
To analyze the measurement properties of the Brazilian-Portuguese version of the Tampa Scale for Kinesiophobia-11 in patients with fibromyalgia.
MethodsAssessment was made at three time points: baseline (n=130) and 15 days (n=54) and eight weeks after baseline (n=51). Data collected at baseline were used to assess internal consistency, criterion and construct validity, and ceiling and floor effects. Data collected at baseline and 15 days after baseline were used to assess reliability and measurement error, and data collected before and after an eight-week exercise-based physical therapy intervention were used to assess interpretability of change scores.
ResultsThe Tampa Scale for Kinesiophobia-11 showed adequate internal consistency (Cronbach's alpha=0.77; alpha if item deleted: 0.74–0.77), substantial reliability (intraclass correlation coefficient2,1=0.85; 95% confidence interval: 0.75, 0.90), good measurement error (standard error of measurement: 2.65 points), and a minimal detectable change (90% confidence) of 6.16 points. For validity, the Tampa Scale for Kinesiophobia-11 showed a positive and good correlation with the original Tampa Scale for Kinesiophobia (r=0.84, p<0.01), positive and moderate correlation with the Pain Catastrophizing Scale (r=0.55, p<0.01), positive and weak correlation with the Numerical Pain Rating Scale (r=0.25, p<0.01), positive and moderate correlation with the Beck Depression Inventory (r=0.39, p<0.01), and no correlation with the Patient-Specific Functional Scale (r=0.11, p=0.23). Kinesiophobia, pain, function, catastrophizing, and depression statistically improved after the eight-week intervention (p<0.01).
ConclusionThe Tampa Scale for Kinesiophobia-11 is consistent, reliable, and appropriate to assess fear of movement in patients with fibromyalgia in the clinical context. Responsiveness of the Tampa Scale for Kinesiophobia-11 should be tested in future studies.
Individuals with chronic musculoskeletal pain have different types and extent of emotional, cognitive, and behavioral response to pain.1 Among these responses, fear related to perceived threatening situations may be most significant. Patients with high levels of fear view pain as a sign of injury and any activity that causes or has the potential to cause pain2 is interpreted as dangerous.3 The fear, avoidance, anxiety, and pain model is the most used to explain the cycle that contributes to pain chronification.3
Kinesiophobia is defined as an excessive, irrational, and debilitating fear of movement and physical activity, resulting from the feeling of vulnerability to painful or new injuries.4 Kinesiophobia was identified in 60% of patients with chronic musculoskeletal pain,5 with a negative impact on function in patients with chronic low back pain,6 knee osteoarthritis,7 and chronic shoulder pain.8 Kinesiophobia is commonly found in patients with fibromyalgia due to the association between pain/fatigue and movement, which consequently reduces the level of physical activity, increases disability, and perpetuates pain.3,9,10
The Tampa Scale for Kinesiophobia (TSK) is the most widely used self-report questionnaire for evaluating kinesiophobia in patients with chronic pain.4 The TSK has already been translated into Brazilian-Portuguese and validated for patients with chronic low back pain.11 In 2005, a shorter version was created that excludes six items with inadequate measurement properties. Four items (4, 9, 12, and 14) were removed because their answers did not fit a normal distribution pattern and two (8 and 16) because they seemed to measure different constructs than the other items. Thus, the 11-item version known as the Tampa Scale for Kinesiophobia-11 (TSK-11) was created.12
The TSK-11 has measurement properties similar to the original version, with the advantage of being shorter and simpler.12 In addition, the TSK-11 is validated for patients with chronic low back pain,12 chronic musculoskeletal pain in older adults,13 and in adults.14 The assessment of kinesiophobia in patients with fibromyalgia may be important to properly design rehabilitation strategies and goals in this population. However, the measurement properties of the TSK-11 in patients with fibromyalgia have not yet been determined. Therefore, the objective of this study was to establish the reliability, interpretability, and criterion and construct validity of the Brazilian-Portuguese version of the TSK-11 in patients with fibromyalgia.
MethodsThis study was approved by the Research Ethics Committee of Universidade Cidade de São Paulo (UNICID), São Paulo, SP, Brazil under number 51328215.1.0000.0064, and authorized by the original author12 of the TSK-11 via direct electronic communication.
ParticipantsOne hundred and thirty participants were recruited through advertisements on local websites and newspapers. After the baseline assessment, participants were divided into two samples: 79 were invited to participate in a second assessment 15 days later, and 51 were included in an ongoing randomized controlled trial15 and received a physical therapy intervention for eight weeks. We included individuals who could read and write in Brazilian-Portuguese and met the 2010 American College of Rheumatology diagnostic criteria for fibromyalgia16: Widespread Pain Index (WPI) greater than or equal to 7 and Symptom Severity Score (SSS) greater than or equal to 5, or WPI between 3 and 6 and SSS greater than or equal to 9, absence of any other disease that explained the symptoms, and presence of pain for at least three months.
The exclusion criteria were the following: uncontrolled systemic diseases (diabetes mellitus, systemic arterial hypertension, and thyroid dysfunction); neurological, cardiorespiratory, and musculoskeletal conditions that could interfere with treatment, such as paralysis, significant changes in sensory function, or changes in the level of cognitive function and understanding; advanced joint diseases (e.g., severe arthrosis, hip or knee arthroplasty, severe rheumatoid arthritis, neck pain with referred pain to upper limbs); injury or severe pain in the lower limb joints that limited aerobic exercise (e.g., meniscal injury, plantar fasciitis); partial or total muscle tear; amputations; recent surgery; and pregnancy. All patients included in the study signed an informed consent form prior to participation.
ProceduresAt baseline assessment, personal, anthropometric, and clinical data were collected for sample characterization. All participants completed the TSK, the TSK-11, the Numerical Pain Rating Scale (NPRS), the Patient-Specific Functional Scale (PSFS), the Pain Catastrophizing Scale (PCS), and the Beck Depression Inventory (BDI). Data collected at baseline assessment were used to assess internal consistency, construct and criterion validity, and ceiling and floor effects. After 15 days, the patients completed the TSK-11 again for the assessment of reliability and measurement error – with the assumption that no change in status would have occurred in 15 days and that the window of time was sufficient to minimize recall. Finally, eight weeks after the baseline assessment, those patients who underwent physical therapy treatment completed the same questionnaires administered at baseline assessment, to assess interpretability of change scores.
QuestionnairesThe TSK consists of 17 questions that assess fear of movement. The score for each item ranges from 1 to 4, where 1 represents “strongly disagree”, 2 “somewhat disagree”, 3 “somewhat agree”, and 4 “strongly agree”. For the final score, it is necessary to reverse the scores of questions 4, 8, 12, and 16. The total score varies between 17 and 68 points, and a higher score represents greater kinesiophobia.11,17
The TSK-11 is composed of 11 items of the TSK, scored in the same manner as described for the 17-item scale. The final score of the scale is calculated by adding the scores of the items and ranges from 11 to 44 points with a higher score representing greater kinesiophobia.12 The TSK has already undergone the process of translation and cross-cultural adaptation to Brazilian-Portuguese, therefore it was not necessary to repeat the translation and cross-cultural adaptation phase for the TSK-11 as it is simply a subset of the questions in the original version.
The NPRS was used for the individual to indicate their average pain over the past seven days. It consisted of an 11-point scale, ranging from 0 to 10, where 0 was “no pain” and 10 was “the worst possible pain”.18
For the PSFS, the individual identifies three primary activities he or she felt unable to do or had difficulty with because of fibromyalgia. Next, the individual rates their ability to perform the identified activities on an 11-point scale, where 0 represents “unable to perform the activity” and 10 represents “able to perform the activity at preinjury level”. The average score for the three activities is then calculated with a higher score indicating better function.18
The PCS is a 13-item scale with three domains: helplessness, magnification, and rumination. It is designed to assess the degree of catastrophization, thoughts, and feelings that patients develop when they are in pain. Each item is scored from 0 to 4 points, where 0 represents “not at all”, 1 “to a slight degree”, 2 “to a moderate degree”, 3 “to a great degree”, and 4 “all the time”. The total score is the sum of all items, ranging from 0 to 52 points. The higher the score, the higher the level of catastrophizing about pain.19
The BDI consists of 21 items that assess depressive symptoms in the last week, including the day of assessment. The answer for each item contains statements about the symptoms that are rated on an ordinal scale from 0 to 3, and the sum of the items results in the total score, which ranges from 0 to 63 points. Severity levels are classified according to the final score as “no depression” or “minimal depression” (from 0 to 13), “mild depression” (from 14 to 19), “moderate depression” (from 20 to 28), or “severe depression” (from 29 to 63).20
All questionnaires used have already been translated and validated to Brazilian-Portuguese. The PSFS and the NPRS were tested on patients with acute low back pain and had substantial to excellent reliability, with intraclass correlation coefficient (ICC) and 95% confidence interval (95% CI) of 0.85 (0.77, 0.90) and 0.94 (0.90, 0.96), respectively.18 The PSFS was considered more responsive than other functional capacity assessment scales in terms of its correlation with the change measured by the Global Perceived Effect Scale (r=0.34, p<0.01).18 The PCS was tested on patients with chronic musculoskeletal pain and showed adequate internal consistency and excellent reliability, with a Cronbach's alpha of 0.91 (0.93 for helplessness, 0.88 for magnification, and 0.86 for rumination) and ICC of 0.92 (95% CI: 0.91, 0.94).19 The BDI showed adequate internal consistency and substantial reliability in community-dwelling patients, with a Cronbach's alpha of 0.93 and ICC of 0.89 (95% CI: 0.82, 0.93).20
InterventionAll patients received the intervention recommended by the guidelines, composed by an educational booklet with information on fibromyalgia, self-care strategies, and exercises.21–23 The treatment consisted of aerobic exercises or modified Pilates exercises performed twice a week in 60-min sessions over a period of eight weeks. Patients who performed aerobic exercise could choose between using a treadmill or stationary bike, maintaining exercise intensity between 57% and 76% of their maximum heart rate.24–26 Perceived exertion for both exercise approaches was monitored using the Borg Perceived Exertion Scale27 with the goal to maintain perceived exertion between 10 and 1228 out of 20. More details about the treatment can be found elsewhere.15
Analysis of measurement propertiesThe analyses had the required number of participants and classifications for each measurement property.29,30 Internal consistency was analyzed using Cronbach's alpha and alpha if item deleted. Alpha values greater than or equal to 0.70 and less than 0.95 were considered adequate.31 Reliability was calculated using ICC type 2,1 and 95% CIs. ICC values lower than 0.40 represent poor reliability, between 0.40 and 0.75 represent moderate reliability, between 0.75 and 0.90 represent substantial reliability, and greater than 0.90 represent excellent reliability.29 Measurement error was calculated using two methods: standard error of measurement (SEM) and minimal detectable change (MDC). The SEM is expressed in the units of measurement of the scale. To obtain the SEM, the standard deviation of the mean of the differences was divided by the square root of 2 (standard deviation of mean differences/√2).32 The percentage of SEM related to the total scale score was interpreted as very good when ≤5%, good when >5% and ≤10%, doubtful when >10% and ≤20%, and poor when >20%.31 The MDC was calculated using the formula MDC=1.645×√2×SEM, which reflects a 90% CI. Values higher than the MDC characterize a change in a patient's score that is above measurement error.31
Construct validity was assessed using Pearson's correlation test, in which r<0.30 indicated a weak correlation, r≥0.30 and <0.60 indicated a moderate correlation, and r≥0.60 indicated a good correlation.33 The correlation was performed between the total scores for the TSK-11 and the total scores for the PCS, NPRS, BDI, and PSFS. Criterion validity can be assessed when there is a gold standard available for the measure. For a patient-reported outcome measure, the long version of an instrument can be considered an acceptable gold standard for the short version of the same instrument.30 Thus, criterion validity was assessed using the correlation between the TSK and the TSK-11. The hypotheses for validity were that the Brazilian-Portuguese version of the TSK-11 would have a positive and good correlation with the PCS, positive and moderate correlation with the NPRS and the BDI, negative and moderate correlation with the PSFS, and a positive correlation greater than 0.70 with the TSK.29,33
Interpretability of the change scores for kinesiophobia, pain, function, catastrophizing, and depression was analyzed with data collected from the 51 patients who received treatment. Paired T-test was used to compare the differences between baseline and eight weeks after baseline assessments. The ceiling and floor effects evaluated the percentage of patients who obtained the maximum and minimum scores on the scale. This effect was considered present when more than 15% of the sample obtained the maximum (ceiling) or minimum (floor) score on the questionnaire.31,34
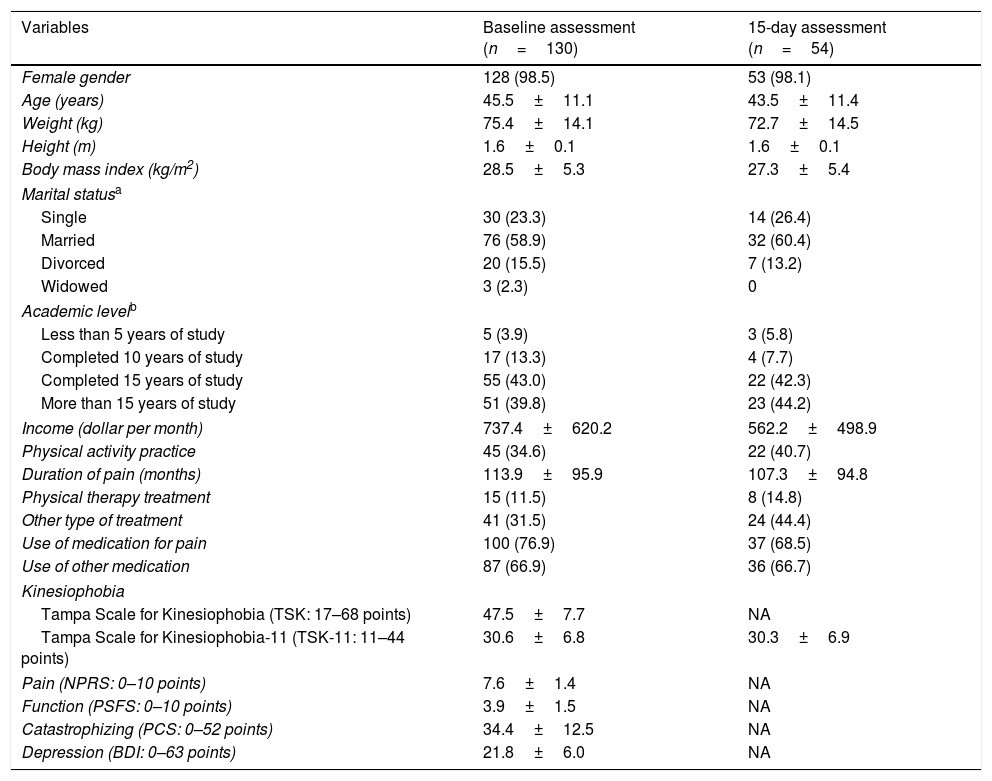
ResultsOne hundred and thirty participants were assessed at baseline for the analysis of internal consistency, construct and criterion validity, and ceiling and floor effects. From this initial group, 54 of the 79 participants invited to participate in the follow-up assessment completed the TSK-11 15 days later. These data were used for the analysis of reliability and measurement error of the TSK-11. Twenty-five participants did not return for assessment at 15 days and their data were used only for the baseline assessment. The demographic and clinical characteristics of the patients included at baseline are described in Table 1, with 11.5% of them receiving physical therapy care and 31.5% receiving other treatments, such as medication (16.9%), and alternative therapies such as acupuncture (6.9%). In the broad category of pain medications, use of muscle relaxants was the most often reported (30.9%), and among other medication, use of antidepressants was the most often reported (69.4%).
Characteristics of the study participants.
| Variables | Baseline assessment (n=130) | 15-day assessment (n=54) |
|---|---|---|
| Female gender | 128 (98.5) | 53 (98.1) |
| Age (years) | 45.5±11.1 | 43.5±11.4 |
| Weight (kg) | 75.4±14.1 | 72.7±14.5 |
| Height (m) | 1.6±0.1 | 1.6±0.1 |
| Body mass index (kg/m2) | 28.5±5.3 | 27.3±5.4 |
| Marital statusa | ||
| Single | 30 (23.3) | 14 (26.4) |
| Married | 76 (58.9) | 32 (60.4) |
| Divorced | 20 (15.5) | 7 (13.2) |
| Widowed | 3 (2.3) | 0 |
| Academic levelb | ||
| Less than 5 years of study | 5 (3.9) | 3 (5.8) |
| Completed 10 years of study | 17 (13.3) | 4 (7.7) |
| Completed 15 years of study | 55 (43.0) | 22 (42.3) |
| More than 15 years of study | 51 (39.8) | 23 (44.2) |
| Income (dollar per month) | 737.4±620.2 | 562.2±498.9 |
| Physical activity practice | 45 (34.6) | 22 (40.7) |
| Duration of pain (months) | 113.9±95.9 | 107.3±94.8 |
| Physical therapy treatment | 15 (11.5) | 8 (14.8) |
| Other type of treatment | 41 (31.5) | 24 (44.4) |
| Use of medication for pain | 100 (76.9) | 37 (68.5) |
| Use of other medication | 87 (66.9) | 36 (66.7) |
| Kinesiophobia | ||
| Tampa Scale for Kinesiophobia (TSK: 17–68 points) | 47.5±7.7 | NA |
| Tampa Scale for Kinesiophobia-11 (TSK-11: 11–44 points) | 30.6±6.8 | 30.3±6.9 |
| Pain (NPRS: 0–10 points) | 7.6±1.4 | NA |
| Function (PSFS: 0–10 points) | 3.9±1.5 | NA |
| Catastrophizing (PCS: 0–52 points) | 34.4±12.5 | NA |
| Depression (BDI: 0–63 points) | 21.8±6.0 | NA |
Continuous variables are expressed as mean±standard deviation and categorical variables as frequency (proportion).
Values valid for 128 participants at baseline assessment and 52 at the 15-day assessment.
NA, not assessed.
Higher scores in the Tampa Scale for Kinesiophobia (TSK), Tampa Scale for Kinesiophobia-11 (TSK-11), Numerical Pain Rating Scale (NPRS), Pain Catastrophizing Scale (PCS), and Beck Depression Inventory (BDI) indicate a worse condition, and higher scores in the Patient-Specific Functional Scale (PSFS) indicate better function.
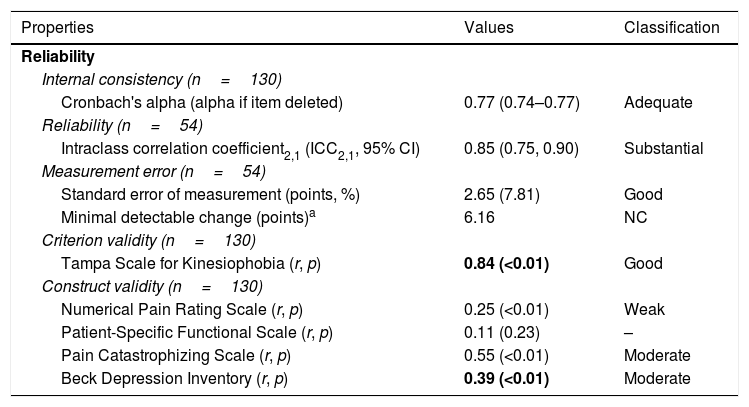
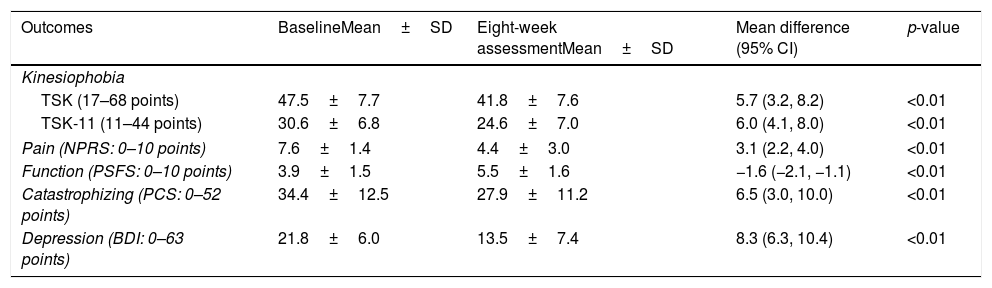
The results of the reliability and criterion and construct validity analyses, and their classification are provided in Table 2. No ceiling and floor effects were detected with no participant reaching the minimum or maximum score. In the validity analysis, the criterion validity between TSK and TSK-11 was confirmed based on a correlation higher than 0.70. For construct validity, only one of the previously defined hypotheses was confirmed (a positive and moderate correlation between TSK-11 and BDI). The results of the interpretability of change scores are presented in Table 3. There was a statistically significant improvement for all outcome measures after the exercise-based intervention (p<0.05).
Reliability and criterion and construct validity of the TSK-11.
| Properties | Values | Classification |
|---|---|---|
| Reliability | ||
| Internal consistency (n=130) | ||
| Cronbach's alpha (alpha if item deleted) | 0.77 (0.74–0.77) | Adequate |
| Reliability (n=54) | ||
| Intraclass correlation coefficient2,1 (ICC2,1, 95% CI) | 0.85 (0.75, 0.90) | Substantial |
| Measurement error (n=54) | ||
| Standard error of measurement (points, %) | 2.65 (7.81) | Good |
| Minimal detectable change (points)a | 6.16 | NC |
| Criterion validity (n=130) | ||
| Tampa Scale for Kinesiophobia (r, p) | 0.84 (<0.01) | Good |
| Construct validity (n=130) | ||
| Numerical Pain Rating Scale (r, p) | 0.25 (<0.01) | Weak |
| Patient-Specific Functional Scale (r, p) | 0.11 (0.23) | – |
| Pain Catastrophizing Scale (r, p) | 0.55 (<0.01) | Moderate |
| Beck Depression Inventory (r, p) | 0.39 (<0.01) | Moderate |
CI, confidence interval; NC, not classified; –, no significant correlation.
Change in scores from pre to post 8-week intervention (n=51).
| Outcomes | BaselineMean±SD | Eight-week assessmentMean±SD | Mean difference (95% CI) | p-value |
|---|---|---|---|---|
| Kinesiophobia | ||||
| TSK (17–68 points) | 47.5±7.7 | 41.8±7.6 | 5.7 (3.2, 8.2) | <0.01 |
| TSK-11 (11–44 points) | 30.6±6.8 | 24.6±7.0 | 6.0 (4.1, 8.0) | <0.01 |
| Pain (NPRS: 0–10 points) | 7.6±1.4 | 4.4±3.0 | 3.1 (2.2, 4.0) | <0.01 |
| Function (PSFS: 0–10 points) | 3.9±1.5 | 5.5±1.6 | −1.6 (−2.1, −1.1) | <0.01 |
| Catastrophizing (PCS: 0–52 points) | 34.4±12.5 | 27.9±11.2 | 6.5 (3.0, 10.0) | <0.01 |
| Depression (BDI: 0–63 points) | 21.8±6.0 | 13.5±7.4 | 8.3 (6.3, 10.4) | <0.01 |
SD, standard deviation; CI, confidence interval.
Higher scores in the Tampa Scale for Kinesiophobia (TSK), Tampa Scale for Kinesiophobia-11 (TSK-11), Numerical Pain Rating Scale (NPRS), Pain Catastrophizing Scale (PCS), and Beck Depression Inventory (BDI) indicate a worse condition, and higher scores in the Patient-Specific Functional Scale (PSFS) indicate better function.
The aim of this study was to analyze the reliability, interpretability, and criterion and construct validity of the TSK-11 in patients with fibromyalgia. The results showed that the Brazilian-Portuguese version of the TSK-11 has adequate internal consistency, substantial reliability, and good measurement error. For validity, the hypotheses confirmed were positive and good correlation with the TSK and positive and moderate correlation with the BDI.
In the baseline assessment, the participants presented with high pain intensity, moderate depression, and a high degree of kinesiophobia and pain catastrophizing. These characteristics are consistent with previous reports of patients with fibromyalgia, i.e., that patients with higher levels of kinesiophobia also report higher levels of pain and depression.1 Other studies in different languages that analyzed the measurement properties of the TSK-11 in patients with chronic pain also found similar results, such as adequate internal consistency, substantial reliability, and good measurement error.9,12–14 Therefore, the Brazilian-Portuguese version of the TSK-11 seems reliable and applicable in the clinical and research settings because it has similar results for these measurement properties as other versions which are already tested and widely used.
The influence of psychological factors is already well described in patients with chronic musculoskeletal pain.35,36 The choice of instruments used in this study to analyze construct validity was based on the fear-avoidance model2 and in agreement with other studies.13,14,17 The TSK-11 was associated with catastrophizing, depression, and pain, as in other studies.13,14 The only instrument that showed no correlation with the TSK-11 was the PSFS, which assesses disability in specific activities indicated by the patient. The PSFS is more specific than other disability scales,18 which may explain this finding. Studies13,14 usually measure functional capacity using general disability assessment instruments. However, only 40% of the hypotheses were confirmed for validity. Given that patients with fibromyalgia appear to have different results from other patients with chronic pain in physical and psychological constructs,37 our hypotheses may have been overestimated. Other point that should be highlighted is that none of the instruments used to assess construct validity evaluates kinesiophobia directly, the chosen instruments evaluate related constructs.
One of the strengths of this study is that the instruments used as comparators to assess the criterion validity and construct validity have already been validated for Brazilian-Portuguese and showed adequate measurement properties. As recommended by the guidelines, to determine whether the results are reliable, it is essential to provide information about the measurement properties of the instruments used to analyze the correlations between the constructs.38 Another important point is that all clinical outcomes (kinesiophobia, pain, function, catastrophizing, and depression) showed improvement after intervention. An improvement of pain and function was expected, as the intervention was designed according to the guidelines.39,40 However, our data showed that kinesiophobia also improved, even after an intervention not designed specifically to change fear. A limitation of the present study is that responsiveness was not assessed. Further studies are needed that include treatments targeting kinesiophobia in patients with fibromyalgia to evaluate the responsiveness of the Brazilian-Portuguese version of the TSK-11.
ConclusionThe TSK-11 may be considered adequate and reliable for use in future research and in the assessment of patients with fibromyalgia in clinical practice. However, further studies are necessary to assess its responsiveness.
Conflicts of interestThe authors declare no conflicts of interest.
This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001. The funder had no role in the study design, in the collection, analysis, and interpretation of data, in the writing of the report, and in the decision to submit the article for publication.



