to February 2018 and hand-searching identified studies investigating prevalence of knee osteoarthritis in former athletes. Meta-analysis was conducted and the GRADE system summarized strength of the current recommendations. Sensitivity analyses investigated whether methodological quality, diagnostic criteria, type of sports or sex impacted on the overall estimated prevalence in former athletes. This review was registered at PROSPERO (CRD42016050903).
ResultsFifteen studies were included and pooling of 3100 participants estimated overall prevalence of knee osteoarthritis in former athletes of 30.0% (95% CI: 20.0 to 40.0%). The strength of the current recommendations was low-quality. Sensitivity analyses suggested that different diagnostic criteria for knee osteoarthritis and type of sports may impact on the overall estimated prevalence.
ConclusionsPrevalence of knee osteoarthritis in former athletes was 30.0%. Researchers, clinicians and policymakers should be careful about potential prevalence differences among type of sports and diagnostic criteria. Current low-quality evidence shows that future high-quality studies are likely to impact on the estimated prevalence.
Osteoarthritis (OA) is a degenerative disease characterized by loss and degradation of articular cartilage in addition to synovial inflammation, leading to joint stiffness, swelling, pain and loss of mobility.1 It is influenced by genetic and epigenetic factors,2,3 sex,4 ethnicity,5 age,1 obesity,4,6 sedentary lifestyle7 and joint injuries.1 For example, obesity increases joint loading1,4,6 and inflamatory mediators,1 which helps to explain its relationship with OA. In addition, sedentary lifestly increases the risk of having metabolic syndrome, type 2 diabetes and insulin resistance, which are also related to the development of the disease.8 According to epidemiological studies, the knee is the most frequently affected joint by OA, with prevalence ranging from 164 to 250 cases per 100,000 in the general population.9,10 This may be explained by the higher knee vulnerability to direct (knocked) and indirect (twisted) trauma,11 along with the high load supported by this joint.
Sports participation might be beneficial for knee joint cartilage and consequently protect against the occurrence of knee OA in former athletes. Jones et al.12 demonstrated that children who participated in more vigorous sports gained twice as much tibial articular cartilage as those who participated in less active sports, suggesting that articular cartilage positively responds to increased loads. Although studies with adults did not demonstrate effects of sports participation in cartilage thickness,13 most athletes start participating in sports in childhood or adolescence,14 which may act as a protective factor for knee OA later in life. It should be noted that sports participation also reduces body fat mass,15 a known risk factor for OA,9 prevents the loss of cartilage proteoglicans,16,17 which are responsible for cartilage's viscoelastic properties,18 and increases muscle mass and strength,19,20 which might reduce loading on joint passive components (e.g. cartilage).
On the other hand, athletes are under high physical demands during many years, which increases their susceptibility to knee joint injuries.21,22 Chen et al.21 demonstrated that the knee was the joint most frequently affected by sports injuries, with 58.8% of athletes having some type of knee injury. This may occur because the knee is particularly vulnerable to direct and indirect trauma.11 Knee injuries produce a local inflammation associated with degradation of the articular cartilage.23,24 Moreover, athletes are more frequently submitted to knee surgeries25–30 and often become overweight after retirement, which are also risk factors for knee OA.31 Therefore, considering that the knee injuries are common in athletes, former athletes might actually have a high prevalence of knee OA.
Previous reviews32–35 on this topic did not focus on knee OA35 prevalence or presented important limitations, and thus, prevalence of knee OA in former athletes is still unclear. For instance, they restricted date of publication32–34 and language32–34 of included studies. The primary aim of this systematic review with meta-analysis was to investigate the prevalence of knee OA in former athletes. The secondary aim was to investigate whether poor methodological quality of included studies, different diagnosis criteria, type of sport or sex impact on overall estimated prevalence of knee OA in former athletes. We hypothesized that former athletes would present high prevalence of knee OA, and that methodological quality of included studies, different diagnosis criteria, type of sport and sex would influence on this prevalence. Knee OA causes disability and consequently increases health care costs.36 Therefore, the results of this systematic review may help to improve understanding about the relationship between sports practice and knee OA prevalence and also provide sports organizations and health care systems important data on a highly prevalent health condition in the general population.
MethodsThe protocol of this review was prospectively registered at PROSPERO (CRD42016050903) and methods followed recommendations from the Joanna Briggs Institute Reviewers’ Manual (The Systematic Review of Prevalence and Incidence Data),37 the Cochrane Collaboration38 and PRISMA reporting guidelines.39
Searches and inclusion criteriaElectronic searches were conducted on MEDLINE (via Ovid), EMBASE, AMED, SPORTDiscus and CINAHL from the earliest record to February 2018, without language restriction. In addition, we hand-searched identified reviews in the field. Hand-searching was performed trough the reading of the entire list of references of all identified systematic reviews related to the topic of our study. Detailed search strategy using descriptors related to “prevalence”, “former athletes” and “osteoarthritis” is presented in Appendix 1.
All published studies that investigated prevalence of knee OA in former athletes were considered in this review. To be included, studies had to investigate participants with knee OA based on at least one of the following diagnosis criteria: (a) imaging; (b) clinical examination; and/or (c) self-reported. Due to inconsistency in how former athletes are named in the literature, we included studies in which at least one of the following descriptors was used by the authors as their included sample of former athletes: “former athletes”; “ex-athletes”; “former elite athletes”; “master athletes”; and “retired athletes”.
Study selectionTwo independent reviewers (BAS and FOM) screened titles and abstracts, and assessed potential full-texts. We included potential full-texts fulfilling eligibility criteria described in previous section. Between-reviewer agreement was tested through Kappa statistics, showing a moderate agreement (k=0.7, p<0.001). Between-reviewer disagreements were solved by a third reviewer (RAR).
Data extraction and study ratingTwo independent reviewers extracted data (BAS and FOM), and disagreements were solved by consulting a third reviewer (RAR). Extracted data included study design, setting, study population, OA definition, diagnostic criteria and prevalence of knee OA. For prevalence, we extracted percentage and/or number of knee OA cases. As most of the studies did not clearly state in which of the knee joints the OA prevalence was investigated (i.e. tibiofemoral, patellofemoral or both joints), we decided to report prevalence of OA in both joints altogether. In addition, when studies reported prevalence of OA in different knee joints (i.e. tibiofemoral or patellofemoral joints), different lower limb sides, or using different diagnostic criteria, the higher prevalence data were computed and reported. Finally, when studies reported prevalence in different sport modalities, we computed and reported the general prevalence for that study.
Two independent reviewers (BAS and FOM) also assessed risk of bias for each included study using “The Joanna Briggs Institute Prevalence Critical Appraisal Tool”.37 Each item was rated as ‘yes’, ‘no’ or ‘unclear’ according to information available in each study, with a maximum score of 10 points. To evaluate if sample size of each included study was appropriate, we used the following equation:
where p was the expected prevalence (19.0%), defined based on a previous study,40Z was the confidence level (1.96) and d was the precision (5.0%).41 Sample size estimation resulted in an appropriate sample size of 236 participants. A third reviewer (RAR) solved potential disagreements regarding risk of bias scoring.Data analysis
Descriptive statistics were used to summarize data. I2 statistics was used to assess among-study heterogeneity and pooling estimated prevalence of knee OA in former athletes, following the Cochrane recommendations.38 For pooling, fixed-effects model was used when I2<50.0% and random-effects model was used when I2≥50.0%.38 Findings from pooling and individual studies were presented in forest plots with 95% Confidence Interval (CI).
The GRADE (Grading of Recommendations Assessment, Development and Evaluation) system was used to summarize the overall quality of the evidence.42 The four levels of the GRADE system range from high-quality evidence, in which further research is very unlikely to change the estimate of prevalence, to very low-quality evidence, in which the estimate of prevalence is very uncertain.42 Scoring of evidence started at high-quality evidence, which was downgraded one level if one of the following pre-specified criteria was present: (i) poor methodological quality (average risk of bias ≤5 points out of 1043); (ii) imprecision (when ≥50.0% of the analyzed studies did not present appropriate sample size – minimum of 236 participants); (iii) indirectness (when ≥50.0% of the studies did not report reliability of the diagnostic criteria for knee OA); and (iv) inconsistency (if I2≥50.0%). Two independent reviewers (BAS and FOM) assessed quality of the evidence. Kappa statistics showed a perfect between-reviewer agreement between raters for GRADE assessment (k=1.00, p<0.046).
Sensitivity analysis investigated whether poor methodological quality of included studies, different diagnosis criteria for knee OA, different type of sports and sex may impact on overall estimated prevalence of knee OA in former athletes. For methodological quality, we removed studies with methodological quality ≤5 out of 10. For diagnostic criteria, we pooled data for imaging, clinical examination and self-reported separately. For type of sports, we pooled data for different types of sports separately. For sex, we removed studies with female samples. All analyses were performed using Comprehensive Meta-Analysis, version 2.2.04 (Biostat, Inc.©, Englewood, New Jersey).
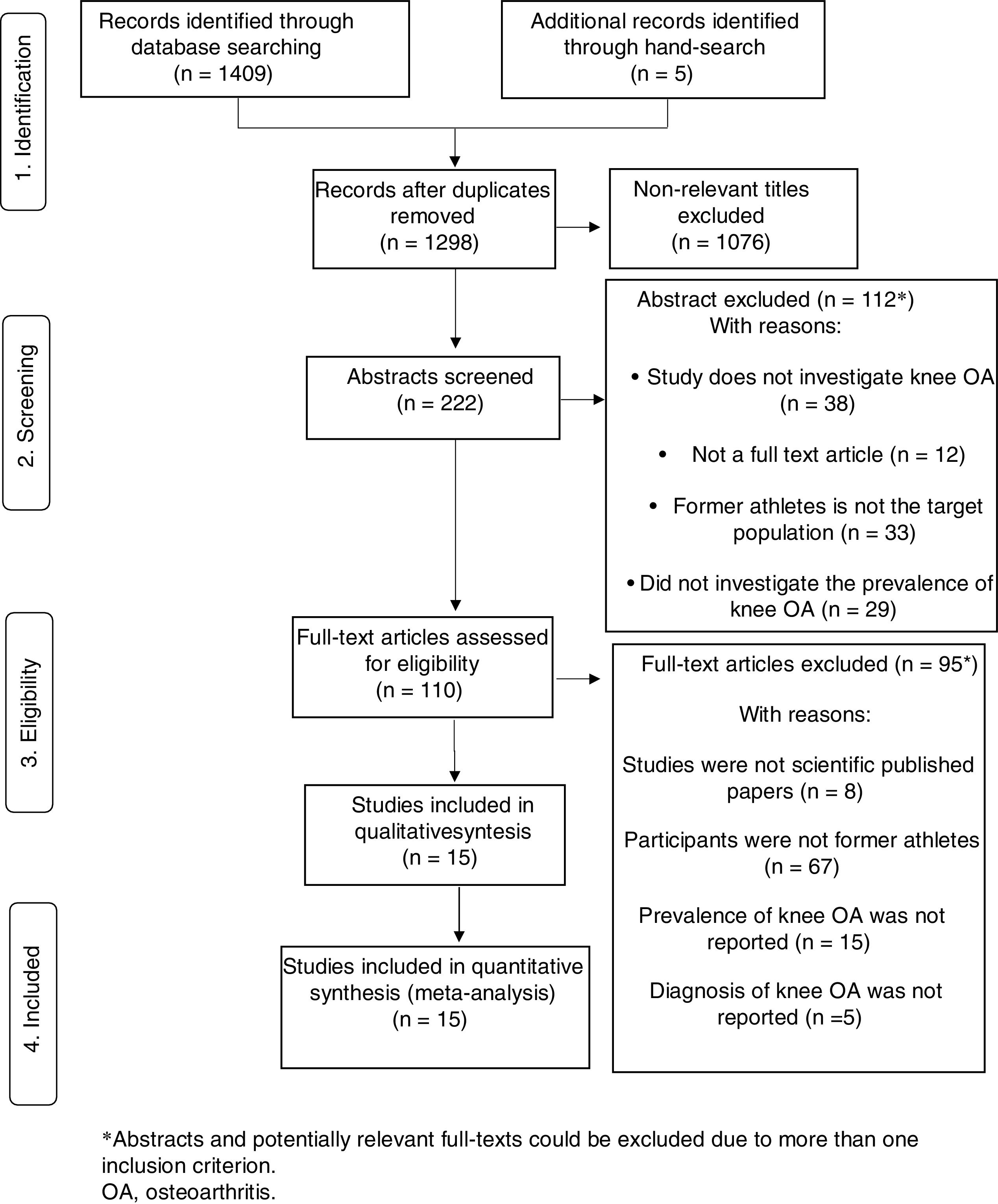
ResultsCharacteristics of the included studiesSearches retrieved 1409 titles and, after initial screening, we selected 110 potential full-texts. After evaluation of the 110 potential full-texts, 15 original studies were included in the review. Included studies were from the years of 1980 to 2016. Reasons for exclusion of potential full-texts were: not published study (n=8); participants were not former athletes (n=67); prevalence was not investigated (n=15); or diagnosis of knee OA was not reported (n=5) (Fig. 1).
Participants of all studies were male, except for one study.44 Ten out of fifteen included studies were cross-sectional,45–54 four were cohort44,55–57 and one was a case-control study.58 For diagnostic criteria, ten out of fifteen studies used imaging44–46,48–50,53–55,58 (i.e. Ultrasound,49 X-ray30–32,34,36,39–41,45 and/or Magnetic Resonance Imaging45), five used clinical exams46,53,55,56,58 and three used self-reported.51,52,57 Three reported prevalence in different sport modalities33,41,42 (Table 1).
Characteristics of the included studies (n=15).
| Study, year | Design | Setting | Study Population | OA definition and measurement | Prevalence |
|---|---|---|---|---|---|
| Arliani et al.,45 2014 | Cross-sectional study | Location: N/A Sample selection: Expedience | n*=27 Average age: 45.6 (5.9) years Gender: Male Sport: Soccer (football) Practice duration: Sports career that lasted at least 5 years | Bilateral knee radiography and magnetic resonance imaging | Knee OA*: Not reported OA in dominant knee*: (18)** 66.6% OA in non-dominant knee*: (18)** 66.6% |
| Drawer and Fuller,51 2001 | Cross-sectional study | Location: England Sample selection: Expedience | n*=185 Average age: 47.6 (13.2) years Gender: Male Sport: Soccer (football) Practice duration: Not reported | Self-administered postal questionnaire based on established published knowledge and criteria for assessing the causes, presence and severity of OA | Knee OA*: Not reported Right knee OA*: (35)** 19.0% Left knee OA*: (39)** 21.3% |
| Elleuch et al.,46 2008 | Cross-sectional study | Location: Tunisia Sample selection: Expedience | n*=50 Average age: 49.2 (3.8) years Gender: Male Sport: Soccer (football) Practice duration: Sports career that lasted at least 10 years | Radiological criteria and clinical examination | Knee OA*: (40)** 80.0% |
| Iosifidis et al.,58 2015 | Case-control study | Location: Greece Sample selection: Expedience | n*=218 (Soccer: 121, skiing: 42, volleyball: 17, martial arts: 16, track and field: 11, basketball: 11) Average age: 50.1 (8.5) years Gender: Male Sport: Soccer (football), skiing, volleyball, martial arts, basketball and track and field Practice duration: 15.3 (6.3) years | Radiological criteria classified according to the Kellgren and Lawrence classification scale, Clinical examination Questionnaire including items on physician-diagnosed knee OA (yes/no) | Clinical knee OA: (19)** 8.7% Soccer: (11)** 9.0%, Skiing: (4)** 9.5%, Volleyball: (1)** 5.8%, Marcial Arts: (1)** 6.2%, Track and Field: (1)** 9.1%, Basketball: (1)** 9.1% Radiographic knee OA: (34)** 19.76 Soccer: (20)** 16.5%, Skiing: (7)** 16.6%, Volleyball: (2)** 11.7%, Martial Arts: (1)** 6.2%, Track and Field: (1)** 9.0%, Basketball: (3)** 27.2% |
| Kettunen et al.,47 2001 | Cross-sectional study | Location: Finland Sample selection: Expedience | n*=867 (Endurance sport: 122, track and field: 212, team sport: 228, power sport: 253, shooting: 52) Average age: Endurance sport 68.8 (9.4), track and field sport 64.4 (9.3), team sport: 61.8 (8.3), power sport 64.5 (8.3), shooting 70.7 (10.8) Gender: Male Sport: Endurance sports (Long-distance running, Cross-country skiing), team sports (Soccer (football), Hockey, Basketball), track and field, power sports (Boxing, Wrestling, Weight lifting, Throwing) and shooting Practice duration: Not reported | Questionnaire in which respondents were asked whether they have ever been diagnosed by a physician before or after the age of 45 | Knee OA*: (230)** 26.5% Endurance: (31)** 25.4% Track and field: (49)** 23.1%, Team sport: (70)** 30.7%, Power sport: (69)** 27.3%, Shooting: (11)** 21.2% |
| Kettunen et al.,57 2006 | Cohort study | Location: Finland Sample selection: Expedience | n*=84 Average age: 58.3 (10.3) years Gender: Male Sport: Track and field Practice duration: Not reported | Health questionnaire | Knee OA*: (17)** 20.2% |
| Klunder et al.,53 1980 | Cross-sectional study | Location: Denmark Sample selection: Randomly | n*=30 Average age: 56.4 (range, 40–79) years Gender: Male Sport: Soccer (football) Practice duration: 22.8 (range 11–41 years) | Radiological criteria and clinical examination | Knee OA*: (8)** 26.7% |
| Krajnc et al.,48 2010 | Cross-sectional study | Location: Slovenia Sample selection: Expedience | n*=40 Average age: 49.2 (9.7) years Gender: Male Sport: Soccer (football) Practice duration: At least 3 years of involvement at the professional level | Radiological criteria classified according to the Kellgren and Lawrence classification scale | Knee OA*: Not reported Non-dominant leg: (23)** 57.5% Dominant leg: (17)** 42.5% |
| Kujala et al.,55 1995 | Cohort study | Location: Finland Sample selection: Expedience | n*=117 (long-distance runners: 28, soccer players: 31, weight lifters: 29, shooting: 29) Average age: 45–68 years Gender: Male Sport: Soccer (football), long distance running, weightlifting and shooting Practice duration: Not reported | Radiological criteria and clinical examination | Knee OA: (23)** 19.6% Shooting (1)** 3.0%, soccer players (9)** 29.0%, weight lifters (9)** 31.0% and long-distance runners (4)** 14.2% |
| Paxinos et al.,49 2016 | Cross-sectional study | Location: Greece Sample selection: Expedience | n*=100 Average age: 46.9 (5.9) years Gender: Male Sport: Soccer (football) Practice duration: 20.5 years | Ultrasound examination of the knee was performed according to published guidelines and bilateral knee radiography | Sonographic prevalence of knee OA*: (52)** 52.0% |
| Rajabi et al.,50 2012 | Cross-sectional study | Location: Iran Sample selection: Expedience | n*=22 Average age: 56.6 (5.17) years Gender: Male Sport: Table tennis Practice duration: At least 10 years of involvement at the professional level | Radiological criteria classified according to the Kellgren and Lawrence classification scale | Radiographic knee OA*: (12)** 54.5% |
| Roos et al.,54 1994 | Cross-sectional study | Location: Sweden Sample selection: Expedience | n*=286 Average age: 55.5 years Gender: Male Sport: Soccer (football) Practice duration: Not reported | Radiological criteria classified according to Ahlbäck | Knee OA*: (20)** 7.0% |
| Spector et al.,44 1996 | Cohort study | Location: United Kingdom, England Sample selection: Expedience | n*=81 (middle and long-distance runners: 67, tennis players: 14) Average age: 52.3 (6.1) years Gender: Female Sport: Running (middle and long distance) and tennis Practice duration: Not reported | Radiological criteria classified according to the Kellgren and Lawrence classification scale | Knee OA*: Not reported Knee at tibiofemoral joint: Osteophytes: (18)** 22.2%, Narrowing: (28)** 34.6%; Knee at patellofemoral joint: Osteophytes: (34)** 42.0%, Narrowing: (11)** 13.6% |
| Turner et al.,52 2000 | Cross-sectional study | Location: United Kingdom, England Sample selection: Expedience | n*=284 Average age: 56.1 (11.8) years Gender: Male Sport: Soccer (football) Practice duration: 13.5 (5.3) years in mean | Questionnaire: respondents were asked if they had been diagnosed with OA and at what age they were diagnosed | Knee OA*: Not reported Right knee: (82)** 28.9% Left knee: (62)** 21.8% |
| Tveit et al.,56 2012 | Cohort study | Location: Sweden Sample selection: Expedience | n*=709 (Impact sports: former soccer players: 397, handball players: 147, ice hockey players; Nonimpact sports: canoeists: 43, long-distance runners: 20, weight lifters: 9, gymnasts: 8, swimmers: 8, biathletes: 6, racing cyclists: 2) Average age: 70 (range, 50–93) years Gender: Male Sport: Soccer (football), handball, ice hockey, canoeing, long-distance running, weightlifting, gymnastics, swimming, athletics and cycling Practice duration: 20.5 years | Clinical examination | Knee OA*: (129)** 19.4% Nonimpact sports: (18)** 20.0%, Impact sports: (111)** 19.3% being that: Soccer: (67)** 18.2%, Handball: (30)** 15.8% and Ice hockey: (14)** 21.5% |
n, sample size; OA, osteoarthritis.
Mean methodological quality was 6.3 out of 10 (ranging from 4 to 9). Four studies out of fifteen scored ≤5 out of 10.46,47,51,57 Methodological quality issues are reported in Table 2. Out of fifteen studies, five did not analyze data with sufficient coverage of the identified sample,46,47,50,51,55 four did not use reliable diagnostic criteria for knee OA47,51,52,57 (i.e. self-reported diagnosis), eight did not present reliability of the method used to identify knee OA,46,47,49,51,52,54,56,57 twelve did not report subpopulations using objective criteria44–46,48–54,57,58 and eleven did not reach appropriate sample size.44–46,48–51,53,55,57,58
Methodological quality of the included studies (n=15).
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Overall score (0–10) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Arliani et al.,45 2014 | N | Y | N | Y | Y | Y | Y | Y | Y | N | 7 |
| Drawer and Fuller,51 2001 | N | Y | N | Y | U | N | N | Y | Y | N | 4 |
| Elleuch et al.,46 2008 | N | U | N | Y | U | Y | U | Y | Y | N | 4 |
| Iosifidis et al.,58 2015 | Y | U | N | Y | Y | Y | Y | Y | Y | N | 7 |
| Kettunen et al.,47 2001 | Y | N | Y | Y | U | N | N | U | Y | Y | 5 |
| Kettunen et al.,57 2006 | N | U | N | Y | Y | N | N | Y | Y | N | 4 |
| Klunder et al.,53 1980 | N | Y | N | Y | Y | Y | Y | Y | Y | N | 7 |
| Krajnc et al.,48 2010 | N | Y | N | Y | Y | Y | Y | Y | Y | N | 7 |
| Kujala et al.,55 1995 | Y | U | N | Y | U | Y | Y | Y | Y | Y | 7 |
| Paxinos et al.,49 2016 | N | Y | N | Y | Y | Y | U | Y | Y | N | 6 |
| Rajabi et al.,50 2012 | N | Y | N | Y | N | Y | Y | Y | Y | N | 6 |
| Roos et al.,54 1994 | N | Y | Y | Y | Y | Y | N | Y | Y | N | 7 |
| Spector et al.,44 1996 | Y | Y | N | Y | Y | Y | Y | Y | Y | N | 8 |
| Turner et al.,52 2000 | N | Y | Y | Y | Y | N | N | Y | Y | N | 6 |
| Tveit et al.,56 2012 | Y | Y | Y | Y | Y | Y | U | Y | Y | Y | 9 |
1. Was the sample representative of the target population?
2. Were study participants recruited in an appropriate way?
3. Was the sample size adequate?
4. Were the study subjects and the setting described in detail?
5. Was the data analysis conducted with sufficient coverage of the identified sample?
6. Were objective, standard criteria used for the measurement of the condition?
7. Was the condition measured reliably?
8. Was there appropriate statistical analysis?
9. Are all important confounding factors/subgroups/differences identified and accounted for?
10. Were subpopulations identified using objective criteria?
11. Y, yes; N, no; U, unclear; N/A, not applicable.
Pooling of 3100 participants from the 15 included studies estimated prevalence of knee OA (Fig. 2). According to the GRADE system used in the review, studies provided low-quality evidence that prevalence of knee OA in former athletes is 30.0% (95% CI: 20.0 to 40.0%). Evidence was downgraded from high- to low-quality because of imprecision (when ≥50.0% of the analyzed studies did not present appropriate sample size – minimum of 236 participants) and inconsistency (if I2≥50.0%).
Sensitivity analysis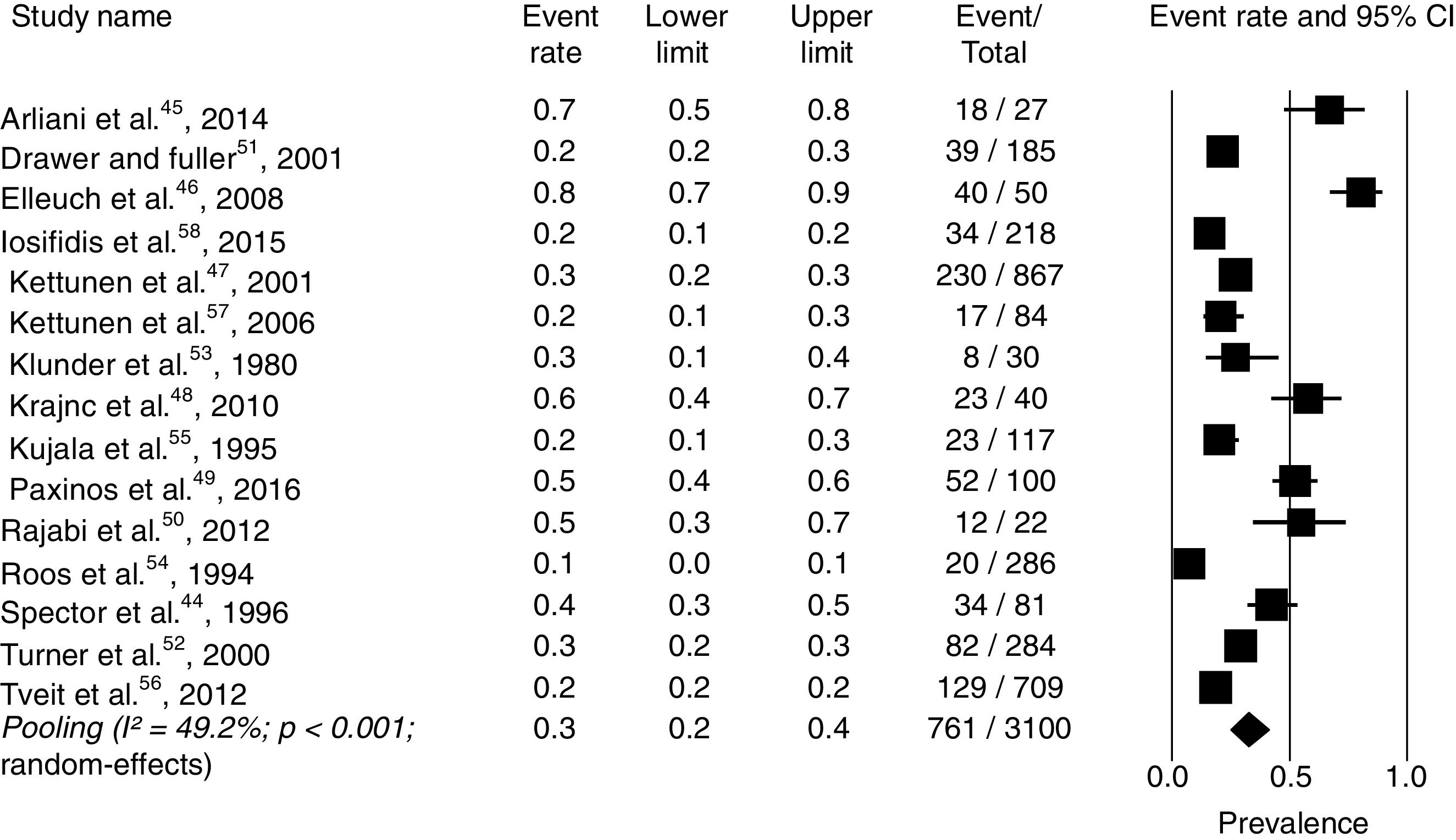
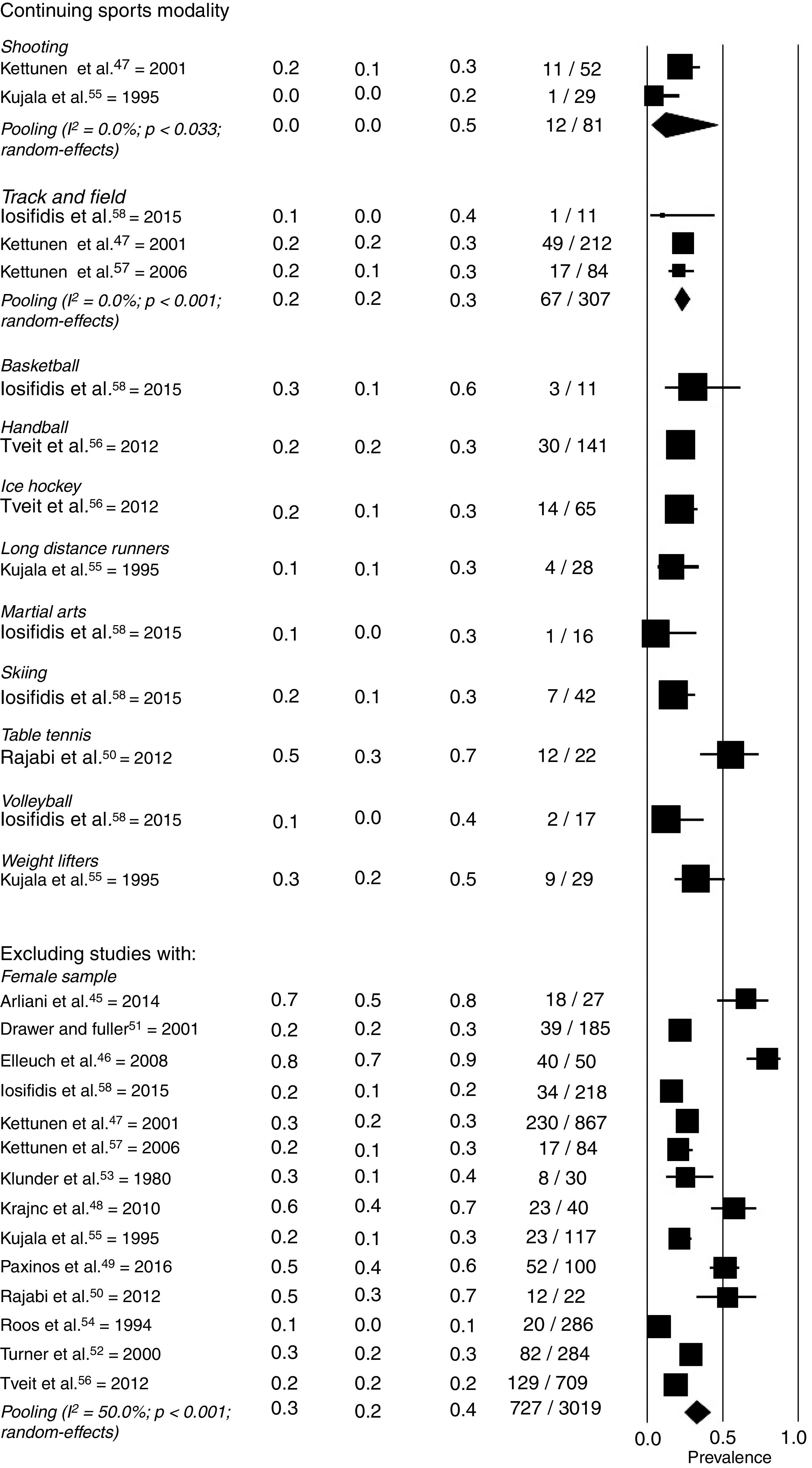
Sensitivity analyses showed that exclusion of studies with methodological quality ≤5 out of 1046,47,51,57 and sex44 did not impact on the estimated prevalence. However, prevalence varied among diagnosis criteria and type of sports. For diagnostic criteria, estimates were 40.0% (95% CI: 20.0 to 60.0%) for imaging, 30.0% (95% CI: 20.0 to 30.0%) for self-reported and 10.0% (95% CI: 10.0 to 30.0%) for clinical examination. For type of sports, estimates were 30.0% (95% CI: 20.0 to 50.0%) for soccer; 20.0% (95% CI: 20.0 to 30.0%) for track and field; and 10.0% (95% CI: 0.0 to 50.0%) for rifle shooting. Therefore, analyses suggested that diagnostic criteria and type of sports impact on estimated prevalence, but not poor methodological quality or sex. See Fig. 3 for detailed sensitivity analyses.
Discussion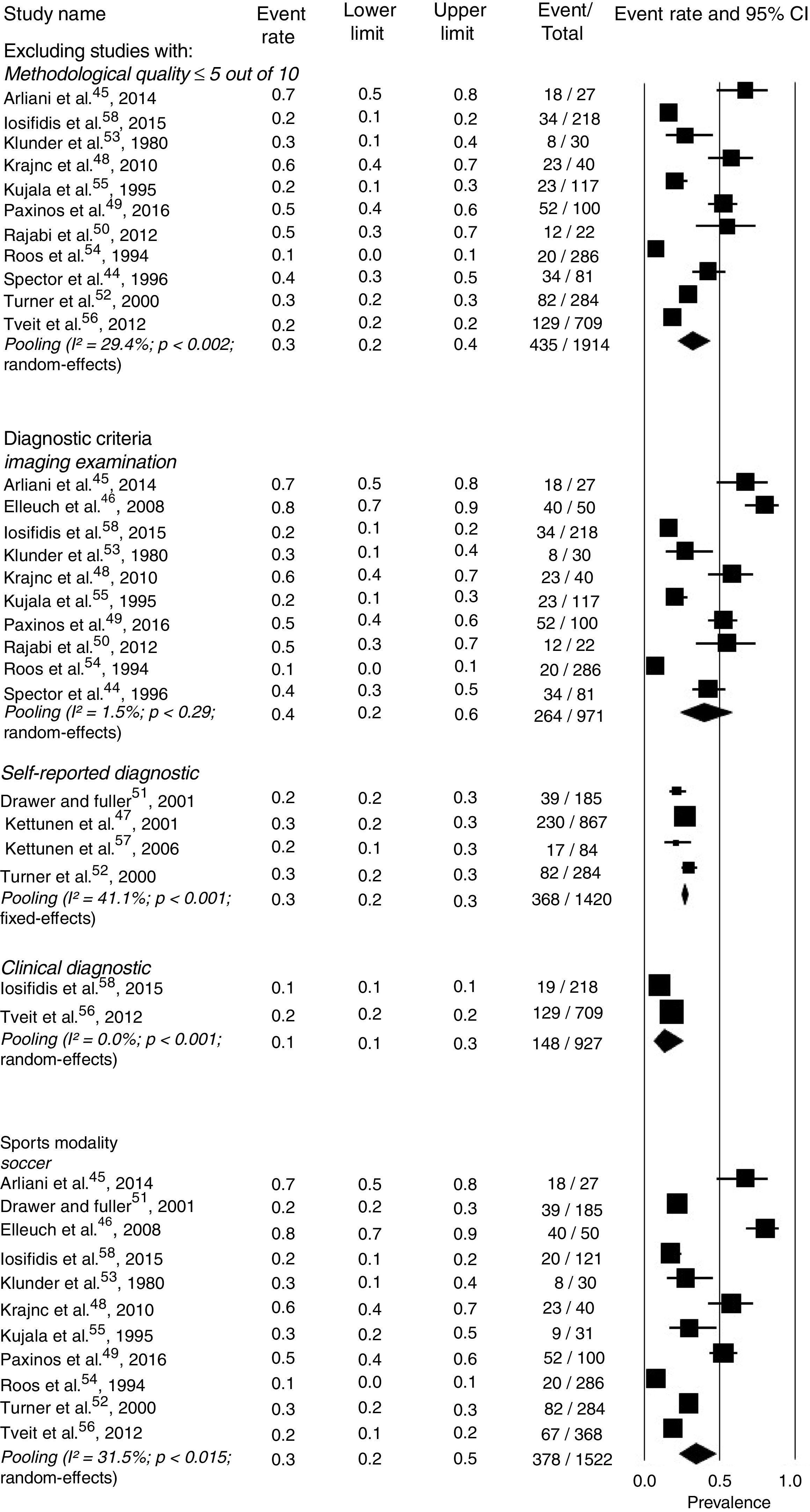
This is the first systematic review with meta-analysis primarily aiming to investigate prevalence of knee OA in former athletes. Prevalence of knee OA was 30.0% (95% CI 20.0 to 40.0%). Current low-quality evidence suggests that estimated prevalence is likely to change with future high-quality studies.
Previous studies showed that the prevalence of knee OA in general population ranged from 19.0 to 28.0%.40,55 Thus, the prevalence of knee OA in former athletes may be higher than in general population, which may be related to higher frequency of knee injuries21,22,40,59–62 and increased knee loading56,58,59,61–64 during sports participation. Knee injuries, such as fractures, ligament ruptures and meniscal tears are strong risk factors for the development of knee OA.9,55,65,66 According to Kujala et al.,55 the risk of developing knee OA is almost five times higher in high-level male athletes with meniscal injuries, knee sprains or ligament ruptures than those without previous injuries. This finding may be explained by the articular cartilage degradation that follows joint injuries.1,62 During the degradation process, the chondrocytes are not able to repair the cartilage damage, making this process continuous and persistent.23,24 In addition, trauma to the knee might cause kinematic changes that modify the cartilage region of load bearing.59 For example, previous studies have demonstrated that patients following meniscectomy and anterior cruciate ligament repair have rotational and translational changes of the tibiofemoral posture.67–69 These kinematic changes shift loading to cartilage regions that typically sustain lower loads,59–61 initiating a cascade of degenerative changes that leads to cartilage thinning.59 Finally, prevalence of knee OA in former athletes might also be explained by repetitive and increased loading associated with sports participation,55,70 which may overtake muscles capacity to protect the knee, resulting in joint degeneration.34,71
The 30.0% mean prevalence of knee OA in former athletes seems to be similar to the prevalence demonstrated by other populations at higher risk of developing knee OA. For example, a previous study31 estimated 27.0% of knee OA prevalence in obese individuals. Moreover, one study showed association of squatting with increased prevalence of knee OA.72 More specifically, the prevalence of knee OA ranged from 30.2 to 37.5% in individuals who spend more than 60min squatting per day. Thus, the prevalence of knee OA in former athletes is comparable to that presented by populations that present risk factors for knee OA, such as increased body fat tissue and knee loading.
Sensitivity analyses suggested that methodological quality of the included studies and sex do not impact on the prevalence of knee OA in former athletes. However, analyses suggested that diagnosis using imaging may overestimate the prevalence of knee OA (40.0%; 95% CI: 20.0 to 60.0%) when compared to self-reported (30.0%; 95% CI: 20.0 to 30.0%) and clinical diagnosis (10.0%; 95% CI: 10.0 to 30.0%). It is possible that radiographic signs of knee OA are more prevalent than its clinical symptoms, such as pain and stiffness.73 In addition, radiographic signs may precede the clinical onset of knee OA,58 mainly in athletes. More specifically, it is suggested that the protective effects of increased muscle strength and better joint proprioception58,71 developed during sports participation increase athletes’ pain threshold,58,70 which contributes to the late clinical diagnosis after the onset of radiographic knee OA in this population.70 Sensitivity analyses also suggested that type of sports impact on prevalence estimates. Specific demands, such as the abrupt changes of direction and increased knee loading related to sprinting, squatting, cutting and pivoting may explain differences in knee OA prevalence between different sports.34,54
Considering the high prevalence of knee OA in former athletes, sports organizations, teams and professionals should implement preventive strategies during and after athletes’ careers, which might help to reduce knee OA prevalence and its associated disabilities74 and socioeconomic impact.36 For example, prevention strategies such as neuromuscular training associated with warm-up,75 were able to reduce the occurrence of anterior cruciate ligament injuries.76,77 Olsen et al.76 showed that this program improves awareness and control of the knee during landing and spinning movements, reducing the occurrence of lower limbs injuries. Finally, previous studies have demonstrated that 78.0 to 80.0% of former soccer players are overweight,46,78 which increases the risk of developing knee OA.79 Therefore, educational programs related to healthy diet and maintenance of an active lifestyle may reduce weight gain after retirement and consequently reduce knee OA prevalence in former athletes.
Previous systematic reviews investigating the prevalence of knee OA in former athletes had methodological limitations, such as restricted date and language35 of publication, lack of protocol registration in PROSPERO and non-evaluation of the strength of the evidence.32–35 Moreover, no meta-analysis with the primary purpose of estimating the prevalence of knee OA in former athletes was conducted. The current systematic review with meta-analysis had its protocol prospectively registered at PROSPERO and the strength of the evidence evaluated using the GRADE system. The prevalence of knee OA found by the present study was higher than the prevalence demonstrated by one previous study34 and lower than two other studies.32,33 This may be explained by differences in the specific purposes and inclusion criteria between studies, which also help to explain the different number of studies included in each systematic review. Moreover, the procedures used to extract prevalence data were different. Moreover, some procedures used to evaluate quality of the included studies were different. For example, Driban et al.,34 unlike others reviews,32,33 assessed the quality of included studies using the Newcastle-Ottawa Scale (NOS). At this moment, considering the limitations demonstrated by previous systematic reviews, we believe that this review provides timely and relevant information on prevalence of knee OA in former athletes for researchers, clinicians, people with knee OA and policymakers.
Low-quality evidence suggests that future high quality studies with higher samples and clear and reliable inclusion criteria for knee OA are likely to impact on the estimated prevalence. The strength of the current evidence was downgraded due to imprecision and inconsistency.
This study had some potential limitations. It was not possible to define specific criteria to characterize former athletes, since most of the studies do not provide information regarding this construct. In order to solve this limitation, we only included studies that clearly stated that the sample was former athletes. Level of competition, OA onset and history of knee injury might influence on estimated prevalence of knee OA. These potential influences were not considered in the current study because most studies do not report them. Future studies should define specific criteria to operationalize former athletes, such as time of exposure to sport and time since retirement. In addition, they should also standardize the diagnostic criteria of knee OA. Level of competition, OA onset and history of knee injury may influence on estimated prevalence of knee OA. However, we did not consider these variables because most studies do not report them. Small number of studies was found, mainly investigating specific sports (e.g. former long distance runners, weight lifters and basketball, handball and table tennis players), which limited sensitivity analysis for some sports. Finally, most studies had small sample sizes30,32,34–37,39,41,44 and there is a lack of studies investigating former female athletes. Future studies including this population are warranted.
ConclusionThis systematic review with meta-analysis showed that the prevalence of knee OA in former athletes was 30.0% (95% CI 20.0 to 40.0%). Current low-quality evidence suggests that prevalence is likely to change with future high-quality studies. Increased knee loading and risk of injuries during sports participation might explain the high prevalence of knee OA in former athletes. Diagnostic criteria for knee OA and sport modality may impact on estimated prevalence. The high prevalence of knee OA in former athletes challenges researches, clinicians and policymakers to prevent and treat this health condition. It is possible that different strategies may reduce the knee OA prevalence and associated disabilities in former athletes.
Conflicts of interestThe authors declare no conflicts of interest.
The authors are thankful to the Brazilian Government Funding Agency FAPEMIG, Grant Number APQ-01139-15, for its financial support.
OVID (Medline, Embase, AMED)
- 1.
prevalence.mp. or Prevalence/
- 2.
Incidence.mp. or Incidence/
- 3.
epidemiolog$.mp.
- 4.
probability.mp. or Probability/
- 5.
athlete$.mp. or Athletes/
- 6.
Sports/ or Athletic Injuries/ or Sportsperson.mp.
- 7.
Sports Medicine/ or Sportsman.mp.
- 8.
Sportswoman.mp.
- 9.
former athlete$.mp. [mp=ab, hw, ti, tn, ot, dm, mf, dv, kw, nm, kf, px, rx, an, ui]
- 10.
retired athlete$.mp. [mp=ab, hw, ti, tn, ot, dm, mf, dv, kw, nm, kf, px, rx, an, ui]
- 11.
elite athlete$.mp. [mp=ab, hw, ti, tn, ot, dm, mf, dv, kw, nm, kf, px, rx, an, ui]
- 12.
ex-athlete$.mp. [mp=ab, hw, ti, tn, ot, dm, mf, dv, kw, nm, kf, px, rx, an, ui]
- 13.
osteoarthr$.mp. [mp=ab, hw, ti, tn, ot, dm, mf, dv, kw, nm, kf, px, rx, an, ui]
- 14.
degenerative joint disease$.mp. [mp=ab, hw, ti, tn, ot, dm, mf, dv, kw, nm, kf, px, rx, an, ui]
- 15.
arthr$.mp. [mp=ab, hw, ti, tn, ot, dm, mf, dv, kw, nm, kf, px, rx, an, ui]
- 16.
1 or 2 or 3 or 4
- 17.
or 6 or 7 or 8 or 9 or 10 or 11 or 12
- 18.
13 or 14 or 15
- 19.
16 and 17 and 18
EBSCO (SPORTDiscus and CINAHL)
| S19 | S16 AND S17 AND S18 |
| S18 | S1 OR S2 OR S3 OR S4 |
| S17 | S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 |
| S16 | S13 OR S14 OR S15 |
| S15 | arthr* |
| S14 | degenerative joint disease* |
| S13 | osteoarthr* |
| S12 | ex-athlete* |
| S11 | elite athlete* |
| S10 | retired athlete* |
| S9 | former athlete* |
| S8 | Sportswoman |
| S7 | Sportsman |
| S6 | Sportsperson |
| S5 | athlete* |
| S4 | probability |
| S3 | epidemiolog* |
| S2 | Incidence |
| S1 | prevalence |



