





This is a cross-sectional study.
SettingUniversity research laboratory.
ParticipantsFifteen healthy adults (mean age: 27.47 years) volunteered for this study.
InterventionThe individuals performed standard bridge exercise and modified bridge exercises with right leg-lift (single-leg-lift bridge exercise, single-leg-lift bridge exercise on an unstable surface, and single-leg-lift hip abduction bridge exercise).
Main outcome measuresDuring the bridge exercises, electromyography of the rectus abdominis, internal oblique, erector spinae, and multifidus muscles was recorded using a wireless surface electromyography system. Two-way repeated-measures analysis of variance (exercise by side) with post hoc pairwise comparisons using Bonferroni correction was used to compare the electromyography data collected from each muscle.
ResultsBilateral internal oblique muscle activities showed significantly greater during single-leg-lift bridge exercise (95% confidence interval: right internal oblique=−8.99 to −1.08, left internal oblique=−6.84 to −0.10), single-leg-lift bridge exercise on an unstable surface (95% confidence interval: right internal oblique=−7.32 to −1.78, left internal oblique=−5.34 to −0.99), and single-leg-lift hip abduction bridge exercise (95% confidence interval: right internal oblique=−17.13 to −0.89, left internal oblique=−8.56 to −0.60) compared with standard bridge exercise. Bilateral rectus abdominis showed greater electromyography activity during single-leg-lift bridge exercise on an unstable surface (95% confidence interval: right rectus abdominis=−9.33 to −1.13, left rectus abdominis=−4.80 to −0.64) and single-leg-lift hip abduction bridge exercise (95% confidence interval: right rectus abdominis=−14.12 to −1.84, left rectus abdominis=−6.68 to −0.16) compared with standard bridge exercise. In addition, the right rectus abdominis muscle activity was greater during single-leg-lift hip abduction bridge exercise compared with single-leg-lift bridge exercise on an unstable surface (95% confidence interval=−7.51 to −0.89). For erector spinae, muscle activity was greater in right side compared with left side during all exercises (95% confidence interval: standard bridge exercise=0.19–4.53, single-leg-lift bridge exercise=0.24–10.49, single-leg-lift bridge exercise on an unstable surface=0.74–8.55, single-leg-lift hip abduction bridge exercise=0.47–11.43). There was no significant interaction and main effect for multifidus.
ConclusionsAdding hip abduction and unstable conditions to bridge exercises may be useful strategy to facilitate the co-activation of trunk muscles.
Trunk stabilization exercises are an important strategy in rehabilitation. Trunk stabilization exercises seem to increase activation of the trunk stability muscles such as the internal oblique (IO) and lumbar multifidus (MF) muscles, and these muscles are essential for precise functioning of the lumbopelvic complex.1,2 Also, trunk stabilization exercises retrain proper activation and coordination of trunk muscle through improved motor control,3,4 which reduces compensatory lumbo-pelvic motion.5 All these aspects contribute to increased spinal stability.3–5
Bridge exercises are often used to strengthen the trunk stability muscles.6 A bridge exercise is a closed-chain weight-bearing exercise that increases activation of the trunk stability muscles to maintain the bridge posture and resist gravitational toque.7,8 Bridge exercises are easy and convenient, activate the trunk stability muscles, and are commonly used in clinical settings.
To improve the effects of bridge exercises, modified bridge exercises have been proposed.8–11 García-Vaquero et al.8 have reported that when bridge exercises were performed with single-leg support, rotational torque in the trunk increased the activation of the trunk muscles to maintain neutral lumbar position.8 Recent research has introduced bridge exercises with the feet on an unstable surface to add dynamic stabilization effort.9,10 Park et al.11 have showed that the integration of limb movement during bridge exercises is more effective for facilitating the activity of the IO and MF muscles than bridge exercises alone, with greater effect from bilateral hip movement than from unilateral movement.11 Limb movements and hip abduction and adduction contribute to the transmission of force to the lumbar muscles via the anterior superior iliac spine portion of the pelvis.12
Studies have examined how bridge exercises on an unstable surface and with limb movement increase trunk muscle activity.8–10 Movement of the lower extremities during bridge exercises has a significant effect on the trunk muscles.11 However, no study has assessed whether these movements are more effective to increase trunk muscle activities than standard modified bridge exercises, such as bridge exercises on an unstable surface. We hypothesized that single-leg support with hip abduction would increase trunk muscle activity. Therefore, this study compared the effects of traditional bridge exercise and modified bridge exercises (e.g., bridge exercises with hip abduction or on an unstable surface) on trunk muscle activity.
MethodsDesignA cross-sectional design was used to compare the effects of modified bridge exercises (e.g., bridge exercises with hip abduction strategy or on an unstable surface) on trunk muscle activity.
ParticipantsThe study enrolled 15 physically active volunteers (12 males, 3 females; mean age 27.47 [SD: 3.04] years; height 172.40 [SD: 6.77]cm; weight 68.20 [SD: 11.27]kg) after they signed informed consent forms approved by the Institutional Research Review Committee of Inje University, Gimhae, South Korea (approval protocol 2-1040124-AB-N-01-20150423-HR-228). The inclusion criteria were (1) no previous or current neurological or musculoskeletal illnesses that could influence bridge exercises; (2) no limitation in hip joint motion (i.e., greater than 0° of hip extension measured by goniometer) or significant weakness of the lower limb muscles (i.e., greater than grade 3 of hip extensor muscles strength using manual muscle testing); and (3) no history of surgery in the trunk or lumbopelvic region. Individuals were excluded if they were pregnant, participated in elite sports training, or had less than 6 months of weight training experience.
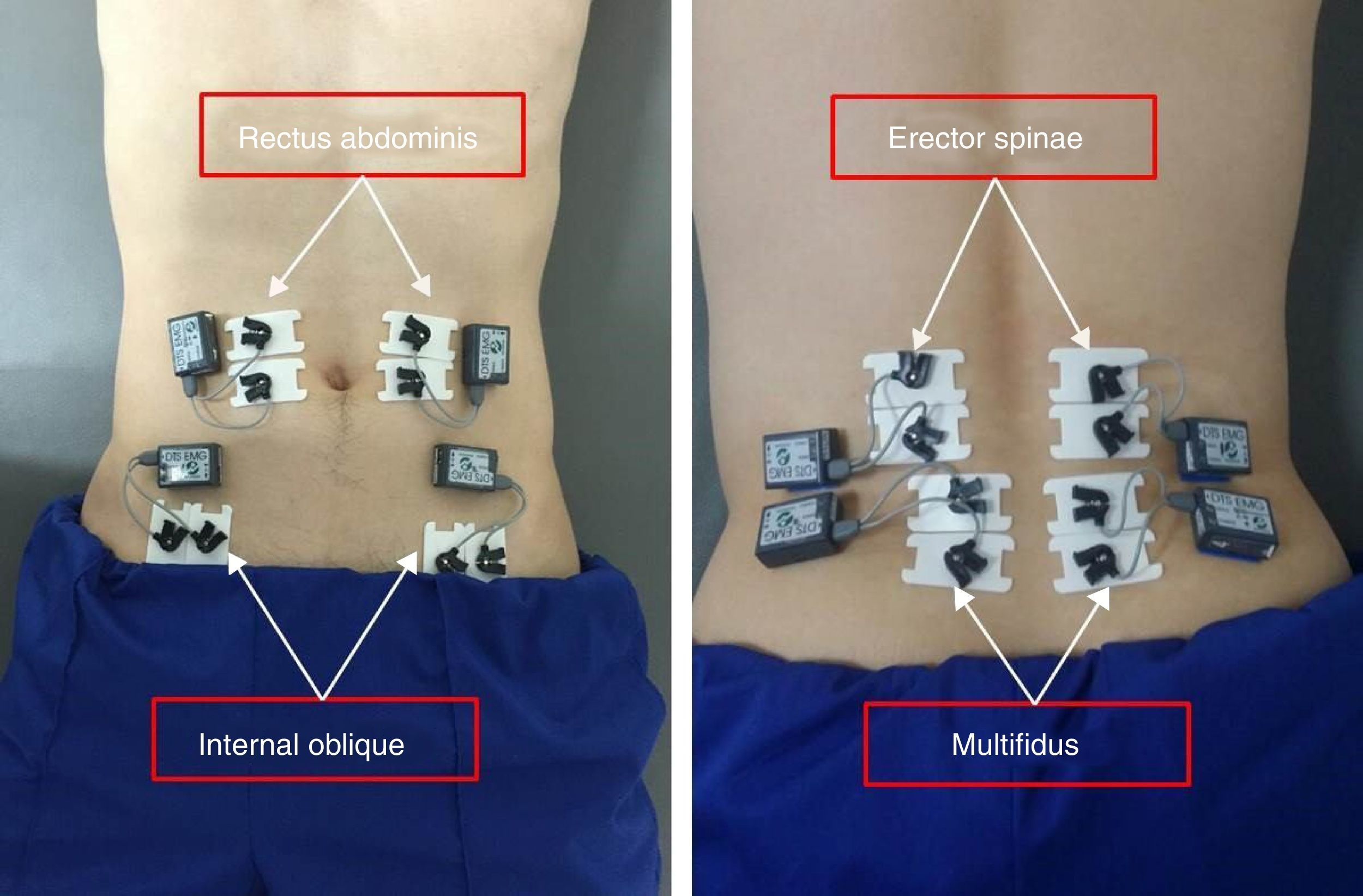
ProceduresElectromyography (EMG) data were recorded and analyzed using the Noraxon TeleMyo 2400T (Noraxon, Scottsdale, AZ, USA). After the skin at the electrode sites was shaved and cleaned with alcohol swabs, surface EMG data were collected from the IO, rectus abdominis [RA], erector spinae [ES], and MF muscles bilaterally. Electrodes for the IO were positioned horizontally 2cm inward and distal to the anterior superior iliac spine12; electrodes for the RA were placed proximally, 3cm lateral to the umbilicus9; electrodes for the ES were attached proximally 3cm lateral to the L3 spinous process12; and electrodes for MF were positioned just laterally from midline of vertebrae, above and below to both posterior superior iliac spines (Fig. 1).9,13
The signals were amplified and band-pass filtered (20–450Hz) before being recorded digitally at 1000samples/s, and then the root mean square (RMS) was calculated. To normalize the EMG signals collected from each muscle, the RMS of 5-s maximal voluntary isometric contraction (MVIC) of the muscles was measured in three trials before the experimental tasks to provide a basis for normalizing the EMG signal amplitude.14,15 Each isometric exercise was performed against manual resistance. Verbal encouragement was given to ensure maximal effort. The maximal activation of the IO was obtained from the same sitting position with the hands placed behind the head, using combined flexion-rotation with the trunk held at a 45° angle and manual resistance applied to the contralateral shoulder.14 The angle of trunk was measured by goniometer, and target bar was placed to maintain target angle during MVIC maneuvers. To generate the maximal isometric activity of the RA, the individual was asked to perform trunk flexion until scapular inferior angle break off floor, against bilateral manual resistance applied to both shoulders, in the straight-knee sitting position, with the hands placed behind the head.15 For the MVIC of the ES and MF, resistance was applied to the posterior aspect of the scapula in the prone position with the legs strapped to the table to prevent them from moving, and the individual was asked to perform trunk extension.14,16 The EMG signals recorded from each muscle during the bridge exercises were calculated as a percentage of the RMS of the MVIC (%MVIC). Three test trials were performed at 3-min intervals. The EMG data were measured for 5s and exclude the first and last seconds at each trial. All EMG data were averaged over three trials for data analysis.
In this study, four types of bridge exercise were performed. Before the measurements, all of the individuals were instructed on each exercise and allowed 5min to practice them, which was sufficient familiarization for each exercise. The details of each exercise are as follows: (1) bridge exercise (BE): the individuals were instructed to adopt a supine position with their arms crossed on their chest and to elevate their pelvis until the hip flexion angle was 0° using goniometer and target bar; (2) single-leg-lift bridge exercise (SLBE): the same posture as for BE was maintained, with the right knee extended; (3) single-leg-lift bridge exercise on an unstable surface (SLBU): the same posture as that for SLBE was maintained with a dynamic air cushion (TOGU, Germany) under the left foot; and (4) single-leg-lift hip abduction bridge exercise(SLHB): the same posture as that for SLBE was maintained with 20° of right hip abduction. To assure a range of 20° in hip abduction during the bridge exercises, target bars were positioned lateral to the right knee joint, and the individuals were asked to keep the lateral area of the knee at the target bar. For the modified bridge exercises, the individuals were told to keep trunk motion to a minimum, while maintaining the spine and pelvis in a neutral position. The individuals were allowed to take a 2-min break between exercises to prevent muscle fatigue in the trunk and lower extremities.17 A 5-min break was allowed after the bridge exercise on an unstable surface because it requires greater muscle activity due to the constant postural and stability changes.18 Each individual was instructed to hold the final position of each exercise for 5s. The four types of bridge exercise were performed in simple randomized order. Fig. 2 shows the four types of bridge exercise used in this study.
Statistical analyses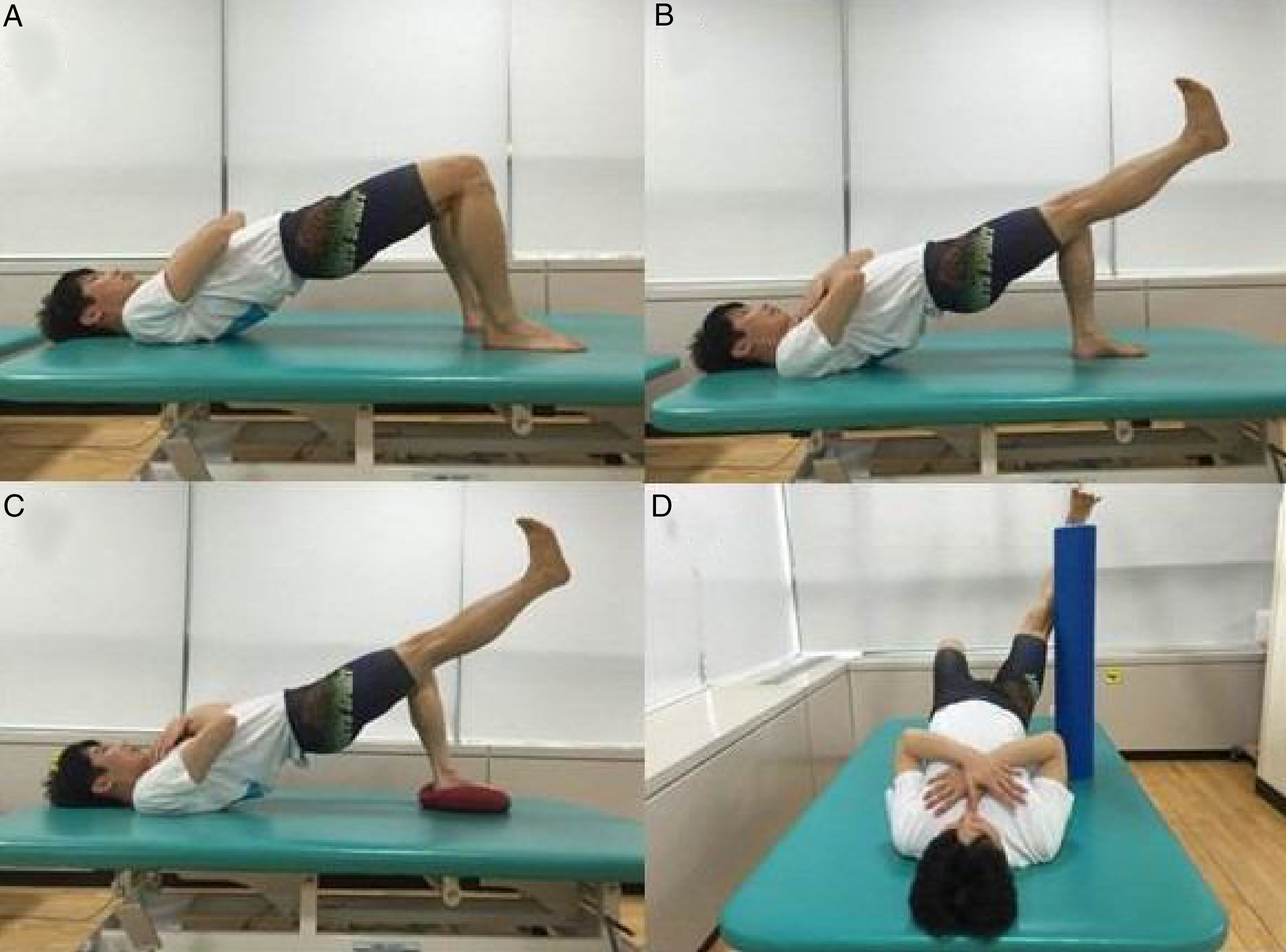
Statistical analysis was performed using the Statistical Package for the Social Sciences ver. 18.0 (SPSS, Chicago, IL, USA). All EMG data were calculated and are expressed as the mean and standard deviation. Two-way repeated-measures analysis of variance was used to compare EMG amplitude of each muscle (IO, RA, ES, and MF) with the factors: exercise (four bridge exercises) and side (right and left). When significant interaction or main effect was found for any item, post hoc analysis for multiple pairwise comparisons was performed using the Bonferroni correction. The level of statistical significance (p) was set at 0.05.
ResultsTable 1 summarizes the EMG data collected for the bilateral IO, RA, ES, and MF during four types of bridge exercise. With respect to IO muscle activity, there was no significant exercise-by-side interaction (p=0.32). However, we found that exercise had a main effect on IO activation (p<0.01). In the post hoc pairwise analysis, bilateral IO showed greater EMG activity during SLBE (right IO, p=0.01; left IO, p=0.04), SLBU (right IO, p<0.01; left IO, p<0.01), and SLHB (right IO, p=0.03; left IO, p=0.02) compared with BE (Fig. 3).
EMG activity (%MVIC) of the trunk muscles during bridge exercise.
| Muscle | Side | Mean±Standard deviation | p value | |||||
|---|---|---|---|---|---|---|---|---|
| BE | SLBE | SLBU | SLHB | Exercise effect | Side effect | interaction | ||
| IO | Right | 4.59±3.59b,c | 9.62±5.74a | 9.14±4.67a | 13.60±9.72a | <0.01* | 0.13 | 0.32 |
| Left | 4.62±3.70b,c | 8.09±6.10a | 7.78±4.69a | 9.19±6.50a | ||||
| RA | Right | 6.58±3.63b,c | 10.78±6.37a | 11.81±7.01a | 14.56±9.24a,c | 0.01* | 0.19 | 0.02* |
| Left | 6.90±6.06c | 8.65±6.06 | 9.62±6.76a | 10.32±6.45a,b | ||||
| ES | Right | 20.84±14.79d | 27.66±20.46d | 25.78±22.07d | 25.52±18.50d | 0.05 | 0.02* | 0.60 |
| Left | 18.48±14.11 | 22.29±16.37 | 21.13±18.58 | 19.58±15.63 | ||||
| MF | Right | 15.88±11.50 | 18.07±14.06 | 17.83±16.20 | 16.17±11.85 | 0.11 | 0.35 | 0.15 |
| Left | 15.29±9.68 | 20.44±13.20 | 19.54±14.53 | 19.06±11.44 | ||||
RA, rectus abdominis; IO, internal oblique; ES, erector spine; MF, multifidus; BE, bridge exercise; SLBE, single leg lift bridge exercise; SLBU, single leg lift bridge exercise on an unstable surface; SLHB, single leg lift hip abduction bridge exercise.
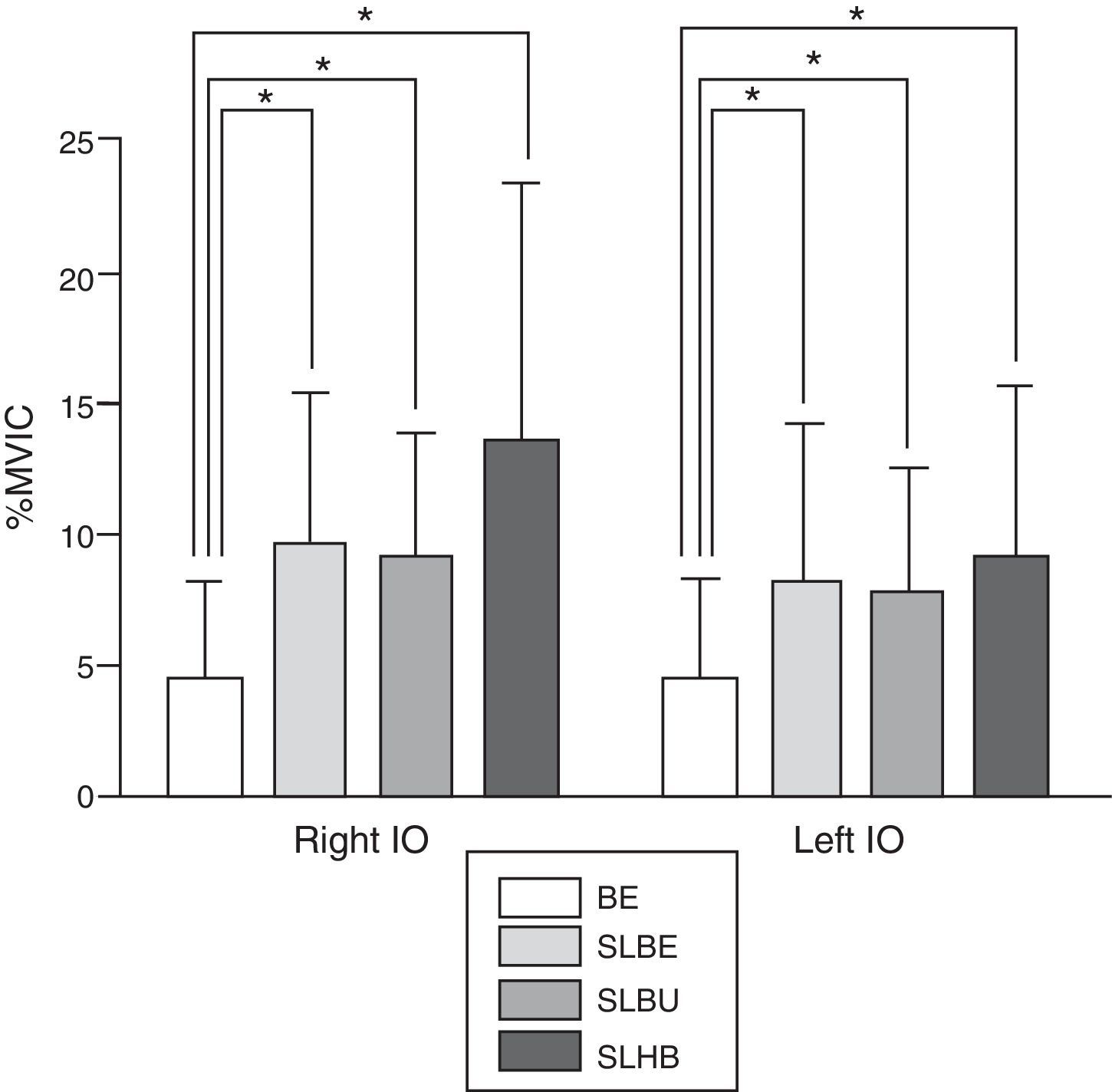
Differences in IO muscle activity (%MVIC) among bridge exercise (BE), single-leg-lift bridge exercise (SLBE), single-leg-lift bridge exercise on an unstable surface (SLBU), and single-leg-lift hip abduction bridge exercise (SLHB). The right leg was lifted during SLBE, SLBU, and SLHB. *p<0.05.
We found significant exercise-by-side interaction (p=0.02) and exercise effect (p=0.01) for RA muscle activity. The post hoc pairwise analysis showed that right RA activity was greater during SLBE (p=0.01), SLBU (p=0.01), and SLHB (p=0.01) compared with BE, while greater right RA activity was found during SLHB (p=0.02) compared with SLBU (Fig. 4). The left RA showed greater EMG activity during SLBU (p=0.01) and SLHB (p=0.04) compared with BE, and greater EMG activity during SLHB (p=0.02) compared with SLBE (Fig. 4).
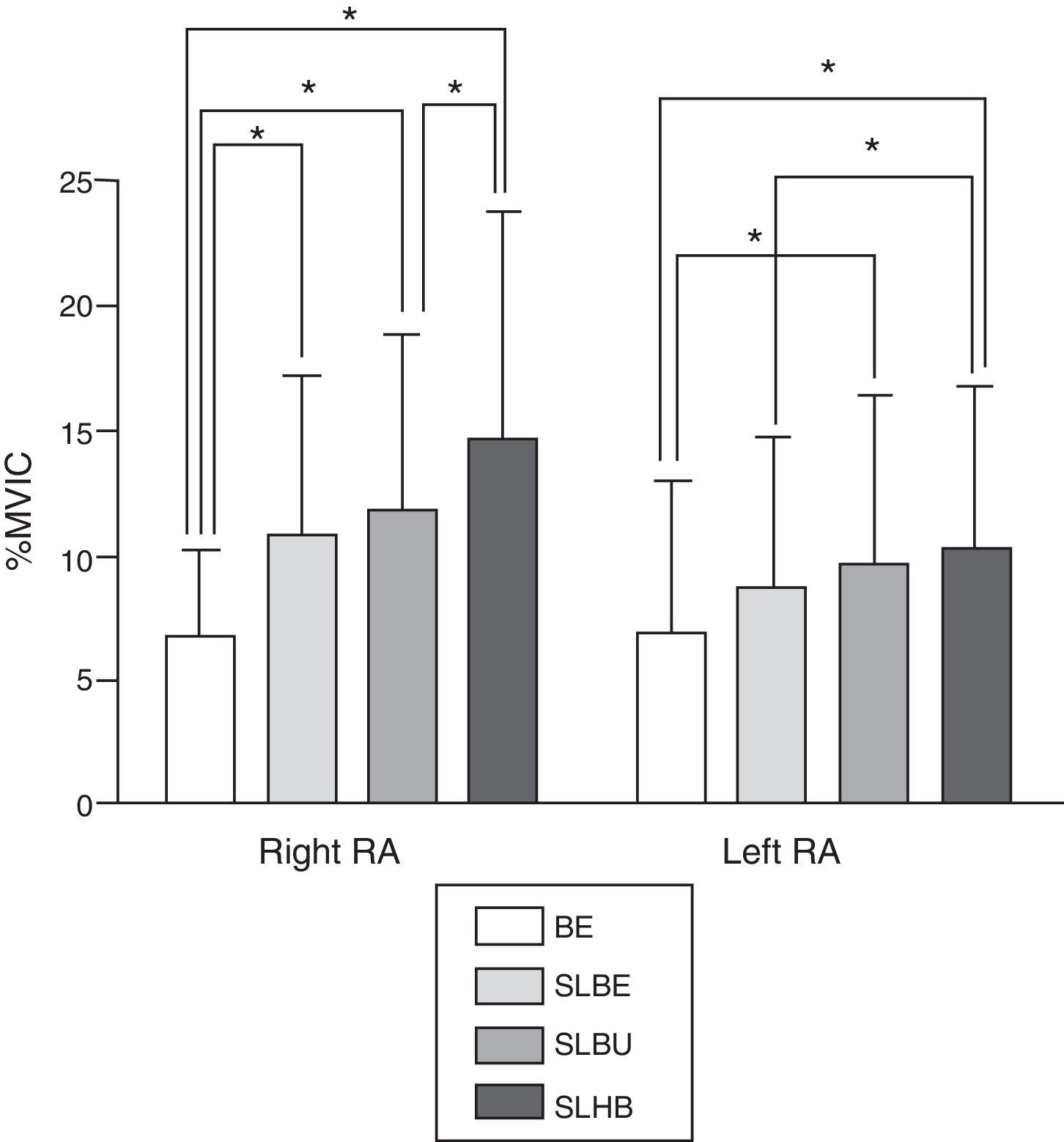
Differences in RA muscle activity (%MVIC) among bridge exercise (BE), single-leg-lift bridge exercise (SLBE), single-leg-lift bridge exercise on an unstable surface (SLBU), and single-leg-lift hip abduction bridge exercise (SLHB). The right leg was lifted during SLBE, SLBU, and SLHB. *p<0.05.
With respect ES muscle activation, significant main effect for side was found (p=0.02), while there was no significant exercise-by-side interaction (p=0.60) and main effect for exercise (p=0.05). The post hoc pairwise analysis showed that right ES muscle activity was greater than left ES during BE (p=0.03), SLBE (p=0.04), SLBU (p=0.02), SLHB (p=0.04). For MF, no significant exercise-by-side interaction (p=0.15) and main effect for exercise (p=0.11) and side (p=0.35) were found.
DiscussionWe examined the influence of modified bridge exercises (i.e., bridge exercises with hip abduction or on an unstable surface) on the EMG activities of the IO, RA, ES, and MF during bridge exercise. This study found that bridge exercises with hip abduction or on an unstable surface facilitated bilateral IO and RA activity, but not ES and MF activity.
Modified bridge exercises are commonly recommended to increase trunk muscle activity.9,10 The IO is crucial for improving trunk stability.19 It is reported that inferior fiber of IO is attached to the lumbar spine indirectly through thoracolumbar fascia.20,21 Therefore, activation of IO increases stiffness of lumbar spine and improve trunk stability.20 In this study, bilateral IO muscle activity increased significantly with the modified bridge exercises compared with the standard bridge exercise. The modified bridge exercise increases activation of the IO to maintain the bridge posture in unstable conditions.9,20 During a modified bridge exercise, the leg is lifted and the base of support (BOS) is reduced. It is thought that the activities of the bilateral IO are significantly increased in the process of overcoming the instability of the body caused by reduction of the BOS. However, the IO activity did not differ significantly among SLBE, SLBU, and SLHB, although right IO muscle activity was increased about 41–48% during SLHB compared with SLBU and SLBE. We infer that the relatively small sample size and large standard deviation of IO muscle activity during exercises may have contributed to non-significant changes in right IO muscle activity among modified bridge exercises.
In this study, the bilateral RA muscle activity increased significantly with SLBU and SLHB compared with BE. The RA is the major flexor of the torso compared with other abdominal wall muscles, and it plays a role in movement and stabilization of the lumbar spine.21 We believe that the RA activity was increased significantly because the BOS during the SLBU and SLHB is narrower than that during the BE, making it difficult to maintain trunk posture. In addition, we found right RA muscle activity was significantly increased during SLBE compared with BE, as well as during SLHB compared SLBU, while there was no significant change in left RA muscle activity between SLBE and BE, as well as between SLHB and SLBU. These findings indicate that RA muscle activity is only changed in the ipsilateral side of leg-lift corresponding to leg position or movement. During SLBE, hip flexor, such as rectus femoris, may be activated to maintain single-leg-lift posture against gravitational force.22 In the case that hip flexor is overactivated during single-leg-lift, pelvis is rotated anteriorly. Sufficient RA muscle activity is required during single-leg-lift task to maintain neutral pelvic posture.22 Thus, it is reasonable that right RA muscle activity was increased to maintain neutral pelvic posture during right single-leg-lift task such as SLBE. With respect to SLHB, hip abduction moves center of mass laterally, which could increase torque about the transverse plane leading to rotation of lumbo-pelvis. It has been stated that increase in lumbar extension and rotation torque generated by leg-lift movement cause counterbalanced compensatory abdominal muscle contraction.23,24 Considering the compensatory role of abdominal muscle, we infer that compensatory right RA muscle contraction to counterbalance rotation torque in the lumbo-pelvic region caused by hip abduction may influence our results.
In the present study, main effect of side was found in the ES muscle activity. Previous findings showed that asymmetrical sport activity and handedness could influence asymmetrical paraspinal muscle morphology.25,26 Considering increase in right ES compared with left ES even during BE in the present study, it is possible that asymmetrical activities in working and daily activities and/or handedness of participants may influence morphology and/or neuromuscular control of ES, resulting in difference in RA muscle activity between right and left sides.
We found no significant main effect of exercise, as well as exercise-by-side interaction, in ES and MF muscle activities. This is consistent with other reports that found no influence of modified bridge exercises on ES activity in healthy adults compared with conventional bridge exercises.8,27 Bridge exercises with single-leg-lift are more challenging for the motor control system, which produces a more intense co-activation of trunk muscles to improve trunk stability.8 During conventional bridge exercise in the present study, back muscles were already activated at a relatively moderate level (15–20%MVIC). When back muscles are activated with moderate level, abdominal muscles were greatly recruited during modified bridge exercise to produce co-activation of trunk muscles.8 Therefore, we consider that no significant differences in EMG activities of back muscles between bridge exercises may result from activation of back muscles at relatively moderate level in this study. Additionally, it is reasonable that greater activation of abdominal muscles rather than back muscles is required to counterbalance rotation torque in the lumbo-plevic region during bridge exercises with single-leg-lift.
In the present study, we demonstrate changes in trunk muscle activity between various trunk stabilization exercises using modified bridge exercises. Considering that core or trunk stability is defined as the ability to control optimal trunk position and movement through neuromuscular system during static and dynamic conditions,28 we infer that trunk stabilization exercise using various modified bridge exercises improved motor control through neuromuscular system, which induces suitable trunk muscle activation to keep neutral lumbo-pelvic posture during modified bridge exercises. However, it is difficult to conclude that these trunk muscle activities are sufficient to gain increased muscle strength. Nevertheless, it has been suggested that muscle activity is significantly correlated to muscle strength.29,30 Based on previous findings,29,30 it is possible that the modified bridge exercises used in our study may lead to much larger %MVIC value in patients with low back pain or individuals with weaker trunk muscle strength compared with healthy individuals who participated in the present study. Thus, it is inferred that long-term modified bridge exercises for patients or weaker individuals lead to greater trunk muscle activation, which may contribute to trunk muscle stability.
From a clinical perspective, our findings provide useful information regarding muscle activation pattern of abdominal muscle and trunk extensor muscle during bridge exercise. However, our findings demonstrated that various bridge exercises resulted in more activation of trunk extensor muscles (15–25%MVIC) than abdominal muscles (<14%MVIC). These findings indicate that bridge exercise is appropriate to produce greater muscle activation of trunk extensor muscles rather than abdominal muscles. Thus, clinicians need to consider various modified bridge exercises as a strategy for enhancing co-activation of abdominal and back muscles rather than an approach focusing only abdominal muscles.
Several limitations of this study should be considered. First, this study used surface EMG, which can record muscle activity from neighboring muscles and therefore may not accurately represent the muscle activity. Also, it is difficult to measure selective activation of transverse abdominis, although inferior fiber of IO represents mixture activation of transverse abdominis and IO.31 Second, the individuals comprised a small sample of the general population and were healthy males and females in their 20s and 30s. Therefore, our results need to be cautious for patients. However, the results of this study might suggest the exercise methods for a step-by-step exercise matched the characteristics of individuals. Finally, this study had a relatively low proportion of females. Additional studies with more individuals should compare the effectiveness of long-term exercise performance and the activity of several trunk muscles.
ConclusionsIn this study, healthy adults performed four types of bridge exercise (BE, SLBE, SLBU, and SLHB). Our findings demonstrate that various modified bride exercises could increase trunk muscle activity. Thus, the present study suggests that hip abduction and unstable conditions in bridge exercises are more beneficial for facilitating co-activation of trunk muscles compared with standard bridge exercises.
Conflicts of interestThe authors declare no conflicts of interest.
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (No. 2015R1D1A1A01056853).



