



The Measure of Processes of Care (MPOC) questionnaires evaluate Family-Centered Practice (FCP) in services for children with developmental disorders. The MPOC-20 and MPOC-SP are completed by parents and by rehabilitation professionals, respectively, and are widely used in several countries.
ObjectivesTo translate and cross-culturally adapt the MPOC-20 and MPOC-SP to Brazilian Portuguese and evaluate their reliability and internal consistency.
Methodsthis study included translation, back-translation, cognitive interviews, testing of the pre-final versions, analysis of reliability and of internal consistency of the final versions. Respondents included parents and rehabilitation professionals from rehabilitation centers in four capital cities in Brazil.
ResultsTranslation and cultural-adaptation procedures ensured the Brazilian versions were understandable and semantically equivalent to the original MPOC-20 and MPOC-SP. Pre-final and final versions were analyzed and vetted by the original authors. The MPOC-20 internal consistency Cronbach's alpha varied between 0.61 and 0.91 (n=107), the test-retest reliability ICC varied between 0.44 and 0.83 and the standard error of measurement varied between 0.66 and 0.85 (n=50). The MPOC-SP internal consistency Cronbach's alpha varied between 0.52 and 0.83 (n=92), the test-retest reliability ICC between 0.83 and 0.90, and the standard error of measure between 0.34 and 0.46 (n=62).
ConclusionThe Brazilian versions of the MPOC-20 and the MPOC-SP are in general stable and sufficiently reliable. They are relevant to the evaluation of FCP and provide information that can improve health services and ensure better care.
Rehabilitation has been moving away from medically-centered service toward a focus on the interests and values of patients.1 In this context, Family-Centered Practice (FCP) has emerged as model of pediatric rehabilitation. FCP recognizes parents as the experts in their child's needs.2–5 According to FCP, the care offered to the child must agree with the desires and values of the family.6 FCP promotes partnerships between parents and health professionals.3,4,6 Partnership in decision-making increases children's and parents’ adherence to treatment3,4,6 as well as satisfaction.6,7 FCP can improve service efficiency to promote health and quality of life.8,9
FCP is widely accepted as the best practice in pediatric rehabilitation.8–10 Implementation of FCP requires periodic service evaluations to detect problems, change methods and consolidate procedures.11 Subjective evaluations can be biased by personal beliefs and assumptions,12,13 therefore evaluation of FCP should be based on valid and reliable standardized instruments6,12 for objective longitudinal monitoring.14 Standardized instruments to evaluate FCP have been developed in English-speaking countries.6,11,12 Before these tools can be used in Brazil, they need to be translated and culturally adapted to our context with systematic scientific procedures.15,16 These procedures save time and costs involved in developing and validating new instruments and allow for international comparisons.14,17
The Measure of Processes of Care-56 (MPOC-56) is the first tool developed to evaluate FCP in services for children with developmental problems at all ages.5,6,11,18,19 It is a self-administered questionnaire that evaluates the perceptions of parents about the central tenets of FCP in the care received by their children.6,11,19 Originally developed in Canada, it has been translated and adapted to 12 languages, with good indices of validity and reliability.11,19,20
The MPOC-56 led to the development of a set of self-administered questionnaires measuring complementary aspects of FCP. The MPOC-20 a widely cited19 short version of the original instrument, developed to simplify the assessment of parents’ perceptions in clinical settings. In contrast, the MPOC-Service Providers (MPOC-SP) evaluates central aspects of FCP from the point of view of rehabilitation professionals.11 It is the only instrument available to investigate beliefs and practices of all members of the rehabilitation team.12,13,19 The reliability and validity of the original and international versions of the MPOC-20 and MPOC-SP have been extensively documented.2,6,11,18,19
The MPOC-20 and MPOC-SP complement each other because parents and professionals might have different points of view regarding FCP.19 Together, the two instruments can give a comprehensive and realistic identification of FCP in rehabilitation. Their Brazilian versions could be very useful in research and evaluation of national rehabilitation services. Before they can be used in Brazil, they need to be translated, culturally adapted and tested for psychometric properties. This study reports the translation, cross-cultural adaptation, the test–retest reliability, internal consistency and standard error of measurement for the Brazilian versions of the MPOC-20 and MPOC-SP.
MethodsDescription of the MPOC-20 and MPOC-SPThe MPOC-20 is a self-administered questionnaire with internal consistency of 0.83 to 0.90 (Cronbach's alpha) and test–retest reliability of 0.78 to 0.86 (Intraclass Correlation Coefficient – ICC).2,18 All the 20 questions start with the expression: “In the past year, to what extent do the people who work with your child...” which is followed with, for example: “...help you to feel competent as a parent” or “...provide you with written information about what your child is doing in therapy”. Responses vary from 0 to 7 in a Likert-type scale as follows: 7 – to a very great extent, 6 – to a great extent; 5 – to a fairly great extent; 4 – to a moderate extent; 3 – to a small extent; 2 – to a very small extent; 1 – not at all. Option zero (0) refers to ‘not applicable’.18 The questions are divided into five domains corresponding to key aspects of FCP: Enabling and Partnership, Providing General Information, Providing Specific Information about the Child, Coordinated and Comprehensive Care for Child and Family, Respectful and Supportive Care.6,18,19 Item scores are averaged to compose the final score of each domain.19 High domain scores indicate perception of frequent family-centered behaviors.8
The MPOC-SP is a self-administered questionnaire for professionals with internal consistency of 0.76 to 0.88 and test–retest reliability of 0.79 to 0.99.11 The 27 questions of the MPOC-SP begin with the expression: “In the past year, to what extent did you...”, which is followed with, for example: “...take the time to establish rapport with parents and children?” or “...discuss expectations for each child with other service providers, to ensure consistency of thoughts and action?”. Response options are the same as MPOC-20. The questions are divided into four domains: Showing Interpersonal Sensitivity, Treating People Respectfully, Communicating Specific Information About the Child and Providing General Information.11,13,19 Each domain has its own average score. Higher scores reflect greater focus of the service on the patient and family.8
Translation and cross-cultural adaptationThe process included six stages after authorization from the CanChild Centre for Childhood Disability Research at McMaster University, Canada.20 This study was approved by the Research Ethics Committee of Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil (CAAE: 74097417.7.1001.5149). All participants signed the Informed Consent Term
In the first stage, two Brazilian translators with different backgrounds (a university professor and a clinician) who were proficient in English and experienced in rehabilitation (both were physical therapists) independently translated the original instruments from English to Portuguese. Then an Expert Committee with three university professors from physical and occupational therapy departments (two who were experienced with translation and cultural adaptation of standardized instruments, one who was certified and experienced as an English teacher and had performed the translation) and two physical therapists (one who was the second translator) compared the two translations and produced a unified version. In the third stage, this version was sent to two professional translators. They were native English speakers who were also fluent in Portuguese; they worked independently of each other and did not know or consulted the original versions of the instruments. They translated the unified Brazilian version back into English (back-translation).15,16 In the fourth stage, two professors (from the physical therapy department) and a physical therapist from the Expert Committee worked with the back-translators and compared the back-translations with the Brazilian and the original version. The Committee also discussed conceptual, idiomatic, semantic and cultural correspondence for each item. The panel worked on best solutions to solve the discrepancies between the Portuguese and English versions of the MPOC-20 and MPOC-SP and produced a unified back-translated version of each. The resulting Brazilian versions as well as the unified back-translations were sent to and approved by CanChild. The Brazilian versions were tested at the fifth stage to ensure that users understood the contents of the MPOC-20 and MPOC-SP.
The pre-final versionsThe fifth stage involved cognitive interviews, which consisted of two techniques. In the ‘think aloud’ technique, the participant is asked to describe what he/she thought when reading the item.21,22 Direct probing’ was used to identify items that were difficult to understand. In this technique, the interviewer asked: “Can you tell me in your words what this question was asking?”.21,22
A physical therapist and two students interviewed parents or family members about their understanding of the MPOC-20, and rehabilitation professionals about the MPOC-SP. After a round of three interviews for each instrument, the interviewers and a university professor analyzed the responses, adjusted the wording and added examples as necessary. To guarantee that meaning was not altered, all changes were submitted to and vetted by the Expert Committee and CanChild. Procedures are detailed in a recent publication.23 Three rounds of interviews were necessary to fully eliminate comprehension problems for each instrument.21,22 All 18 respondents were selected by convenience at the General Hospital of UFMG.
The MPOC-20 and MPOC-SP adjusted Brazilian versions were then tested as recommended internationally.15 Participants were 30 parents and 30 rehabilitation professionals from the SARAH Network in Belo Horizonte. They were interviewed about their understanding of each item and the reason for their response choice. Only if 15% or more of the respondents had any doubts in any of the items, would it be rewritten and a new round of testing carried out.15 At this phase, we noted that some parents felt more comfortable being orally interviewed rather than filling in the self-administered questionnaire. For the next phase, each parent chose his or her preferred format. All professionals used the self-administered format.
Evaluation of the measurement propertiesAt the final sixth stage, the internal consistency was determined with 107 and 92 respondents for the MPOC-20 and MPOC-SP, respectively. To determine test–retest reliability and the standard error of measurement, the questionnaires were applied twice to a subset of 50 and 62 parents and professionals, respectively, 7 to 14 days apart to avoid memory bias. The Brazil-ABEP Economic Classification Criteria were used to describe their socioeconomic level.24
For this phase of the study, parents or caretakers of children under 12 years of age were selected by convenience. The children were in treatment for at least one year (as outpatient or inpatient) in one of the hospitals of the Sarah Network. Professionals working with children's rehabilitation for at least one year were also selected, including 3 physical therapists from the Associação Mineira de Reabilitação in Belo Horizonte and other professionals (physical therapists, pediatricians, occupational therapists, pedagogues, nurses, physical educators, speech therapists, psychologists, social workers and dietitians) from the Sarah Hospitals in Rio de Janeiro, Belo Horizonte, Salvador and São Luís.
Statistical analysisReliability indices were determined using intra-class correlation coefficients (ICC3,1) with the ICCagreement model. Reliability values were classified as poor (<0.4), moderate (0.4–0.75) or excellent (>0.75).25 For each domain of each instrument, the Cronbach's alpha as used as an index of internal consistency. The Cronbach's alpha is a measure of how closely related a set of items are as a group. Values between 0.70 and 0.90 indicate a good correlation between items.26 The standard error of measurement was calculated for the total score of each domain, for each instrument. The Statistical Package for Social Sciences version 18.0 (2011) was used for all analyses.
ResultsTranslation and cross-cultural adaptationSome wording was adapted by the Expert Committee to reflect terms commonly used in Brazilian Portuguese. The response options for both instruments in the original version included options ranging from 7 (to a very great extent) to 1 (not at all). Because the direct translation would involve unusual wording (e.g. ‘em bastante grande medida’), the options were translated as follows: 7 (totally), 6 (very much); 5 (plenty); 4 (more or less); 3 (little); 2 (very little), 1 (not at all). ‘Parents’ was changed to the more inclusive expression ‘mothers and fathers’ in the MPOC-20. ‘Circling’ was changed to ‘Marking’, which is the most commonly used action to indicate answers in a form. In question 20 of the MPOC-20, “organization's parent resource library” was replaced by “web pages and parent associations” because resource libraries are uncommon in Brazil. In the description of the type of services evaluated by the MPOC-SP, the expression “community care facility” was replaced by a list of Brazilian institutions that usually provide care to children: rehabilitation clinics and hospitals, primary health care units and rehabilitation centers. ‘Disability’ was translated to ‘Deficiência’, in line with previous Brazilian translations of the International Classification of Functioning, Disability and Health.27 Finally, in the absence of a literal translation for “nonjudgmental way”, the expression “without any judgment of values” was used. These amendments were approved by CanChild.
Pre-final and final versionsCognitive interviews indicated the need to change wording and give examples to avoid difficulties in understanding the questions. Eight questions were modified in each instrument. A detailed report of the interview procedures and all ensuing changes is available in Vaz et al.23 To guarantee that the changes in wording and addition of examples did not affect original content, all modifications were analyzed and vetted by CanChild. For example, question 11 of the MPOC-20 asked: “In the past year, to what extent do the people who work with your child treat you as an equal rather than just as the parent of a patient (e.g., by not referring to you as “mom” or “dad”)?”. In the Brazilian version, the example was changed to “(e.g., by calling you and your child by the name)?”
The translated and cross-culturally adapted versions of the instruments were then tested with 30 caretakers and 30 rehabilitation professionals to detect doubts. Caretakers included 28 mothers, one grandmother and one aunt with age varying between 17 and 57 (33.7±9.36). Their socioeconomic status varied from A to D/E. Professionals included 15 nurses, 6 physicians, 5 physical therapists, 1 speech therapist, 1 clinical psychologist, 1 nursing assistant and 1 orthopedic workshop technician aged between 35 and 56 years (44.4, ±6.70) with socioeconomic status varying between A and B2. Because less than 15% of the interviewees had doubts in any specific item, none of the items had to be rewritten and re-tested.15 Please refer to Appendices I and II for the final translation of the questions of each instrument to Brazilian Portuguese (approved by CanChild).
Evaluation of measurement propertiesTable 1 contains characteristics of the 107 caretakers and 92 professionals whose resposnses were used to determine measurement properties of the MPOC-20 and MPOC-SP, respectively. Internal consistency of the MPOC-20 varied between 0.61 and 0.91. Test–retest reliability (ICC3,1) varied between 0.44 and 0.84 for the five domains. The standard error of measurement varied between 0.66 and 0.85 (Table 2). Internal consistency of the MPOC-SP varied between 0.52 and 0.83. Test–retest reliability (ICC3,1) varied between 0.83 and 0.97 for the four domains. The standard error of measurement varied between 0.34 and 0.46 (Table 2).
Characteristics of MPOC-20 and MPOC-SP respondents.
| Parents or caretakers | ||
| Age (years) | 35.7±5.6, 19–71 | |
| Sex | Male | 7 (6.5) |
| Female | 100 (93.4) | |
| Family relationship | Mother | 92 (85.9) |
| Father | 6 (5.6) | |
| Other | 9 (8.4) | |
| Education | Higher education or above | 17 (15.8) |
| High school complete | 55 (51.4) | |
| High school incomplete | 8 (7.4) | |
| Elementary school complete | 13 (12.1) | |
| Elementary school incomplete | 12 (11.2) | |
| Family income | Less than 1 minimum wage | 48 (44.8) |
| 1–2 minimum wages | 31 (28.9) | |
| 2–5 minimum wages | 19 (17.7) | |
| Above 5 minimum wages | 9 (8.4) | |
| Socioeconomic status (Brazil-ABEP criteria) | A | 3 (2.8) |
| B1 | 9 (8.4) | |
| B2 | 19 (17.7) | |
| C1 | 24 (22.4) | |
| C2 | 33 (30.8) | |
| D/E | 19 (17.7) | |
| Child age (years) | 6.7±2.1, 1–12 | |
| Child sex | Female | 42 (39.2) |
| Male | 65 (60.7) | |
| Child diagnosis | Cerebral palsy | 49 (45.7) |
| Myelomeningocele | 27 (21.4) | |
| Club-foot | 7 (6.5) | |
| Zikavirus microcephaly | 7 (6.5) | |
| Other | 17 (15.8) | |
| Service providers | ||
| Age (years) | 41.7±8.4, 32–58 | |
| Sex | Male | 12 (13) |
| Female | 80 (86.9) | |
| Profession | Physical therapist | 24 (26.0) |
| Occupational therapist | 7 (7.6) | |
| Physician | 20 (21.7) | |
| Physical educator | 9 (9.7) | |
| Pedagogue | 6 (6.5) | |
| Social worker | 2 (2.1) | |
| Psychologist | 9 (9.7) | |
| Speech therapist | 2 (2.1) | |
| Dietician | 3 (3.2) | |
| Nurse | 10 (10.8) | |
| Time in service | 12.1±5.6, 1–30 | |
| Educational degree | Graduate | 32 (34.7) |
| Specialist | 44 (47.8) | |
| Master | 13 (14.1) | |
| Doctorate | 2 (2.1) | |
| Post-doctorate | 1 (1) | |
| Socioeconomic status (Brazil-ABEP criteria) | A | 46 (50) |
| B1 | 29 (31.5) | |
| B2 | 17 (18.4) | |
Data are means ± standard deviation, frequency (proportion) and range (lowest-highest value).
Internal consistency and reliability of the Brazilian versions of the MPOC-20 and MPOC-SP.
| Domain | MPOC 20 | ||
|---|---|---|---|
| α | ICC3,1(95%CI) | SEM | |
| EP | 0.612 | 0.44 (0.33–0.53) | 0.665 |
| PGI | 0.912 | 0.83 (0.80–0.87) | 0.735 |
| PSI | 0.845 | 0.73 (0.65–0.79) | 0.858 |
| CC | 0.662 | 0.49 (0.38–0.59) | 0.726 |
| RSC | 0.738 | 0.58 (0.47–0.68) | 0.737 |
| Domain | MPOC SP | ||
|---|---|---|---|
| α | ICC3,1(95%CI) | SEM | |
| CSI | 0.523 | 0.90 (0.88–0.93) | 0.345 |
| PGI | 0.797 | 0.85 (0.85–0.88) | 0.437 |
| IS | 0.835 | 0.83 (0.80–0.85) | 0.369 |
| RT | 0.805 | 0.89 (0.87–0.91) | 0.467 |
α, Cronbach's alpha; ICC, Intraclass Correlation Coefficient; CI, Confidence Interval; SEM, Standard Error of Measurement; EP, Enabling and Partnership; PGI, Providing General Information; PSI, Providing Specific Information; CC, Coordinated and Comprehensive Care; RC, Respectful and Supportive Care; CSI, Communicating Specific Information; PGI, Promoting General Information, IS, Interpersonal Sensitivity; RT, Respectful Treatment.
The lowest internal consistency value was observed for the domain “Providing Specific Information” of the MPOC-SP”, which is formed by questions 14, 15 and 16. Further analysis indicated that origin of the low internal consistency was the fact that the responses to question 15 had a wider dispersion (were more varied between respondents) than questions 14 and 16. In Fig. 1, histograms show the frequency distribution for responses of each question.
Discussion”.")
This study reports the translation and cross-cultural adaptation of the MPOC-20 and MPOC-SP to Brazilian Portuguese, following internationally recommended guidelines.15,16,26 Interviews were used guarantee appropriate understanding of each question. All adaptations were analyzed and vetted by an Expert Committee and authors of the original instruments, and ensured semantic equivalence between translated and the original versions. Assessment with respondents from different regions of Brazil ensured representativeness of the target population, given our wide cultural and linguistic diversity.17
In the beginning of the translation phase the panel of experts foresaw that the objectives of the questionnaires could be difficult to understand. Empowerment and active participation of patients are still incipient in Brazil.23,28 However, parents and professionals understood the content and objective of the questions and expressed satisfaction for being asked about FCP concepts and values. They reiterated the importance of FCP in rehabilitation services.
The Committee was also concerned that the interviewees would find it difficult to distinguish response options on a 7-point scale. This problem had occurred in the adaptation of the MPOC-20 in South Africa; the African versions thus was modified to have fewer response options.29 The Brazilian interviewees, however, did not have any doubts about response options, and all of them were retained.
Some adjustments or substitutions of wording were necessary. For example, “organization's parent resource library”, “community care facility” and “nonjudgmental way” were changed to words with equivalent concepts. In Brazil, the translation for “parents” is the word “pais”, that also means “fathers”. The Committee chose to use “mothers and fathers” in the MPOC-20 because mothers usually accompany their children to the health services. To value respect and partnership, mothers deserved due recognition; therefore, the word “mother” was added to the translation.
Because of responses to the cognitive interviews, we added examples to some questions. We intended to preserve their original meanings, but also allow the interviewees to link their content to their practical implications for professional–patient interactions. For instance, in the question “... helped you feel competent as a mother or father?” we added the following example: “eg., by praising and encouraging you”. Cognitive interviews are uncommon in translation and adaptation studies, but we believe they were fundamental for the elaboration of the Brazilian MPOC versions.
In this study, the MPOC questionnaires were applied in two different formats, self-application or interview, to accomodate for the heterogeneity of the respondents. A South African study also used the interview format29 because many patients were unfamiliar with self-administered questionnaires and had different levels of education.30–32 The interview format is also inclusive of individuals with visual problems (two mothers in this study). Format flexibility can widen applicability of the instruments.
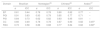
We tested measurement properties after language and format flexibilization. See Tables 3 and 4 for comparisons between Brazilian and other versions of the MPOC-20 and MPOC-SP. In general, internal consistency and test–retest reliability were moderate to good and were comparable to values found for other versions of the instruments, indicating stability of the translated versions. The two exceptions were the domains “Enabling and Partnership” and “Coordinated and Comprehensive Care” of the MPOC-20, that showed low internal consistency and low reliability. These results may be related to specificites of Brazil and the drastic variation of education levels in the patient population. Note that reliability values were consistently higher for MPOC-SP, directed to rehabilitation professionals. When applying the MPOC-20, Brazilian service managers should interpret results of the two domains with caution, or establish reliability values for their service's target respondents. Other domains of the instrument are unaffected and can be used reliably.
Consistency (α) and reliability (ICC) of the Brazilian MPOC-20 version compared to other versions.
| Domain | Brazilian | Norwegian35 | Chinese36 | Arabic37 | ||||
|---|---|---|---|---|---|---|---|---|
| α | ICC | α | ICC | α | ICC | α | ICC | |
| EP | 0.61 | 0.44 | 0.78 | 0.78 | 0.80 | 0.82 | 0.77 | – |
| PGI | 0.91 | 0.83 | 0.93 | 0.79 | 0.85 | 0.77 | 0.71 | – |
| PSI | 0.84 | 0.73 | 0.62 | 0.82 | 0.83 | 0.85 | 0.81 | – |
| CC | 0.66 | 0.49 | 0.78 | 0.78 | 0.87 | 0.80 | 0.82 | 0.45a |
| RSC | 0.73 | 0.58 | 0.86 | 0.88 | 0.77 | 0.84 | 0.82 | 0.68a |
α, Cronbach's alpha; ICC, Intraclass Correlation Coefficient.
EP, Enabling and Partnership; PGI, Providing General Information; PSI, Providing Specific Information about the child; CC, Coordinated and Comprehensive Care; RSC, Respectful and Supportive Care
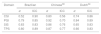
Consistency (α) and reliability (ICC) of the Brazilian MPOC-SP version compared to other versions.
| Domain | Brazilian | Chinese38 | Dutch39 | |||
|---|---|---|---|---|---|---|
| α | ICC | α | ICC | α | ICC | |
| CSI | 0.52 | 0.90 | 0.80 | 0.56 | 0.74 | 0.86 |
| PGI | 0.79 | 0.85 | 0.92 | 0.70 | 0.84 | 0.89 |
| SIS | 0.83 | 0.83 | 0.86 | 0.76 | 0.65 | 0.83 |
| TPS | 0.80 | 0.89 | 0.87 | 0.77 | 0.66 | 0.83 |
α, Cronbach's alpha; ICC, Intraclass Correlation Coefficient.
CSI, Communicating Specific Information; PGI, Providing General Information; SIS, Showing Interpersonal Sensitivity; TPS, Treating People Respectfully.
The low internal consistency found for the domain “Providing Specific Information” of the “MPOC-SP” is probably a result of the wide dispersion of the answers observed in question 15. For this question, answers were more varied than for questions 14 and 16, which belong to the same domain. Question 15 asks: “In the past year, to what extent did you provide parents with written information about their child's health condition, progress or treatment?”. In Brazil, physicians usually provide written information (such reports and prescriptions). Some professionals may have thought of “written information about their child's health condition” to refer to medical documents, while others might have included educational materials in their reasoning, causing the variability of the responses. We believe the internal consistency value reflects the Brazilian context, not the quality of the domain questions, because the respondents did not report any doubts about this question in any phase of the study. Additionally, the test–retest reliability of question 15 was classified as excellent26 (ICC=0.84 (0.75–0.90)). Thus, translation of question 15 was stable and needed no further adjustments.
In general, the low values of the standard error of measurement (below 0.85) indicate small dispersion of the measurement errors in the estimation of the true scores from observed scores.26 Thus, a clinician or manager can be quite confident that the true scores for a given application of the Brazilian-Portuguese MPOC-20 and MPOC-SP are within less than a point below or above the scores obtained for each domain. These results show that the instruments have adequate reliability.
The full versions of MPOC-20 and MPOC-SP in Brazilian Portuguese are now available through the CanChild website for Brazilian rehabilitation services to either assess a course of treatment provided to a specific family, or to assess the general quality of services provided by the institution.33 For example, the MPOC-SP could be used before and after structural service changes to detect whether they had any impact on the behavior of the rehabilitation team.34 The MPOC-SP and MPOC-20 are self-administered questionnaires, therefore they can be sent in print or electronic forms to potential respondents. Privacy and anonymity in responding can help individuals feel safe to critically assess the services. Interviews were also feasible within 30min; thus their use is attainable in routine activities.
In general, our results are in agreement with other studies that translated and adapted the MPOC versions.35–39 The MPOC-SP and MPOC-20 Brazil are standardized instruments with adequate psychometric properties.6,14 The instruments evaluate FCP, widely accepted as the “best practice” in pediatric rehabilitation.8–10,12,19 They could be used for periodic service evaluations13 informing on patients’ and professionals’ perceptions. The two instruments complement each other and are valuable to plan better care.40
ConclusionsThe present study reports the translation, cultural adaptation, and evaluation of the psychometric properties of the Brazilian versions of the MPOC-20 and MPOC-SP. The instruments are culturally appropriate and mostly reliable. The two domains of the MPOC-20, “Enabling and Partnership” and “Coordinated and Comprehensive Care” must be used with care. The MPOC-20 and MPOC-SP may be used to help improve the efficiency of rehabilitation services provided to children and families.
Conflicts of interestThe authors declare no conflicts of interest.
We thank all family members and rehabilitation professionals who agreed to participate in this study. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
The following are the supplementary data to this article:




