





To evaluate within- and between-days reliability of two normalization methods of surface electromyography (sEMG) recordings of the trapezius muscle.
MethodsNineteen women were allocated into 2 groups (healthy and with neck-shoulder pain). The sEMG was recorded in two sessions with 7 days in between sessions. The four portions of the trapezius muscle (the clavicular and acromial fibers of the upper trapezius, the middle and the lower trapezius) were evaluated during maximal and submaximal isometric voluntary contractions. The within- and between-days reliability of both maximal and submaximal contractions were assessed through Intraclass Correlation Coefficient (ICC(2,1) was used for within-day analyses of both maximal and submaximal contractions, and for between-days analyses of maximal contractions while ICC(2,3) was used for between-days analyses of submaximal contractions), Coefficient of Variation, Standard Error of Measurement, and Bland–Altman analysis.
ResultsIn general, submaximal contractions presented higher within-day reliability, with higher ICC values (e.g., middle trapezius – mean of 0.97), smaller Coefficient of Variation and Standard Error of Measurement ranges compared to maximal contractions (ICC values, e.g. for middle trapezius – mean of 0.94) in both groups. The same pattern was observed for between-days analyses, with submaximal contractions presenting higher ICC values (e.g., middle trapezius – mean of 0.84), smaller Coefficient of Variation and Standard Error of Measurement ranges than maximal contractions (ICC values, e.g. for middle trapezius – mean of 0.73) in both groups.
ConclusionSubmaximal contractions are recommended for normalization procedures of trapezius sEMG, in both subjects with neck-shoulder pain and healthy individuals.
The trapezius muscle is one of the most important stabilizers of the shoulder,1 performing scapular movements and providing stabilization combined with the serratus anterior muscle.2 Alterations in trapezius activation have been associated with musculoskeletal disorders.2–4 Therefore, surface electromyography (sEMG) has been widely used in different areas of knowledge to assess the trapezius muscle such as in clinical research,5–7 sports science8–10 and occupational biomechanics.11–13 Despite its wide use, the reliability of sEMG data is susceptible to intrinsic and extrinsic influences such as the type of muscle contraction used to assess activation,14 electrode placement, skin resistance,15 and signal processing methods.16 In order to minimize the influence of such factors, signal normalization using standardized and reproducible muscle contractions is strongly recommended.11
In 1995, a systematic review synthesized the main sEMG normalization methods for the upper trapezius and proposed a standardized method for normalization.11 The authors recommended that sEMG normalization of the upper trapezius should be performed based on both maximal voluntary contractions (MVC) and submaximal voluntary contractions (SVC). However, only MVC has been used.17,18 Literature has recommended the use of MVC for sEMG normalization19 due to its good reliability and because it allows researchers to calculate the percentage of muscle activation during the task under investigation. However, this recommendation has important limitations, particularly for individuals with pain, because maximal effort can cause discomfort, increase symptoms, and underestimate maximal effort.19
Studies focusing on the evaluation of methods of sEMG normalization have investigated lower limb,20–23 trunk, and upper limb muscles,24–27 but not the trapezius. Furthermore, studies assessing the trapezius have only considered its upper portion.11,28,29 The only study that assessed the different portions of the trapezius30 was an investigation of various sEMG normalization techniques, all of which employed maximal contractions without considering submaximal ones. Moreover, there is an important lack of information in the available literature regarding sEMG normalization for subjects with pain. Considering that studies assessing trapezius muscle sEMG in subjects with chronic or acute pain have shown important changes in the activation pattern and muscle recruitment,17,31,32 the need for information about reliable methods of sEMG normalization of the trapezius muscle in subjects with neck-shoulder pain is clear. To our knowledge, there is no study evaluating the reliability of sEMG normalization methods, considering the different portions of the trapezius muscle in subjects with and without neck-shoulder pain.
The aim of this study was to evaluate within and between-days reliability of isometric SVC and MVC of the four portions of the trapezius muscle, in order to uncover the best method for sEMG normalization, in women with and without neck-shoulder pain. We hypothesized that: (1) both maximal and submaximal contractions will exhibit good reliability; (2) subjects with neck-shoulder pain will exhibit more reliable results for SVC when compared to MVC since maximal effort can be a source of variability for subjects with pain.
MethodsSampleWomen between 20 and 30 years old, not professionally involved in sports, were invited to participate in this study. They received an e-mail and were asked to answer an online questionnaire. Eligible subjects were contacted to schedule a physical evaluation,33 performed by a trained physical therapist, in order to assign them into the two study groups. According to the results of the physical examination, the data collection was scheduled. We focused on women due to their greater predisposition to develop upper limb work-related musculoskeletal disorders.34,35
Sample size was estimated according to a method developed for reliability studies.36 Both α and β values were set at 0.05 and 0.2, respectively. We have also considered: (1) the number of replicates used in the analyses (n=3); (2) the minimally acceptable ICC of 0.6 (classified as good)37; and (3) the expected ICC of 0.9 (based on a study evaluating the within and between reliability obtained from trunk muscles).38 Sample size was estimated as 16 volunteers, and to avoid problems with loss of data, twenty subjects were recruited. They were allocated into two groups: healthy (HG) and neck-shoulder pain (NSPG) group. Sample selection was based on the results of the Nordic Musculoskeletal Questionnaire (NMQ)39 – which was collected online, the Visual Analog Scale (VAS) and the standardized physical examination proposed by the Department of Occupational and Environmental Medicine, Lund, Sweden.33 Inclusion criteria for the HG were: absence of self-reported musculoskeletal symptoms in the last week and absence of disorders in the neck-shoulder region according to the NMQ and the standardized physical examination, respectively. The inclusion criteria for the NSPG were: self-reported problems in the neck region in the last seven days according to the NMQ; diagnosis of neck tension syndrome or cervical syndrome accordingly to the standardized physical examination; pain in the neck region with a moderate to severe pain intensity measured by a VAS (i.e., score>4cm on a 0–10cm scale).40 In the recruitment stage, 6 subjects were excluded once they did not meet all inclusion criteria for NSPG. Exclusion criteria for both groups were: the presence of more than 4 affected body regions in the past week according to the NMQ, for preventing the inclusion of subjects with systemic disorders; self-report of circulatory, rheumatic or inflammatory diseases; involvement in overhead sports, even in leisure time. One subject of the NSPG was excluded due to problems with sEMG signal.
Ten women were allocated in HG with mean (standard deviation): age – 21.4 (3.2) years, weight – 56.3 (8.3)kg, and height – 161.8 (6.3)cm; and 9 in NSPG with mean (standard deviation): age – 23.4 (1.9) years, weight – 56.8 (6.6)kg, and height – 163.3 (5.20)cm. The reported pain intensity in NSPG for neck and shoulders were 5.4±1.1cm and 2.6±3.1cm, respectively. This study was conducted in agreement with the Declaration of Helsinki, and was approved by the ethics committee of Universidade Federal de São Carlos (UFSCar), São Carlos, SP, Brazil (Protocol #28384814.6.0000.5504). All subjects signed a consent form prior to participation.
Experimental protocolThe sEMG recordings were performed in two sessions with 7 days between sessions. Both portions of the upper trapezius-clavicular (C-UT) and acromial (A-UT), the middle (MT) and the lower (LT) trapezius were evaluated on the dominant side using active differential electrodes (DE-2.3, Delsys, Boston, MA, USA). Before electrode placement, the skin was rubbed lightly with 70% ethyl alcohol and shaved in order to reduce the impedance and eliminate possible interference.
The C-UT electrode was placed 20% laterally to the midpoint between the dorsal processes of C4 and the posterior lateral third of the clavicle41; the A-UT electrode was placed approximately 2cm lateral to the midpoint between C7 and the acromion with the poles of the electrode parallel to the direction of the muscle fibers11; the MT electrode was placed approximately 20% medial to the midpoint between the medial border of the scapula and T4; and the LT electrode was placed approximately 33% medial to the midpoint between the medial border of the scapula and T8.42 The reference electrode (adhesive, squared, 5cm side) was fixed on the manubrium sternae. The signals were acquired at 1000Hz and conditioned by the main amplifier, which provided a gain of 2000, 16-bit resolution and noise of 1.2μV (RMS).
After electrode placement, a 5-seconds rest recording was performed in order to eliminate basal noise from the recordings. Two series of isometric maximal and submaximal contractions were then randomly performed. Both series were composed of 3 contractions of 5s each43 with an interval of 1min between them.44 For the maximal series, manual resistance was applied45 and verbal encouragement was used. The submaximal series were performed while holding a halter of 1kg.43 For the C-UT and A-UT contractions, the subjects were positioned seated in a comfortable chair with knees and hips flexed at 90°. For the C-UT contraction, the subjects positioned the dominant arm at 90° abduction on the frontal plane, with hand facing down, and the neck was extended and rotated to the non-dominant side41 (Fig. 1A). For the A-UT contraction, the subjects positioned the dominant arm at 90° abduction on the frontal plane, with hand facing down and the neck in neutral position11 (Fig. 1B). For the MT and LT contractions, the subjects were lying prone with the neck in neutral position. For MT, the shoulder was abducted 90° parallel to the table with the hand rotated 90° laterally (Fig. 1C). And for LT, the arm was aligned to the direction of the LT muscle fibers, abducted to approximately 120°, with the hand facing down46 (Fig. 1D). For all MVCs, the manual resistance was applied proximal to the elbow joint – except for the C-UT, with resistance proximal to the shoulder. Furthermore, for C-UT and A-UT contractions the evaluator was positioned behind the subject, while for MT and LT the evaluator was positioned beside the trunk of the subject. The order of assessment of the muscle portions was randomized.

Test positions during maximal and submaximal muscle contractions for the upper-clavicular fibers (a), upper-acromial fibers (b), middle (c), and lower (d) trapezius. Manual resistance was applied for maximal voluntary contractions, as shown in the pictures. The same positions were used for submaximal voluntary contractions with subjects holding a halter of 1kg.
The sEMG signals were processed using Matlab (version 8.0, The Mathworks Inc., Natick, MA, USA). All signals were corrected for offset and band-pass filtered using a 6th order zero-lag Butterworth filter in the 30–450Hz band. Signals were then converted into RMS using 100-millisecond moving windows47 with overlap of 50%. The mean RMS amplitude obtained during rest was considered the noise level and removed from the signals, in a power basis. To evaluate the within-day reliability, the sEMG peak amplitude was considered for each trial of MVC and the mean sEMG amplitude was used for each trial of SVC. The highest sEMG peak amplitude, regardless of which trial, for MVCs on day 1 and on day 2 was extracted and used in the between-days reliability analysis. The mean sEMG amplitude of all the three submaximal trials on days 1 and 2 were used for the between-days reliability analysis of SVCs.
Statistical analysisThe within- and between-days reliability, which may be analyzed in order to determine how much a measure are equal, considering repeated measurement in different occasions,48 was evaluated through the Intraclass Correlation Coefficient, the coefficient of variation (%CV), the standard error of the measurement (SEM and %SEM) and the Bland–Altman analysis. All the tests were run in SPSS (Statistical Package for Social Science, v. 17) and Microsoft Excel (Microsoft Office, v. 2007), with the alpha level set at 0.05 (5%). All data were tested for normality (Shapiro Wilk test) and homoscedasticity (Levene test).
Relative reliability of the within-day analyses for MVC and SVC and of the between-days analyses for MVC was determined based on the ICC(2,1) while the relative reliability of the between-days analyses for SVC was based on the ICC(2,3). The ICC for within-day reliability was calculated using data from the 3 trials assessed on the first day. To determine the between-days reliability, ICC was calculated using the average of the mean sEMG amplitude from the SVCs in each day and the peak amplitude from the MVCs in each day. The ICC values were interpreted according to the following classification: poor (<0.20), fair (0.21–0.40), moderate (0.41–0.60), good (0.61–0.80) or very good (0.81–1.00).37
Absolute reliability was determined by the %CV, SEM and %SEM, and Bland–Altman analysis. CV expresses the stability of the measurement and was calculated following the formula: %CV=SDCV/MCV×100, where SDCV is the standard deviation of CV values calculated for each individual and MCV is the mean of the 3 trials on day 1 (within-day reliability) or the mean of day 1 and 2 (between-days reliability). The SEM considers the random error of the measurement and quantifies the variability between subjects on repeated measures.49 It was calculated according to the formula: SEM=SD √(1−ICC), where the SD represents the standard deviation between trials (within-day reliability) or the standard deviation of days 1 and 2 (between-days reliability). The %SEM was calculated to evaluate this measure on relative values.38 The following formula was used: %SEM=(SEM/M)×100, was used, where M is the mean of trials on day 1 (within-day reliability) or the mean of days 1 and 2 (between-days reliability).
The Bland–Altman analysis was used to determine the agreement between the measures during day 1 and day 2. The mean of differences (MD) between the two days (estimated bias) and the 95% upper and lower limits of agreement (LOA) were calculated in order to determine the influence of random error on the data of interest. The LOA was calculated using the following formula: LOA=SD*1.96±MD.
ResultsThe results regarding relative and absolute within-day reliability, for both groups, are shown in Table 1. Considering ICC scores, all contractions showed very good within-day reliability (ICC>0.81). Comparing SVC and MVC within-day, almost all portions of the trapezius muscle presented more reliable values for SVC (higher ICC values and smaller %CV and %SEM ranges), except the LT for NSPG, which presented a trend of more reliable values for MVC, considering the relative (higher value of ICC), and absolute reliability (slightly smaller values of %CV and %SEM).
Mean and standard deviation (SD) of sEMG amplitude (in mV) at each trial on day 1 and within-day reliability analyses results (ICC with its confidence intervals, %CV, SEM and %SEM), for both groups, in maximal voluntary contractions (MVC) and submaximal voluntary contractions (SVC).
| Healthy group | Neck-shoulder pain group | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trial 1 Mean (SD) | Trial 2 Mean (SD) | Trial 3 Mean (SD) | ICC (CI) | %CV | SEM | %SEM | Trial 1 Mean (SD) | Trial 2 Mean (SD) | Trial 3 Mean (SD) | ICC (CI) | %CV | SEM | %SEM | |
| MVC (Peak RMS) | ||||||||||||||
| C-UT | 0.093 (0.048) | 0.090 (0.047) | 0.105 (0.063) | 0.94 (0.82–0.98) | 21.19 | 0.06 | 21.99 | 0.126 (0.055) | 0.144 (0.076) | 0.181 (0.139) | 0.87 (0.60–0.97) | 18.03 | 0.05 | 35.38 |
| A-UT | 0.307 (0.198) | 0.290 (0.161) | 0.285 (0.166) | 0.99 (0.96–1.00) | 9.34 | 0.04 | 11.56 | 0.282 (0.143) | 0.251 (0.105) | 0.243 (0.087) | 0.95 (0.86–0.99) | 11.74 | 0.04 | 15.24 |
| MT | 0.232 (0.104) | 0.195 (0.094) | 0.189 (0.098) | 0.95 (0.82–0.99) | 20.06 | 0.06 | 17.78 | 0.214 (0.125) | 0.205 (0.122) | 0.173 (0.094) | 0.93 (0.78–0.98) | 18.15 | 0.05 | 24.57 |
| LT | 0.296 (0.166) | 0.243 (0.109) | 0.250 (0.121) | 0.95 (0.83–0.99) | 14.95 | 0.06 | 19.00 | 0.281 (0.111) | 0.252 (0.114) | 0.247 (0.111) | 0.97 (0.90–0.99) | 12.05 | 0.03 | 11.98 |
| SVC (Mean RMS) | ||||||||||||||
| C-UT | 0.025 (0.026) | 0.023 (0.023) | 0.023 (0.022) | 1.00 (0.98–1.00) | 9.16 | 0.02 | 12.12 | 0.025 (0.008) | 0.027 (0.010) | 0.027 (0.009) | 0.96 (0.87–0.99) | 10.52 | 0.00 | 12.06 |
| A-UT | 0.083 (0.043) | 0.074 (0.039) | 0.078 (0.042) | 0.99 (0.96–1.00) | 8.66 | 0.03 | 9.15 | 0.086 (0.034) | 0.082 (0.032) | 0.082 (0.033) | 0.98 (0.93–0.99) | 7.66 | 0.01 | 10.01 |
| MT | 0.114 (0.067) | 0.108 (0.056) | 0.125 (0.062) | 0.96 (0.87–0.99) | 13.18 | 0.05 | 18.21 | 0.088 (0.060) | 0.098 (0.063) | 0.104 (0.061) | 0.98 (0.93–1.00) | 11.20 | 0.02 | 15.40 |
| LT | 0.131 (0.055) | 0.119 (0.043) | 0.123 (0.042) | 0.95 (0.87–0.99) | 11.38 | 0.05 | 13.02 | 0.122 (0.045) | 0.127 (0.059) | 0.133 (0.059) | 0.94 (0.81–0.99) | 12.85 | 0.02 | 16.98 |
Table 2 shows the results regarding the between-days reliability. The ICC showed more variable ranges when compared with the within-day reliability. For the HG, all trapezius portions, except the LT, showed greater reliability on SVC (good ICC for C-UT and MT, and very good for A-UT). Regarding the NSPG, all trapezius portions, except the C-UT, showed greater reliability on SVC through higher values of ICC and smaller values of %SEM.
Mean and standard deviation (SD) of sEMG amplitude (in mV) at each day and between-days reliability analyses results (ICC with its confidence intervals, %CV, %SEM, %LOA and %MD) for both groups, in maximal voluntary contractions (MVC) and submaximal voluntary contractions (SVC). U in %LOA represents the upper limit of agreement and L the lower limit.
| Healthy group | Neck-shoulder pain group | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Day 1 Mean (SD) | Day 2 Mean (SD) | ICC (CI) | %CV | %SEM | %LOA | %MD | Day 1 Mean (SD) | Day 2 Mean (SD) | ICC (CI) | %CV | %SEM | %LOA | %MD | |||
| MVC (Peak RMS) | ||||||||||||||||
| C-UT | 0.115 (0.058) | 0.144 (0.065) | 0.57 (−0.47 to 0.89) | 35.07 | 37.27 | U: | −16 | −2.9 | 0.186 (0.135) | 0.155 (0.075) | 0.69 (−0.32 to 0.93) | 37.05 | 43.20 | U: | −19 | 3.1 |
| L: | 10 | L: | 24 | |||||||||||||
| A-UT | 0.322 (0.194) | 0.298 (0.100) | 0.79 (0.15–0.95) | 26.21 | 28.63 | U: | −23 | 2.4 | 0.291 (0.134) | 0.290 (0.120) | 0.95 (0.78–0.99) | 11.54 | 12.92 | U: | −11 | 0 |
| L: | 28 | L: | 11 | |||||||||||||
| MT | 0.237 (0.101) | 0.302 (0.198) | 0.57 (−0.56 to 0.89) | 23.29 | 45.17 | U: | −4 | −6.5 | 0.234 (0.126) | 0.192 (0.094) | 0.89 (0.49–0.98) | 16.66 | 22.89 | U: | −8 | 4.1 |
| L: | 27 | L: | 16 | |||||||||||||
| LT | 0.304 (0.159) | 0.293 (0.160) | 0.97 (0.87–0.99) | 10.01 | 13.34 | U: | −11 | 1.1 | 0.286 (0.112) | 0.213 (0.089) | 0.32 (−1.02 to 0.83) | 35.37 | 37.94 | U: | −17 | 7.3 |
| L: | 13 | L: | 32 | |||||||||||||
| SVC (Mean RMS) | ||||||||||||||||
| C-UT | 0.024 (0.023) | 0.027 (0.013) | 0.72 (−0.15 to 0.93) | 41.28 | 38.34 | U: | −4 | −0.4 | 0.026 (0.009) | 0.035 (0.017) | −0.40 (−4.50 to 0.67) | 36.36 | 54.16 | U: | −5 | −0.8 |
| L: | 3 | L: | 3 | |||||||||||||
| A-UT | 0.079 (0.041) | 0.080 (0.036) | 0.93 (0.70–0.98) | 16.82 | 12.89 | U: | −4 | −0.2 | 0.083 (0.032) | 0.084 (0.034) | 0.98 (0.92–1.00) | 5.09 | 5.04 | U: | −2 | 0 |
| L: | 4 | L: | 2 | |||||||||||||
| MT | 0.116 (0.059) | 0.137 (0.105) | 0.77 (0.11–0.94) | 23.85 | 31.89 | U: | −17 | −2.2 | 0.096 (0.060) | 0.083 (0.057) | 0.92 (0.66–0.98) | 21.20 | 18.30 | U: | −5 | 1.3 |
| L: | 12 | L: | 7 | |||||||||||||
| LT | 0.125 (0.045) | 0.145 (0.088) | 0.64 (−0.41 to 0.91) | 18.90 | 30.71 | U: | −16 | −2.1 | 0.127 (0.052) | 0.131 (0.051) | 0.73 (−0.34 to 0.94) | 18.05 | 20.16 | U: | −10 | −0.3 |
| L: | 12 | L: | 9 | |||||||||||||
Furthermore, considering the Bland–Altman analysis, SVC showed MD values closer to 0 and smaller ranges of LOA for both groups and for all muscle portions except for LT in HG when compared to MVC. These findings can be confirmed through Bland–Altman plots that show the distribution of measurement differences between days 1 and 2 (Figs. 2 and 3).
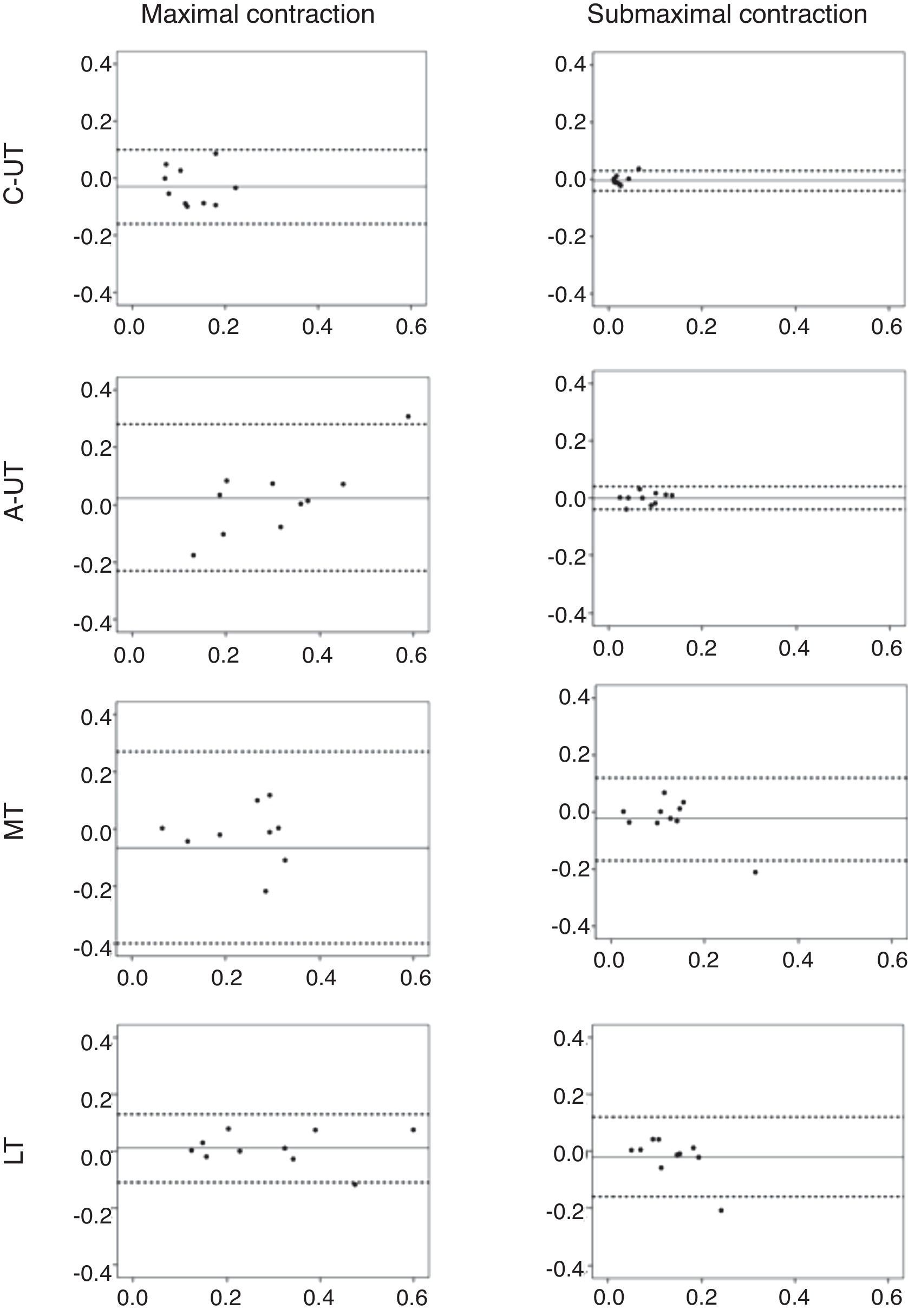
Bland–Altman plots for sEMG amplitude on submaximal and maximal contractions for clavicular fibers of the upper trapezius (C-UT), acromial fibers (A-UT) of the upper trapezius, middle (MT), and lower (LT) trapezius on healthy group. Axis X represents the mean of values obtained on day 1 and day 2 and axis Y represents the difference between those values. The full line shows the mean difference between day 1 and day 2. The dashed lines show the lower (mean−1.96*SD) and upper (mean+1.96*SD) limits of agreement.
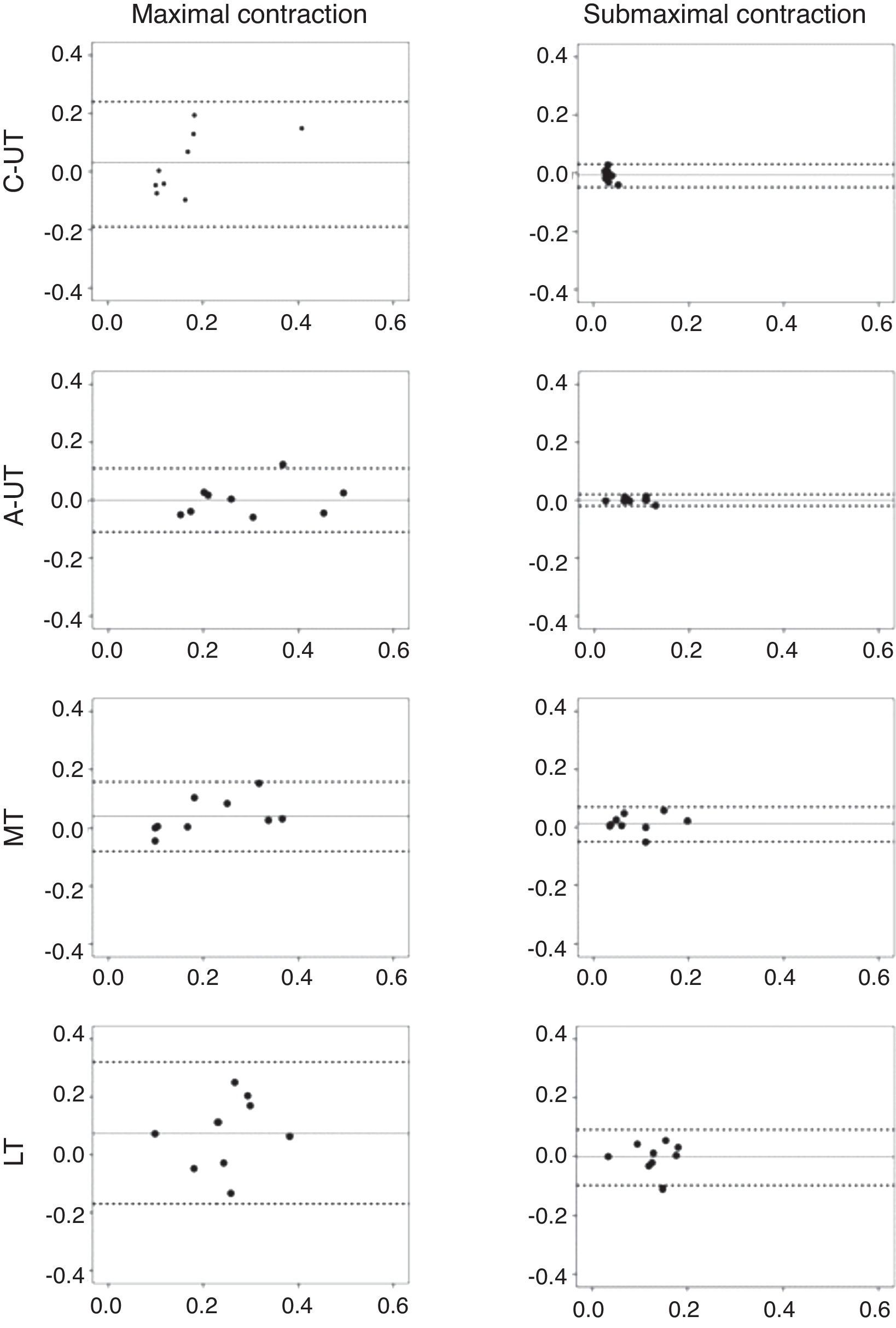
Bland–Altman plots for sEMG amplitude on submaximal and maximal contractions for clavicular fibers of the upper trapezius (C-UT), acromial fibers of the upper trapezius (A-UT), middle (MT) and lower (LT) trapezius on neck-shoulder pain group. Axis X represents the mean of values obtained on day 1 and day 2 and axis Y represents the difference between those values. The full line shows the mean difference between day 1 and day 2. The dashed lines show the lower (mean−1.96*SD) and upper (mean+1.96*SD) limits of agreement.
This study investigated the reliability of maximal and submaximal isometric contractions performed for sEMG normalization in subjects with and without neck-shoulder pain. In general, both maximal and submaximal contractions showed good relative reliability (observed through ICC values), regardless of the group, considering both within- and between-days. Nevertheless, when considering the absolute reliability (determined by the %CV, SEM and %SEM and Bland–Altman analysis), submaximal contractions showed better within- and between-days reliability than maximal contractions for almost all portions of the trapezius muscle, in both groups.
The results for the healthy group showed that submaximal contractions had higher reliability when compared to MVCs in the within-day analysis for all trapezius portions, considering the %CV and %SEM. Similar results were observed in the between-days comparison. Literature shows similar results for trunk and upper limb muscles, with higher reliability reported for SVC than MVC.38,47,50 Allison et al.47 have also found higher values of %CV during MVC for the biceps brachialis muscle, indicating a higher variation on sEMG signal obtained during maximal contractions compared with submaximal ones. According with the analysis interpretation proposed by Ludbrook,51 the results from Bland–Altman analysis for between-days comparison indicate better between-days agreement for submaximal contractions in comparison with MVCs for all trapezius portions except for LT, reinforcing the recommendation to use SVC for sEMG normalization.
The results observed for the neck-shoulder pain group were similar to the healthy group. Submaximal contractions showed higher reliability than MVCs in within-day analysis for all portions of the trapezius muscle except for the LT. Furthermore, submaximal contractions were also more reliable than MVCs for the between-days analysis. These findings were confirmed by the Bland–Altman analyses. The only exception was C-UT, which presented higher reliability for maximal contractions according to ICC and %SEM. The test position used in this study to evaluate C-UT is recommended as the best one to record maximal muscle activity.41 However, to our knowledge, there is no recommendation of a testing position for submaximal contractions of C-UT. The absence of resistance on the head during submaximal tests may have influenced the activation of the C-UT since the upper fascicles of this muscle portion are involved in head movement. The evaluation of the clavicular (C-UT) and acromial fibers (A-UT), as well as the different motor behavior between these two portions, is relatively new52 and deserves attention in future research. Therefore, the lack of information reduces the ability to understand the expected behavior for those portions of the upper trapezius.
It is important to consider that motivational and psychosocial factors may influence the performance of MVCs38 and that the effort of the subjects cannot be adequately controlled and monitored during the test.53 The use of maximal contractions can be a source of discomfort and also can lead to an overestimation of muscle activation.54 The type of resistance applied during MVCs can also be a source of variability. In this study, the resistance was manually applied since this method is the most reported in the literature38 but the use of straps is also commonly reported.55–59 It is possible that the use of manual resistance (feedback) associated with straps (stability) might decrease the variation on sEMG signal obtained during maximal contractions. This may deserve attention in further research because there is no consensus in the literature regarding the best way to provide resistance in maximal contractions.
Even though submaximal contractions have been shown to be more reliable than maximal ones, they may reduce the inter-subject variability when compared to MVCs.11 This is something desired but, on the other hand, may make the assessment of muscle activity patterns considering the true biological variance more difficult.47 The use of SVCs with standardized load may be a confounding factor when evaluating subjects with different muscle activation levels during its performance.29 In such a case, the sEMG signal may also be normalized through other methods such as isokinetic MVCs and dynamic activities (e.g. the cycles of gait)23 besides maximal and submaximal contractions.
Finally, some methodological limitations should be addressed. Our results are applicable to the women population. Considering the recent evidence for sex differences on trapezius activation,60,61 further studies should consider performing this investigation in males. Furthermore, the manual resistance applied during MVCs may represent a source of variability during the tests. Other testing positions have been reported in the literature, with external loads different than 1kg for submaximal contractions or with different types of resistance applied for maximal contractions. Different resistance and test positions may cause different patterns of muscle activation. Therefore, our findings are applicable just for the conditions described above. Notwithstanding, these test positions are commonly reported in the literature.
ConclusionThe use of submaximal contractions for sEMG normalization is recommended for the trapezius muscle in subjects with and without neck-shoulder pain. Our results contribute to a better standardization of sEMG normalization methods for the trapezius muscle, which has been widely investigated in several areas of knowledge due to its important role in shoulder function and in the development of neck-shoulder disorders.
Conflicts of interestThe authors declare no conflicts of interest.



