





Interprofessional education of healthcare providers is necessary to foster collaborative practice and improve patient outcomes.
ObjectiveTo examine the effectiveness of the single-session interprofessional education in improving interprofessional attitudes, increasing knowledge of healthcare professions, and improving perceived-readiness for working interprofessionally and with older adults in students in occupational therapy, physical therapy, and physician assistant graduate programs.
MethodsWe used a prospective, pre–post cohort design. Fall risk evaluation for older adults was selected as the topic of the 4-hour interprofessional education session. Graduate students from three professional programs including occupational therapy (n=20), physical therapy (n=26), and physician assistant studies (n=35) participated in the study, and 17 older adults aged 65 years or older volunteered for the session. Our primary outcome measure was the Interprofessional Attitudes Scale measuring interprofessional attitudes, and our secondary outcome measure was the study-specific questionnaire measuring the direct effect of our interprofessional education session.
ResultsGraduate students showed significant improvements in the subscale of teamwork, roles, and responsibilities in the Interprofessional Attitudes Scale. Students also showed significant improvements in “understanding of other professions,” “perceived-readiness to work interprofessionally,” and “perceived-readiness to work with older adults” in the study-specific questionnaire. Ceiling effects were observed in most of the subscales in the Interprofessional Attitudes Scale.
ConclusionThis study demonstrates that a single 4-hour interprofessional education session can improve interprofessional attitudes, knowledge of other professions, and perceived-readiness of health science graduate students to work interprofessionally and to work with older adults.
Health-related academic programs educate their students to become competent healthcare professionals in their respective profession upon graduation. Once entering the healthcare field, these professionals are expected to work collaboratively to provide optimal patient care. Studies have shown introduction of interprofessional education (IPE) during academic preparation can improve attitudes and perceptions of other healthcare professions.1,2 The World Health Organization initiated discussions of IPE to increase collaboration amongst healthcare providers and improve patient outcomes.3 Furthermore, the continued increase in medical costs and the rising number of older adults have resulted in the need for healthcare providers to be more effective and efficient in their services while offering quality at a lower cost. These actions naturally support the need for interprofessional collaborative care and IPE, and, as a result, IPE standards have been implemented into healthcare professions’ academic requirements over the years.4–9 According to the multiple systematic reviews, the positive impacts of interprofessional collaboration on clinical outcomes include faster functional recovery, fewer complications, higher quality of life, shorter hospital stay, fewer hospitalization, less morbidity, and higher patient satisfaction compared to those of standard care.10–12 In addition, positive impacts on health human resources include higher provider satisfaction and workplace quality, and lower outpatient costs.13 Despite these positive impacts, adoption of interprofessional collaboration in practice has been slower than hoped.8
The number of injured persons from unintentional falls almost triples for persons 65 and older.14 The American Geriatrics Society and British Geriatric Society have fall prevention guidelines for healthcare professionals with the recommendation that all older adults be screened and assessed for falls.15 Various healthcare professions address fall prevention and, therefore, it is imperative for interprofessional collaboration to occur when working with older adults during this process. Healthcare professionals, specifically physicians, physician assistants, and nurse practitioners, need to ensure that correct referrals for therapy services are being made to appropriate healthcare professionals. The increase in the number of physician assistants16 providing medical services to older adults increases the need to educate these professionals on proper referrals to occupational therapy and/or physical therapy services. One way to improve the understanding of occupational therapy and physical therapy and appropriate referrals is to educate physician assistant students when they are in their academic preparation. Conversely, therapists often refer patients to specialist care or back to primary care practitioners to address medical concerns. Therefore, all healthcare providers must understand each other's roles, responsibilities, and scope of practice, and how these professions can improve communication and work collaboratively in providing healthcare services.17 Although there are a few studies where the effectiveness of IPE sessions was examined with students from physician assistant, physical therapy, or occupational therapy graduate programs,18–21 none of these studies were aligned with core competencies for interprofessional collaborative practice.8 Furthermore, to our knowledge, there is no study where the effectiveness of an IPE session was examined among graduate students from physician assistant, physical therapy, and occupational therapy programs in terms of fall prevention.
The research purposes of our study were to determine the effectiveness of the IPE session on fall risk evaluations for older adults in (1) improving interprofessional attitudes, (2) increasing knowledge of own and other professions, and (3) improving perceived-readiness for working interprofessionally as well as working with older adults in students in occupational therapy, physical therapy, and physician assistant graduate programs.
MethodsStudy designA prospective, pre–post cohort design was used for this study with the IPE occurring between Pretest and Posttest (see Fig. 1). After agreeing to participate in the study, graduate students completed the outcome measures prior to their IPE session (Pretest), received the IPE session, and again completed the outcome measures after their IPE session (Posttest).
Participants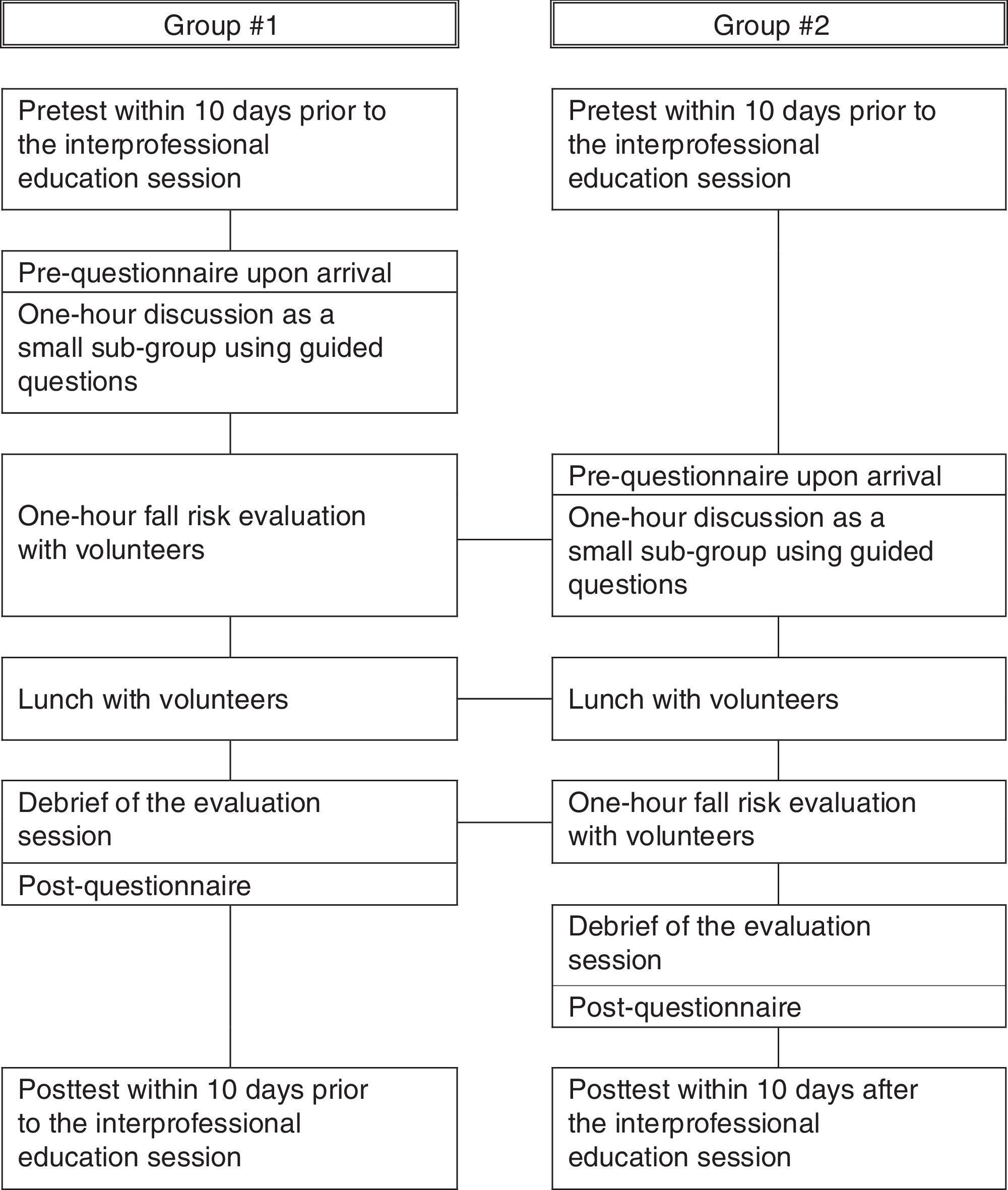
Convenience sampling without sample size calculation or power analysis was used to recruit participants for this study. As a result, 20 students in the Master of Science in Occupational Therapy (OT) program, 26 students in the Doctor of Physical Therapy (PT) program, and 35 students in the Master of Science in Physician Assistant (PA) program in College of Allied Health Sciences at East Carolina University, Greenville NC participated in this study as a part of the requirements in their respective graduate courses in the summer of 2016. The participation in this study required students’ informed consent, completion of Pretest and Posttest, and participation in the IPE session, and all students who participated in the IPE session completed Pretest and Posttest without missing data. OT graduate students were in their third semester out of seven semesters, PT graduate students were in their fourth semester out of nine semesters, and PA graduate students were in their third semester out of seven semesters in the program. The faculty members of OT, PT, and PA departments voluntarily planned and implemented this IPE session, instead of being required by the College, to provide opportunities for IPE and working with older adults to their respective students.
ProcedureFall risk evaluations for older adults were selected for the IPE session because of older adults’ interest in their risk for falls and their accessibility through our community. This study was the first time that students from those three departments participated in the IPE session. Six meetings with each lasting 1.5–2hours, among four core faculty members (two from OT, one from PT, and one from PA), occurred to plan the IPE session, starting 6 months prior to the session. During the meetings, faculty generated nine educational objectives in relation to four interprofessional collaborative practice competency domains8 and discussed logistics of the session (see Table 1). The logistics included (1) identifying proper semester, date, and time for the session, (2) identifying the location of the session, (3) identifying volunteer (senior community members) recruitment strategies, (4) identifying the appropriate assessment tools for fall risk evaluation, (5) creating the fall risk assessments training plan for students, and (6) creating the schedules and directions for the session for a smooth and optimal session flow.
Educational objectives, and interprofessional collaborative practice competency domains and core competencies.
| Competency domaina | Educational objective | Core competencya |
|---|---|---|
| Values/ethics for interprofessional practice | Place the interests of clients at the center of the interprofessional experience. | (VE1) Place the interests of patients and populations at the center of the interprofessional health care delivery. |
| Respect other professions’ cultures, values, roles/responsibilities, and expertise. | (VE4) Respect the unique cultures, values, roles/responsibilities, and expertise of other health professions | |
| Work in cooperation with others (clients and other professionals). | (VE5) Work in cooperation with those who receive care, those who provide care, and other who contribute to or support the delivery of prevention and health services. | |
| Roles/responsibilities | Recognize one's limitations in skills, knowledge, and abilities. | (RR2) Recognize one's limitations in skills, knowledge, and abilities |
| Clearly communicate one's roles and responsibilities to others (clients and other professionals). | (RR1) Clearly communicate one's roles and responsibilities to patients, families, and other professionals. | |
| Interprofessional communication | Communicate with others (clients and other professionals) in a form that is understandable (e.g. avoiding jargons). | (CC2) Organize and communicate information with patients, families, and healthcare team members in a form that is understandable, avoiding discipline-specific terminology when possible. |
| Express one's knowledge and opinions to other professionals with confidence, clarity, and respect. | (CC3) Express one's knowledge and opinions to team members involved in patient care with confidence, clarity, and respect, working to ensure common understanding of information and treatment and care decisions. | |
| Teams and teamwork | Apply leadership practices for collaborative practice and interprofessional effectiveness. | (TT5) Apply leadership practices that support collaborative practice and team effectiveness |
| Perform effectively on teams. | (TT11) Perform effectively on teams and in different team roles in a variety of settings. | |
Note: VE, values/ethics for interprofessional practice; RR, roles/responsibilities; CC, interprofessional communication; TT, teams and teamwork.
Adapted from “Core Competencies for Interprofessional Collaborative Practice: Report of an Expert Panel,” by Interprofessional Education Collaborative Expert Panel, 2011. Copyright 2011 by the American Association of Colleges of Nursing, American Association of Colleges of Osteopathic Medicine, American Association of Colleges of Pharmacy, American Dental Education Association, Association of American Medical Colleges, and Association of Schools of Public Health.
Following the approval from the Institutional Review Board at East Carolina University, Greenville, NC, USA (UMCIRB 16-000869), one OT faculty member who was not involved in course instruction of this session visited each profession's class 10 days prior to the IPE session to prevent any bias of measurement. During the visit, the faculty member explained the study to the students, obtained the informed consent, and administered the Pretest using Interprofessional Attitudes Scale (IPAS). A code number was assigned to each student, and all other faculty were blind to the code assignment to ensure student responses did not affect their academic grading and to prevent any source of measurement bias. Posttest using IPAS was administered by the same faculty member within 10 days of the completion of the IPE session. IPAS was self-reported, and no other student information than the code number was written on the assessment sheets.
Students were trained by their respective faculty member(s) on the assessment tools for fall risk evaluation between Pretest and the IPE session. The fall risk assessment tools selected for OT included Saint Louis University Mental Status,22 Short Falls Efficacy Scale – International,23 and Snellen Chart24; those for PT included Dynamic Gait Index25 and Modified Clinical Test of Sensory Integration and Balance26; and for PA was the Simple Geriatric Screen.27 Training sessions for each respective profession lasted for an hour, and students were required to review their assigned assessment tools prior to the interprofessional session to demonstrate competency.
Students were divided into two similar group sizes and exposed to the same experiential components over 4hours, however, in a different order (see Fig. 1). Upon the students’ arrival at a local church where the IPE session occurred, students completed the Pre-questionnaire (study-specific questionnaire) followed by 1-hour discussion time. During this discussion time, students as a small sub-group (maximum of five students consisting of one or two OT students, one or two PT students, and two PA students) discussed about each profession's curriculum, degree requirements, scope of practice, practice settings, and assessment tools they were going to use for the fall risk evaluation. The same small sub-groups then went to an assigned room to administer the fall risk evaluation for their volunteers. The volunteers were a total of 17 older adults aged 65 years or older in the community and were recruited through personal connections and flyer advertisements. No information on volunteers’ demographics or medical history was collected for this study. Each small sub-group conducted the fall risk evaluation with one volunteer for 1 hour and was encouraged to spend no more than 20minutes for each profession to complete the evaluation. Students were also encouraged to observe and assist with other professions’ evaluations. After the fall risk evaluations, small sub-groups of students and volunteers gathered and had lunch together, and asked any questions they had from the evaluation process as well as the results of the evaluations. After this lunch/debriefing session, students completed Post-questionnaire (study-specific questionnaire) and were dismissed.
MeasuresDescriptive information on gender and age ranges was collected from the students. Our primary outcome measure was the IPAS developed to be consistent with four core competencies of the 2011 Core Competencies for Interprofessional Collaborative Practice report.8 IPAS measures interprofessional attitudes using 27 items in five sub-scales including teamwork, roles, and responsibilities, patient-centeredness, interprofessional biases, diversity and ethics, and community-centeredness. The 14 items in the subscales of teamwork, roles, and responsibilities, and patient-centeredness were adapted from the extended Readiness for Interprofessional Learning Scale28 with minor wording modifications to make them more relevant to students, and the 13 items in the subscales of interprofessional biases, diversity and ethics, and community centeredness were newly added. The IPAS uses a five-level ordinal scale from 1 (strongly disagree) to 5 (strongly agree) and yields mean scores for sub-scales. It was validated through exploratory factor analysis and confirmatory factor analysis.29
Our secondary outcome measure was the study-specific questionnaire that we created to measure the direct effects of our IPE experience. The questionnaire contains 15 items measuring understanding of role/scope of practice and practice settings for each profession including their own, readiness to work interprofessionally in terms of their understanding, perceived-performance, and confidence, and readiness to work with older adults in terms of their understanding, perceived-performance, and confidence in communicating with older adults and administering fall risk assessments with this population. The questionnaire uses a five-level ordinal scale from 1 (strongly disagree) to 5 (strongly agree) and yields mean scores for five different categories including understanding of own profession, understanding of the two other professions, perceived-readiness to work interprofessionally, and perceived-readiness to work with older adults.
Data analysisStatistical analyses were performed with the IBM SPSS 24 (IBM Corp., Armonk, NY) and Microsoft Excel (Microsoft Corporation, Redmond, WA) for effect size calculation. Descriptive statistics were used to document the demographics of the students. Due to the assumption violation, Kruskal–Wallis tests were used to compare the differences in changes among OT, PT, and PA graduate students for each sub-scale of IPAS and each category of the study-specific questionnaire, followed by Mann–Whitney tests with Bonferroni corrections as appropriate. For the difference in changes in understanding of the two other professions, Mann–Whitney tests were used. Lastly, Wilcoxon signed-rank tests were used to analyze the changes in each sub-scale of IPAS and each category of the study-specific questionnaire for students in each individual professional program. For all Kruskal–Wallis tests, an alpha level of .05 was used to determine statistical significance. To determine the degrees of differences found from Mann–Whitney tests and/or Wilcoxon signed-rank tests, effect sizes r were calculated. A r value between 0 and 0.09 is considered as negligible effect, between 0.10 and 0.23 as small effect, between 0.24 and 0.36 as medium effect, between 0.37 and 0.70 as large effect, and a r value of 0.71 or greater as very large effect.30
ResultsMost students were female (n=64, 78%) and belonged to age groups of 21–26 years (n=69, 85%) (see Table 2). In the IPAS subscale of teamwork, roles, and responsibilities, we found significant improvements at Posttest compared to Pretest for all three programs (p=.02, p=.03, and p=.03 for OT, PT, and PA, respectively). We also found significant improvement in the IPAS subscale of patient-centeredness at Posttest compared Pretest for OT students (p=.04). Ceiling effects were observed in all IPAS subscales, except for the subscale of interprofessional biases (see Table 3). In the study-specific questionnaire, we found significant improvements at Post-questionnaire compared to Pre-questionnaire in all categories (p<.001), except for the category of “understanding of own profession in general.” Specifically, the degrees of these significant improvements were very large (r=0.74–0.86). We found significant differences in improvements between the PT and PA students in the category of “understanding of OT profession in general” (p=.03, r=0.30) and among the three programs in the category of “perceived-readiness to work with older adults” (p=.003). According to the post hoc tests for the category of “perceived-readiness to work with older adults,” we found significantly different improvements between OT and PT students (p=.002) and between PT and PA students (p=.004) with large effect sizes r (0.46 and 0.37, respectively). PT students showed significantly smaller improvements compared to OT and PA students (see Table 4).
Demographics of students.
| Gender, n (%) | Age groups in years, n (%) | ||||
|---|---|---|---|---|---|
| Male | Female | 21–23 | 24–26 | 27 and over | |
| OT | 1 (5) | 19 (95) | 9 (45) | 8 (40) | 3 (15) |
| PT | 6 (23.1) | 20 (76.9) | 16 (61.5) | 9 (34.6) | 1 (3.8) |
| PA | 10 (28.6) | 25 (71.4) | 9 (25.7) | 18 (51.4) | 8 (22.9) |
Note: OT, occupational therapy; PT, physical therapy; PA, physician assistant.
Results of Interprofessional Attitudes Scale between times and among programs.
| Subscales | Profession | Pre Mdn (IQR) | Post Mdn (IQR) | Program | Time | ES r |
|---|---|---|---|---|---|---|
| Teamwork, roles, and responsibilities | OT (n=20) | 4.44 (0.78) | 4.83 (0.33) | H=1.18p=.55 | z=−2.35p=.02 | 0.53 |
| PT (n=26) | 4.44 (0.81) | 4.56 (0.69) | z=−2.16p=.03 | 0.42 | ||
| PA (n=35) | 4.56 (0.61) | 4.78 (0.44) | z=−2.13p=.03 | 0.36 | ||
| Patient-centeredness | OT (n=20) | 5.00 (0.15) | 5.00 (0) | H=3.19p=.20 | z=−2.07p=.04 | 0.46 |
| PT (n=26) | 5.00 (0.25) | 5.00 (0.05) | z=−1.30p=.19 | |||
| PA (n=35) | 5.00 (0.60) | 5.00 (0) | z=−0.14p=.89 | |||
| Interprofessional biases | OT (n=20) | 3.83 (0.92) | 3.33 (1.58) | H=0.48p=.79 | z=−0.60p=.55 | |
| PT (n=26) | 3.67 (0.67) | 3.67 (1.00) | z=−0.71p=.48 | |||
| PA (n=33) | 4.00 (1.17) | 3.67 (0.67) | z=−0.03p=.98 | |||
| Diversity and ethics | OT (n=20) | 5.00 (0) | 5.00 (0) | H=0.24p=.89 | z=−0.74p=.46 | |
| PT (n=26) | 5.00 (0.06) | 5.00 (0.06) | z=0p=1.00 | |||
| PA (n=33) | 5.00 (0) | 5.00 (0) | z=−0.78p=.44 | |||
| Community-centeredness | OT (n=20) | 4.80 (1.00) | 5.00 (0.55) | H=0.60p=.74 | z=−1.27p=.20 | |
| PT (n=26) | 4.20 (1.00) | 4.20 (1.00) | z=−1.25p=.21 | |||
| PA (n=33) | 4.60 (0.70) | 4.80 (1.00) | z=−0.21p=.83 | |||
Note: OT, occupational therapy; PT, physical therapy; PA, physician assistant; ES, effect size.
Results of the study-specific questionnaire between times and among programs.
| Categories | Profession | Pre Mdn (IQR) | Post Mdn (IQR) | Program | Time | ES r† |
|---|---|---|---|---|---|---|
| Understanding of own profession in general | OT (n=20) | 5.00 (0) | 5.00 (0) | H=0.61p=.74 | z=−1.00p=.32 | |
| PT (n=26) | 5.00 (0) | 5.00 (0) | z=−0.45p=.66 | |||
| PA (n=35) | 5.00 (0) | 5.00 (0) | z=−1.00p=.32 | |||
| Understanding of OT profession in general | PT (n=26) | 3.50 (1.00) | 4.25 (0.43) | z=−2.16p=.03 | z=−4.16p<.001 | 0.82 |
| PA (n=35) | 3.50 (1.00) | 4.50 (1.00) | z=−5.04p<.001 | 0.85 | ||
| Understanding of PT profession in general | OT (n=20) | 4.00 (0.50) | 4.50 (1.00) | z=−0.65p=.517 | z=−3.31p=.001 | 0.74 |
| PA (n=35) | 4.00 (0.50) | 5.00 (1.00) | z=−4.78p<.001 | 0.81 | ||
| Understanding of PA profession in general | OT (n=20) | 3.50 (1.50) | 4.50 (0.88) | z=−0.33p=.74 | z=−3.50p<.001 | 0.78 |
| PT (n=26) | 3.00 (1.13) | 4.00 (0.50) | z=−4.33p<.001 | 0.85 | ||
| Perceived-readiness to work interprofessionally | OT (n=20) | 4.00 (0.58) | 5.00 (0.92) | H=3.78p=.15 | z=−3.55p<.001 | 0.79 |
| PT (n=26) | 4.00 (0.67) | 4.67 (1.00) | z=−3.97p<.001 | 0.78 | ||
| PA (n=33) | 4.00 (0.67) | 5.00 (0.33) | z=−4.51p<.001 | 0.78 | ||
| Perceived-readiness to work with older adults | OT (n=20)a | 3.67 (0.83) | 4.75 (0.67) | H=11.78p=.003 | z=−3.84p<.001 | 0.86 |
| PT (n=26)a,b | 4.00 (0.67) | 4.83 (1.00) | z=−4.04p<.001 | 0.79 | ||
| PA (n=35)b | 3.67 (1.00) | 4.50 (0.83) | z=−4.86p<.001 | 0.82 | ||
Note: OT, occupational therapy; PT, physical therapy; PA, physician assistant; ES, effect size.
a,b,cPrograms that share a letter are significantly different from each other in their improvements based on the post hoc tests.
In our study, we examined the effect of a one-session IPE on the interprofessional attitudes and perceived-readiness to work interprofessionally and with older adults. The single-session model was selected because it was more realistic in our educational setting which has not yet implemented formal institution-wide interprofessional coursework. Also, this model was appropriate for the specific standards that our professional programs should have met. Abu-Rish et al.31 identified barriers of IPE implementation reported in 83 published studies, and these included scheduling, learner-level compatibility, preparation time required, outcomes measurement, and administrative support.31 Although it required six meetings among the involved faculty members to prepare the session, faculty's and departments’ flexibility in scheduling, matching educational levels in the programs, pre-existing relationship among the faculty members, geological factors including the close proximity among the faculty offices and the short distance to the session location, and the support from the departments and administration were the supporting factors for the session.
Not surprisingly, we found significant improvements in interprofessional attitudes only in the subscale of teamwork, roles, and responsibilities for all three program students. During the IPE session, students were given time to interact with other professional students using the guided questions. Also, many of the items in the IPAS subscale of teamwork, roles, and responsibilities were related to “learning” or “shared learning” that students may have more easily related to their interactions with other students and perceived as the main objective of our session. Although some of the other IPAS subscales, such as patient-centeredness and diversity and ethics, were also reflected in our session's educational objectives, these areas were considered more as “foundational values” in the programs and professions and, hence, we did not expect to see big improvements for all programs through this one-time session. Therefore, interprofessional attitudes toward teamwork, roles, and responsibilities may have been the most closely aligned outcome area for our IPE session or even any isolated IPE session.
According to our study-specific questionnaire, students in three programs reported increased knowledge of other professions and increased perceived-readiness to work interprofessionally and work with older adults. In addition, the degrees of these improvements were very large. Students in three programs showed very high understanding of their own professions at Pretest, meaning that there was only minimal potential for change. The large-degree increase in knowledge on other professions were unexpected, considering that they had only 2hours to discuss with each other and approximately 40minutes to observe the other professions’ fall risk evaluations. However, the smaller improvements in knowledge on OT by PT students compared to PA students can be possibly due to PT students’ easier access to OT practice during shadowing or fieldwork.
It was also surprising that students’ perceptions on their readiness to work interprofessionally and with older adults improved to a very large degree despite their indirect collaborations with each other during the evaluation sessions and the short amount of time for interactions with older adults. Although students were encouraged to “actively observe and assist” the other professions’ respective assessments, faculty observed that three professions’ fall risk assessments completed by students from three professional programs appeared paralleled rather than interactive. Our findings are consistent with results from five studies where students showed improved interprofessional attitudes, interprofessional perceptions, and/or understanding of other professions after participating in 2.5–4hours of IPE sessions.32
There are several practical implications for IPE among healthcare professional students that we learned from our study. First, although it is challenging to organize and implement a successful IPE session among multiple professions, it is possible with planning and support from stakeholders. Based on our experience, it will be ideal to begin the planning at least 6 months prior to the session. Secondly, our study showed that even a single IPE session with older adults can provide a valuable opportunity to healthcare professional students to improve their interprofessional attitudes and readiness to work with other professions for older adults. Considering students’ improvement in these areas, and the common issue of falls in older adults requiring interprofessional collaboration, the time and effort to organize and implement the session is worthwhile. Having an opportunity to observe and interact with other professional students while working with a real community dwelling elders, compared to a written case study, may enhance student engagement and the effectiveness of the IPE session. Lastly, an IPE session with specific educational objectives, such as fall risk evaluation, may help students understand expectations of the IPE and focus on working together to achieve a common goal. Our IPE session specifically focused on completing a fall risk evaluation, and we believe this allowed students to easily understand the goals of the IPE that were to effectively communicate and collaborate with other professions for optimal patient outcomes within a specific context.
There were several limitations in our study. First, it was not feasible to have a control group in our study because our IPE session was the part of the coursework in each program and it was not possible to schedule several different sessions for three professional programs. Secondly, although students were in the third or fourth semesters of their professional programs, their knowledge level of their own professions as well as other professions may have not been equivalent because of the differences in curriculum. For example, PT students had already completed their first clinical experience during their previous semester, whereas OT and PA students had not completed any clinical experiences yet. However, these differences did not bias our results because we measured the changes in the outcomes, instead of measuring them at a single point in time. Thirdly, Posttest using the IPAS was conducted within 10 days of, rather than right after, the IPE session. Although the purpose of this delayed Posttest was to allow students for time to reflect on their experience, their responses on the Posttest may have been biased by other factors, such as conversation among their classmates. In addition, the long-term effect of the IPE session for each professional program was not examined due to students’ receiving differing class contents after the session. Lastly, although the items of our study-specific questionnaire were closely aligned with the educational purposes of our session, its psychometric properties were not tested prior to our experience; therefore, readers need to keep this in mind when interpreting the results of the study-specific questionnaire.
ConclusionThis study demonstrates the feasibility of a single 4-hour IPE session among OT, PT, and PA graduate students within institutions without a formal interprofessional curriculum. However, careful planning and coordination among the involved departments prior to the session are necessary to have clear educational and research objectives with detailed plans to achieve those objectives. This study shows that a single 4-hour IPE session among OT, PT, and PA graduate students can improve their interprofessional attitudes in teamwork, roles, and responsibilities, knowledge of other professions, and perceived-readiness to work interprofessionally and work with older adults. Future studies should consider including a control group by scheduling a delayed IPE session, having an IPE session at the end of the semester to minimize any factors affecting the results of Posttest and to allow follow-up tests with fewer confounding factors, and using the items of the well-established assessments as a guide to develop the educational objectives.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank Chia-Cheng Lin for his assistance choosing assessments for supervising students and Black Jack Free Will Baptist Church, Greenville, NC for providing physical space and assistance for the interprofessional education session.



