



Previous validity studies of the Alberta Infant Motor Scale (AIMS), using raw scores and percentile curves for group comparisons, showed that infants in Brazil achieved gross motor milestones at later ages. Validity of the AIMS norms were later reassessed using a logistic regression model that placed the AIMS items on an age scale.
ObjectivesOur study examined the validity of the AIMS norms for Brazilian infants using the recommended method for calculating and comparing item locations.
MethodsData from 732 Brazilian infants (2009–11), 3 days to 18 months old, were compared to the AIMS normative sample (n=2202). Logistic regression placed the AIMS items of both samples on age scales representing the age at which 50% of infants passed an item and compared the two datasets. Pearson correlation coefficient tested the association across samples.
Results47 of the 58 AIMS items met the criterion for stable regression to calculate item locations of the Brazilian dataset. Based on the age when 50% of the infants passed a criterion, most of the items from the Brazilian sample (n=28) differed by two weeks or less compared to the Canadian normative sample.
ConclusionThe sequence and age for the emergence of AIMS items were similar between the Brazilian and Canadian samples. Canadian norms are appropriate for clinical decisions and research with Brazilian infants.
The Alberta Infant Motor Scale (AIMS)1 is a Canadian norm-referenced measure to assess infants’ gross motor abilities from birth to independent walking. The use of culturally specific assessment tools may influence clinical decisions and lead to either under or over-referral to pediatric services. Cultural influences on infants’ motor development may affect the validity of the AIMS norms. Studies using AIMS normative data to evaluate its validity in different countries have yielded inconsistent results.2–7 While Canadian and full-term Greek infants5 appear to acquire gross motor milestones at similar ages, Dutch infants3,6obtained motor skills at older ages. Previous studies with Brazilian infants using AIMS norms suggested that their gross motor milestones appeared at older ages compared to the Canadian normative sample.8–11 A recent study reported that Brazilian infants demonstrated lower scores in most age groups.12 The authors of these studies used the raw scores and the percentile curves for group comparisons.
In 2014, Darrah et al.13 compared the published normative data of the AIMS collected more than 20 years ago with a contemporary sample of data on Canadian infants. They conducted this re-evaluation to determine if either the back to sleep campaign occurring after development of the original normative data or changes in the ethnic diversity of the Canadian population may have influenced the age of appearance of AIMS items. They used logistic regression to place the AIMS items on an age scale representing the age at which 50% of the infants passed an item (item location). The authors concluded that the sequence and age at emergence of AIMS items have remained similar over 20 years and that the normative values remain valid. They also suggested the use of their logistic regression analysis as a cost-effective strategy for international comparisons.
A recent study has used the recommended scaling method to evaluate the appropriateness of the AIMS norms for Dutch infants.6 The authors compared the item locations of the Dutch sample (n=499) to that of the AIMS Canadian dataset (n=2202). Results showed that although the sequence of AIMS items was the same between Dutch and Canadian infants, the mean age at which 50% of the Dutch infants passed AIMS items was older compared to the Canadian sample. Based on the observed differences in the developmental rate between Canadian and Dutch infants, the authors concluded that the Canadian AIMS norms might not be appropriate to evaluate Dutch infants.6 The AIMS is the gold standard instrument to evaluate gross motor skills in infants during the first 18 months of life and used to document gross motor changes following infant early intervention programs. It is important to re-examine the validity of its normative data for Brazilian infants using the statistical method described by the AIMS authors.13
The purpose of this study was to examine if the AIMS normative data are appropriate to be used with Brazilian infants, using the logistic regression method suggested by the AIMS authors.
MethodsDesignA cross-country dataset comparison between Canadian and Brazilian normative samples, using secondary data analysis. Institutional ethics review approvals were obtained for the original data collection for both samples (University of Alberta, Edmonton, Alberta, Canada; Universidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil, approval: ETIC 604-08).1,10
ParticipantsThe Brazilian (nB=732) and the Canadian (nC=2202) samples included full-term and preterm infants (corrected age) between 3 days and 18 months old. Full-term infants from both samples had birth weights greater than 2.5kg. Participants were excluded if they showed gestational and/or delivery complications (i.e., Apgar scores below 7), and/or if they had cardiac, respiratory, or neurological problems. Brazilian and Canadian samples also included a group of healthy preterm infants.1,10 Participants from the Brazilian sample were recruited in private pediatric clinics, private day care centers, and public health services. Infants from the Canadian sample were evaluated in 27 health units from the province of Alberta, with the largest number of infants (n=1200) assessed in Edmonton and Calgary, as they are the two largest units.1,10 Parents of infants from both samples were informed of the study’s procedures and signed informed consent forms.1,10 The stratification of the infants by age group in the Brazilian sample was proportionately similar to the Canadian data.
Instrument and procedureThe AIMS is a performance-based, norm-referenced observational measure of infant gross motor development from birth to 18 months.1 The test has 58 items distributed into four subscales: prone (21 items), supine (9 items), sitting (12 items), and standing (16 items). Each item includes a description of the distribution of body weight, the postural components, and the active movements the examiner must observe to assign a grade of “observed” for an infant’s performance. Brazilian infants were evaluated by one of three experienced physical therapists trained to administer the AIMS and who achieved inter-rater reliability of 0.9. Each infant was observed for 20−30min with at least one parent (if the child was at home) or caretaker (if the child was at daycare) present. After observing an infant’s spontaneous movements, the therapist completed the AIMS score sheet. Each examination was video recorded for confirmation of the score if necessary. The sum of the item scores produced the total raw score (0–58), which can be converted to a percentile rank based on monthly age levels (0–19). For preterm infants, adjusted age was used to obtain their percentile scores.
Data analysesThe statistical technique described by Darrah et al.13 was replicated to compare the original Canadian normative dataset with Brazilian data. First, a standard logistic regression method placed AIMS items on an age scale to determine the order of the items and the age of emergence of individual items. The regression parameters were scaled to provide an estimate of the score at which 50% of the infants of that age passed each AIMS item; this age represented the ‘item location’. The second step identified the items in both datasets, which had a proportion of infants passing the item between 0.1 and 0.9 (stability criterion), excluding items whose proportions felt outside this range. Next, the item locations were plotted from both samples and the correlation coefficient was estimated. When they were strongly linearly related, the descriptive statistics were calculated. In the third step, the means and standard deviations (SD) of the item location of both sets of selected items were calculated. From these values, the locations of the items were linearly equated using the equation below, adapted from Darrah et al.13 This method allowed for a smaller sample size than needed for the original normative data.
Where:C1=std. dev.(XBrazil)/std. dev.(XCanada)
C0=Mean (XBrazil)–C1×Mean (XCanada)
The Stata® 14.1 software was used in the analyzes.
ResultsTable 1 shows the descriptive characteristics of both samples. Of the 58 items, 11 items were removed because they did not meet the stability criteria in both data sets (i.e., the regressions of age on performance are unstable for items that have more than 90% of the infants passing or failing them). Only two of the 11 items met the exclusion criteria for the Canadian data and not for the Brazilian data (prone 4 and supine 4). Because these two items were very close to reaching the elimination criteria, they were retained in the Brazilian analyses to keep the data sets similar. Thus, the same 47 items were used for the regression analyses comparison (Table 2).
Descriptive characteristics of the Canadian and Brazilian samples.
| Characteristics | Brazilian sample | Canadian sample |
|---|---|---|
| Totala | 732 | 2202 |
| Full-term infants | 664 | NA |
| Preterm infants | 68 | NA |
| Sex | ||
| Female | 363 | 1072 |
| Male | 369 | 1130 |
| Age (weeks) | 38±19.6 | 37.4±17.6 |
NA: Although the Canadian normative sample included full-term and preterm infants, the number of infants in each of these groups is not available.
Item location and age difference of the AIMS items in the Brazilian sample and AIMS norms.
| AIMS item | Brazilian infants | Original Canadian norms | Age difference between datasets (week) | Selected item | ||
|---|---|---|---|---|---|---|
| % Of infants passing | Age (week) | % Of infants passing | Age (week) | |||
| PR 1 | 100 | – | 100 | – | – | No |
| PR 2 | 97.8 | 1.8 | 97.9 | 3.1 | – | No |
| PR 3 | 91.4 | 10.4 | 94.9 | 8.6 | – | No |
| PR 4 | 85.9 | 15.0 | 90.7 | 13.6 | – | No |
| PR 5 | 83.7 | 16.5 | 89.1 | 15.1 | 1.4 | Yes |
| PR 6 | 79.5 | 19.9 | 85.0 | 18.6 | 1.3 | Yes |
| PR 7 | 73.5 | 23.9 | 79.6 | 21.8 | 2.2 | Yes |
| PR 8 | 69 | 26.5 | 66.5 | 27.8 | −1.3 | Yes |
| PR 9 | 65.9 | 28.6 | 70.9 | 25.8 | 2.8 | Yes |
| PR 10 | 68.2 | 27.3 | 73.6 | 25.1 | 2.2 | Yes |
| PR 11 | 62.2 | 30.8 | 66.0 | 28.6 | 2.2 | Yes |
| PR 12 | 58.1 | 33.1 | 57.0 | 32.9 | 0.3 | Yes |
| PR 13 | 53.8 | 34.9 | 56.2 | 33.2 | 1.6 | Yes |
| PR 14 | 52.7 | 36.2 | 54.7 | 34.0 | 2.2 | Yes |
| PR 15 | 50.4 | 37.5 | 52.5 | 35.0 | 2.5 | Yes |
| PR 16 | 51.6 | 36.8 | 48.6 | 36.8 | 0.0 | Yes |
| PR 17 | 48 | 38.9 | 37.4 | 43.6 | −4.7 | Yes |
| PR 18 | 47.3 | 39.2 | 46.0 | 38.0 | 1.2 | Yes |
| PR 19 | 44 | 40.4 | 43.2 | 39.4 | 0.9 | Yes |
| PR 20 | 41.5 | 42.6 | 39.8 | 41.2 | 1.4 | Yes |
| PR 21 | 36.6 | 45.6 | 39.0 | 41.5 | 4.1 | Yes |
| SU 1 | 100 | – | 100 | – | – | No |
| SU 2 | 98 | 2.8 | 99.4 | 1.6 | – | No |
| SU 3 | 93.7 | 8.6 | 97.3 | 6.4 | – | No |
| SU 4 | 87.4 | 13.8 | 91.4 | 13.0 | – | No |
| SU 5 | 79.6 | 19.6 | 84.4 | 18.6 | 1.0 | Yes |
| SU 6 | 75.6 | 22.4 | 82.3 | 19.6 | 2.8 | Yes |
| SU 7 | 73 | 24.1 | 78.4 | 22.4 | 1.7 | Yes |
| SU 8 | 67.4 | 27.6 | 66.6 | 27.9 | −0.3 | Yes |
| SU 9 | 61.2 | 31.3 | 59.4 | 31.8 | −0.5 | Yes |
| Sit 1 | 99.5 | 0.0a | 99.1 | – | – | No |
| Sit 2 | 89.5 | 11.9 | 89.7 | 14.0 | −2.1 | Yes |
| Sit 3 | 86.1 | 14.8 | 87.3 | 16.4 | −1.5 | Yes |
| Sit 4 | 78.6 | 20.6 | 79.9 | 21.4 | −0.8 | Yes |
| Sit 5 | 76.8 | 21.9 | 78.0 | 22.9 | −1.0 | Yes |
| Sit 6 | 71.6 | 25.3 | 72.5 | 25.8 | −0.5 | Yes |
| Sit 7 | 69.7 | 26.5 | 68.1 | 27.8 | −1.3 | Yes |
| Sit 8 | 65.7 | 29.0 | 63.6 | 29.9 | −1.0 | Yes |
| Sit 9 | 61.2 | 31.6 | 59.2 | 31.9 | −0.4 | Yes |
| Sit 10 | 56.8 | 33.9 | 43.5 | 39.7 | −5.9 | Yes |
| Sit 11 | 52.9 | 36.0 | 49.0 | 36.6 | −0.6 | Yes |
| Sit 12 | 48.1 | 38.8 | 40.0 | 41.0 | −2.2 | Yes |
| ST 1 | 100 | – | 99.6 | – | – | No |
| ST 2 | 93.2 | 8.8 | 96.2 | 3.7 | – | No |
| ST 3 | 74.6 | 23.1 | 76.2 | 22.9 | 0.2 | Yes |
| ST 4 | 49.5 | 38.0 | 47.0 | 37.5 | 0.5 | Yes |
| ST 5 | 45.9 | 40.0 | 45.0 | 38.5 | 1.5 | Yes |
| ST 6 | 44.8 | 40.0 | 44.9 | 38.5 | 1.5 | Yes |
| ST 7 | 42.8 | 41.8 | 35.0 | 44.5 | −2.6 | Yes |
| ST 8 | 41.5 | 42.5 | 42.8 | 39.5 | 3.0 | Yes |
| ST 9 | 38.3 | 44.4 | 38.1 | 42.0 | 2.4 | Yes |
| ST 10 | 34.3 | 46.8 | 35.5 | 43.5 | 3.3 | Yes |
| ST 11 | 30.3 | 49.4 | 28.1 | 47.7 | 1.7 | Yes |
| ST 12 | 26.8 | 51.8 | 22.9 | 51.0 | 0.8 | Yes |
| ST 13 | 21.7 | 55.7 | 20.4 | 52.7 | 3.0 | Yes |
| ST 14 | 20.8 | 56.6 | 17.6 | 55.9 | 0.7 | Yes |
| ST 15 | 21 | 56.4 | 19.1 | 53.9 | 2.5 | Yes |
| ST16 | 18 | 59.1 | 16.7 | 56.2 | 2.9 | Yes |
PR: Items from the prone subscale (AIMS); SU: items from the supine subscale (AIMS); Sit: items from the sitting subscale (AIMS); ST: items from the standing subscale (AIMS).
Considering the age at which 50% of the infants passed the item, most of the items from the Brazilian dataset differed by two weeks or less compared with the published Canadian normative data.1 Specifically, 28 items (60%) differed less than two weeks, 16 items (34%) differed between 2.1 and 4 weeks. Only three items showed a difference greater than four weeks (Table 3). The average±SD age difference in weeks between the Brazilian and the Canadian item locations was 1.8±1.2 weeks.
Differences in weeks of item age location in Brazilian and Canadian AIMS datasets.
| Difference in item age location | Number of items | Item location is earlier in Brazilian data | Item location is earlier in Canadian data |
|---|---|---|---|
| <1 week | 15 | 8 | 7 |
| 1–2 weeks | 13 | 3 | 10 |
| 2–3 weeks | 14 | 3 | 11 |
| 3–4 weeks | 2 | 0 | 2 |
| 4–6 weeks | 3 | 2 | 1 |
| Total | 47 | 16 | 31 |
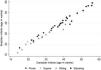
The Pearson correlation coefficient showed an association of 0.99 between the age locations of the set of items from both samples. Fig. 1 illustrates this strong linear relation between datasets.
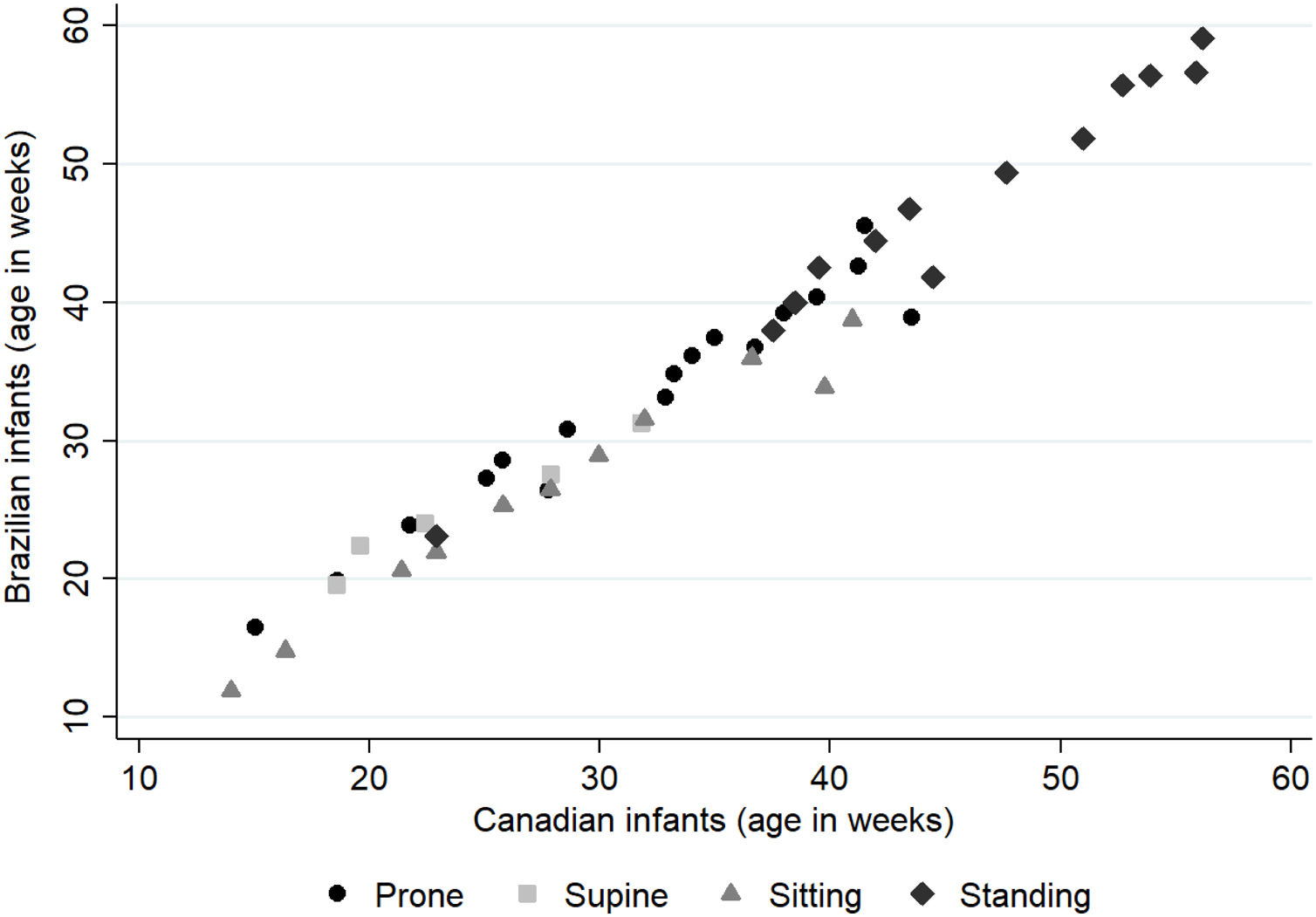
The AIMS normative age locations (in weeks) are re-scaled into Brazilian age locations using the linear equation below:
The age (in weeks) at which 50% of the Brazilian children pass an AIMS item can be estimated, on average, by multiplying 1.03 and subtracting 0.4 from the age (in weeks) reported by the AIMS norms. For example, on average, the estimated age at which Brazilian infants passed Item Prone #5 is 15.2 weeks, which equals the age location from the AIMS norms (15.1 weeks), multiplied by 1.03 and subtracting 0.4. Across the age scale from 0 to 18 months, the average difference between datasets was 0.8 weeks, less than one week.
DiscussionThis study used the AIMS’ item locations strategy to investigate if the Canadian original norms are appropriate for evaluating Brazilian infants. Our results suggest that the AIMS normative data are appropriate to be used in the assessment of Brazilian infants. Both the location of the items and the order of emergence of the gross motor functions were very similar between the two samples. The observed differences were minimal and would not affect either research or clinical decision.
The plotted item locations of the two data sets fall on a straight line. This linear relation confirms the similarities of item location between Canadian and Brazilian infants. Considering the age when 50% of the infants passed an item, most of the items from the Brazilian sample differed by 1 or 2 weeks, compared to the Canadian original sample. According to Darrah et al.,13 if the percentile ranks were moved by one week, it would not interfere with clinical decisions. Considering the four postures of the test, items from supine and sitting showed minor differences between groups.
One important finding from our study is that the difference between the age of emergence of gross motor milestones across the two groups was not systematically in favor of one of the groups. Out of the 47 items, 31 (66%) items appeared slightly earlier in the Canadian sample, while 16 (34%) items appeared slightly earlier in the Brazilian sample. The small magnitude of these minor differences between samples has no clinical relevance. Using the data analyses suggested by Darrah et al.,13 our results are contrary to previous studies comparing the gross motor development of Brazilian infants with the Canadian norms.9,11,12
Previous comparative studies suggested that Brazilian infants exhibited an apparent delay. According to Lopes et al.,11 full-term infants (n=70) from birth to 6 months showed lower percentiles than the AIMS normative values, with most of the Brazilian infants falling at or below the 25th percentile. With similar results, Saccani and Valentini9 reported that Brazilian full-term and preterm infants (n=795) scored lower in 13 out of 18 age groups when compared with the Canadian normative sample. In a previous study10 with 660 infants, differences were identified in the 10th percentile (at 4 months) and in the 5th percentile (at 9 and 10 months) curves. At that time, the use of Brazilian percentile curves was recommended, considering that the suggested AIMS cut-off points for diagnosing or predicting motor delay is the 10th percentile at 4 months of age.14 A recent study involving full-term and preterm infants from different regions of Brazil corroborated with the results of previous studies suggesting that Brazilian infants acquire gross motor milestones at later ages compared to the Canadian infants.12
Although results from previous studies using the percentile ranks argued that Brazilian infants exhibit an age-related delay in gross motor skills evaluated by the AIMS, when applying the logistic regression model and examining item location, as recommended by Darrah et al.,13 these differences were minimal. Our study shows that considering the item location, i.e., the age that 50% of the infants perform the item, the Canadian norms are appropriate for Brazilian infants. A recent study that used this same statistical strategy identified that Dutch infants acquired gross motor skills at a later age compared to the Canadian sample.6 The authors questioned the appropriateness of the AIMS norms to evaluate Dutch infants based mostly on statistical differences rather than on the clinical relevance of such differences. Effectively, for more than 30% of the items that differed between the two samples, the magnitude of the observed differences was very small (e.g., differences of 0.49 or 0.01 week).15 Cross-cultural studies are valuable in identifying determinants of child development that are universal and culture-specific. In such comparisons, statistical inferences must be accompanied and discussed in light of their clinical relevance. In addition, clinical decisions should never be exclusively based on a single assessment score; they must also integrate the concerns of the therapist and the family.
The items that showed greater difference between the two samples were Prone #17 (reciprocal creeping1) and Sitting #10 (sitting to prone). On average, Brazilian infants acquired these two motor skills 4–6 weeks earlier than Canadian infants. It is possible that the year-long Brazilian tropical climatic conditions, which facilitate children to play on the floor, with fewer clothes, may have contributed to the early acquisition of these abilities.
Two items showed a 3–4-week difference between samples. They were Stand #10 (cruising with rotation) and Stand #13 (standing from modified squat). Both items appeared earlier in the Canadian sample. Infants’ acquisition of these two items was nine weeks apart. Although the time of emergence differed between samples, the rhythm of acquisition of these two gross motor skills remained consistent in both Brazilian and Canadian samples.
One strength of our study is the appropriate sample size and adequate representation of preterm infants, as suggested by Darrah et al.13 In their study, a sample size of 675 or greater was suggested to yield valid comparisons with the AIMS norms. It was also recommended that comparison samples include both full-term and preterm infants (age corrected). Our study is the first Brazilian investigation that used logistic regression analyses to examine the cross-country validity of the Alberta Infant Motor Scale norms.
A limitation of this study is that data from Brazilian infants were collected only in one city, located in the southeast region of Brazil (Belo Horizonte city, the capital of Minas Gerais state). Brazil is a large country with regional cultural specificities that may reflect diverse parenting practices, access to early childhood education or daycare, and access to quality health services. Such contextual characteristics may vary within and across the country’s various regions, and they may have an impact on infants’ gross motor development. The generalizability of our results is anchored on the extent to which the gross motor skills of infants from the city of Belo Horizonte are similar to that of infants from other regions of Brazil. Nevertheless, rigorous reproduction of the method proposed by Darrah et al.13 with Brazilian infants may add robustness to this study’s results.
ConclusionThis study showed that the sequence of gross motor development is similar between the two samples and that the Canadian normative values of the AIMS are appropriate for evaluating Brazilian infants.
Conflicts of interestThe authors declare no conflicts of interest.
We want to thank Brazilian parents and their infants for participating in our study. We are grateful to Dr. Johanna Darrah, who provided valuable inputs for this study during data analyses and gave important suggestions on preliminary versions of this manuscript.



