







Both eccentric training and neuromuscular electrical stimulation (NMES) are used for quadriceps strengthening. However, the effects of these interventions combined are unclear.
ObjectivesTo compare the effects of eccentric training combined to NMES and eccentric training alone on structure, strength, and functional performance of knee extensor muscles of healthy subjects.
MethodsThis is a three-arm, single-blinded, randomized controlled trial. Forty-three volunteers (18–35 years) completed the full study schedule: control group (n=15); eccentric training group (ECC; n=15); and eccentric training combined to NMES group (ECC+NMES; n=13). Eccentric training program was performed twice a week for 6 weeks. A biphasic pulsed current (400μs; 80Hz; maximal tolerated intensity) was applied simultaneously to voluntary exercise for ECC+NMES group. Muscle structure (ultrasonography of vastus lateralis – VL, and rectus femoris – RF), strength (isokinetic dynamometry) and functional capacity (single hop test) were assessed before and after the training program by blinded researchers to groups allocation.
ResultsControl group had no changes throughout the study in any outcome. Eccentric training (with or without NMES) did not affect concentric peak torque, hop test, and VL pennation angle (effect sizes>0.2). ECC and ECC+NMES programs generated significant adaptations (small to moderate effect sizes) on isometric (8–11%) and eccentric (13%) peak torques, VL muscle thickness (5%), VL fascicle length (5–8%), RF muscle thickness (8–9%), RF pennation angle (−2%), and RF fascicle length (12%).
ConclusionNMES combined to eccentric training did not influence consistently the type or magnitude of adaptations provoked by knee extensor eccentric training alone in healthy subjects.
Strength training (or resistance training) is characterized by the systematic execution of voluntary muscular contractions against external loads, and it is considered the most appropriate method for muscular strengthening.1 Despite strength training programs are usually performed with constant load during concentric and eccentric muscle contractions (i.e., conventional strength training), the advantages of regimens using eccentric overload have been widely evidenced in the literature (for a review, see Baroni et al.2 and Douglas et al.3). These advantages include higher muscle strength gains, faster hypertrophic response and increased muscular fascicle length compared to those obtained in conventional strength training programs.2,3 Therefore, eccentric training has been studied as an interventional strategy directed to performance enhancement, injury prevention and rehabilitation.4
As well as strength training using voluntary contractions, neuromuscular electrical stimulation (NMES) is an effective strengthening method for healthy and impaired muscles.5 Although randomized controlled trials have shown the positive effect of NMES training programs on muscle performance of healthy subjects6 and athletes,7 NMES seems to be more beneficial when applied to subjects affected by musculoskeletal disorders,8 probably due to the deleterious effects provoked by reduced use9 and arthrogenic inhibition.10 Therefore, rehabilitation programs using NMES have been proposed for subjects with several conditions, such as anterior cruciate ligament (ACL) reconstruction,11 patellofemoral pain syndrome,12 and knee osteoarthritis.13
Evidences suggest that NMES has similar effects to voluntary exercise for recovering muscle mass and strength after disuse/immobilization periods,8 but it remains as a complementary approach to voluntary exercise in the musculoskeletal rehabilitation context. In addition, healthy subjects trained with voluntary exercises usually present higher strength gains than those trained with NMES.5 Nevertheless, NMES used simultaneously to voluntary muscle contraction (i.e., superimposed NMES) have been suggested as a more effective strategy for muscular strengthening than those training strategies applied apart.14 Some studies have found greater muscle strengthening with superimposed NMES compared to voluntary exercise,15–17 while others showed similar gains with the two training methods.18,19 Thus, this combined intervention needs further investigation.
The aim of this study was to compare the effects of eccentric training combined to NMES and eccentric training alone on structure, strength, and functional performance of knee extensor muscles of healthy subjects. Our hypothesis was that the superimposed NMES would lead to greater gains than eccentric training alone.
MethodsStudy designThis was a three-arm, single-blinded, randomized controlled trial. Forty-five volunteers were randomically allocated in one of three groups: control group; eccentric training (ECC) group; and eccentric training combined to NMES (ECC+NMES) group. This trial was approved by the Research Ethics Committee of the Universidade Federal de Ciências da Saúde de Porto Alegre-UFCSPA (#1.500.581), Porto Alegre, RS, Brazil and registered at Registro Brasileiro de Ensaios Clínicos (RBR-3fg9cd).
ParticipantsA convenience sampling of undergraduate and graduate students, aged between 18 and 35 years, physically active but not specialized of any sport were invited to participate in the study. Those subjects who presented one or more of the following characteristics were excluded: (1) presence of any health condition that contraindicated or prevented high intensity exercise; (2) history of knee surgery (e.g., meniscal repair, ACL or other ligaments reconstruction) or recent lower-limb musculoskeletal injury that could impair their performance during tests or interventions (e.g., muscle injury, tendinopathy, patellofemoral pain); (3) engagement in any kind of training program during the study period; (4) engagement in lower limb strength training program during the three months preceding participation in the study; (5) use of ergogenic supplements to improve physical performance and/or muscle mass. All volunteers signed an informed consent before data collection.
Sample-size calculationSample size was estimated based on eccentric peak torque results from the study by Baroni et al.20 Based on a power of 80% and level of significance of 5%, this study should include at least 12 individuals per group. Considering a possible sample loss of 20% throughout the study, three extra participants were added in each group, totalling 45 individuals divided into three groups (15 participants per group).
Randomization and blindingThe randomization process was conducted by an assistant not involved with recruitment, assessment or treatment. Blocks of six participants were independently randomized in a 1:1:1 allocation ratio. Researchers involved in training sessions did not attend to evaluation sessions and researchers responsible for evaluations did not follow the training sessions. Due to the nature of interventions (voluntary exercise and electrical stimulation), volunteers and therapists were not blinded to treatments’ allocation.
Outcomes and follow-upAs presented in Fig. 1, measurements of muscle structure (by ultrasonography), torque production capacity (by isometric and isokinetic dynamometry) and functional capacity (by single hop test) were performed one week before and one week after the knee extensor eccentric training program in both ECC and ECC+NMES groups. Participants in the control group were instructed to maintain their regular physical activity routine during the period between assessments. All procedures took place in the Physiotherapy Laboratory at the UFCSPA (Porto Alegre, RS, Brazil). Knee extensor eccentric peak torque was the primary outcome, and the secondary outcomes were: knee extensor isometric and concentric peak torques; muscle thickness, pennation angle and fascicle length of vastus lateralis (VL) and rectus femoris (RF); and hop test.
AssessmentsMuscle architecture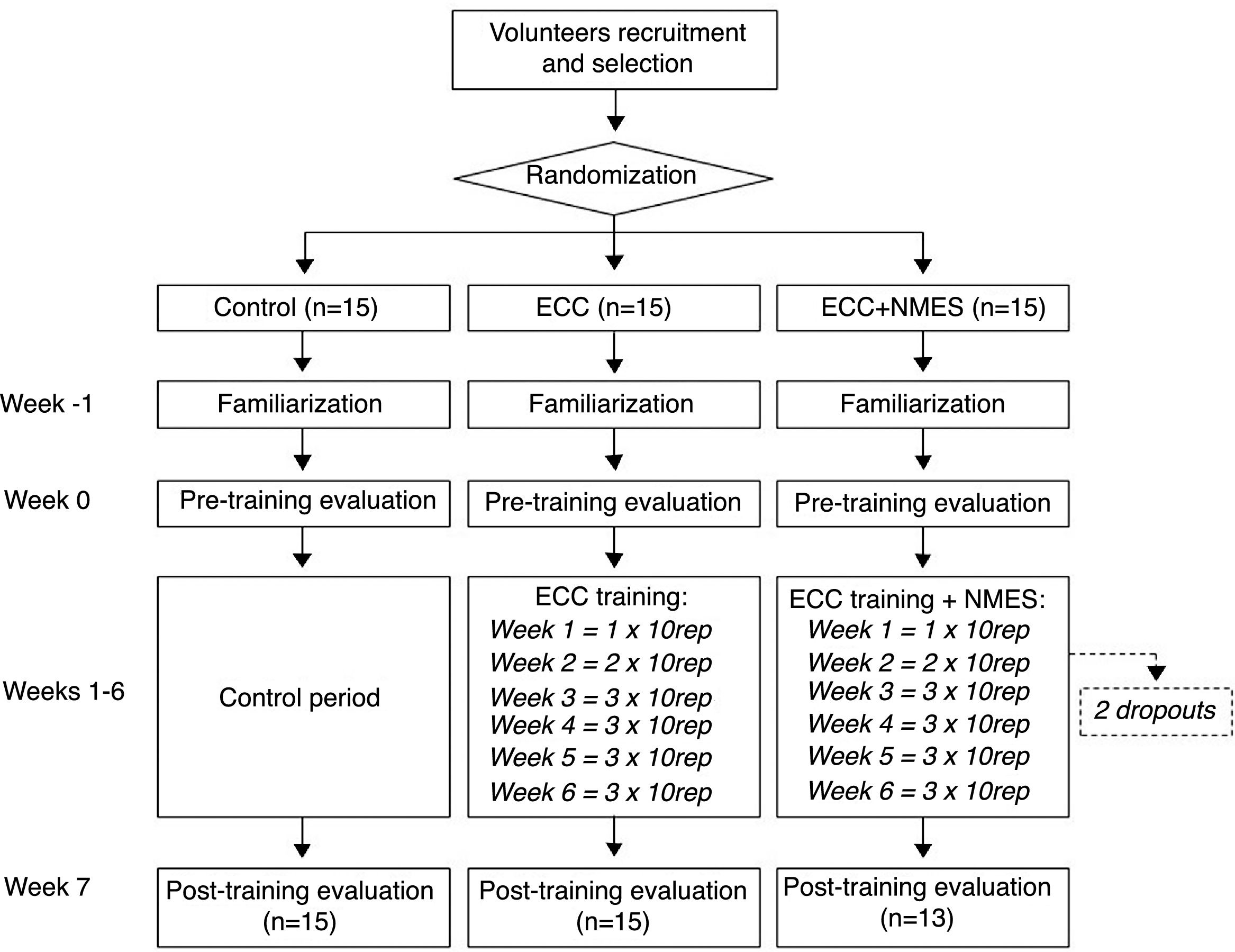
Ultrasonographic images of the dominant lower limb were captured using a GE Vivid I equipment (GE Medical Systems, Fairland, USA), along with a linear array probe (48mm, 7.5MHz). A single researcher was responsible for collection and analysis of the images from the VL and RF muscles, following previously described protocols.21 Measures were obtained at 50% of the length between the knee joint line and the anterior superior iliac spine. Participants were evaluated laying supine, with both knees totally extended and muscles relaxed. A minimal resting period of 10min was respected before capturing the images. Maps were drawn in transparent sheets to identify the probe site in relation to anatomical references (e.g., patellar margin) and skin marks (e.g., scars or nevi). This procedure ensured similar positioning of the ultrasonography probe in the pre- and post-intervention measurements. Three images were collected from each muscle and analyzed using the ImageJ software (National Institute of Health, USA). Muscle thickness, pennation angle and fascicle length were determined following validated procedures.22 Mean values obtained from the three ultrasonographic images of each muscle were used for statistical analysis.
Muscle strengthIsometric and isokinetic evaluations were performed on a Biodex System 4 isokinetic dynamometer (Biodex Medical Systems, New York, USA). After a 5-min warm-up on a cycle ergometer, participants were positioned at the dynamometer according to manufacturer's instructions. Ten knee flexion-extension submaximal repetitions at 120°s−1 were performed as specific warm-up. Knee extensor isometric peak torque was obtained through three 5-s maximal voluntary isometric contractions (MVIC) at 60° of knee flexion (0°=full extension). An extra MVIC was performed when a variation higher than 10% was observed among the three preceding MVIC values. Two sets of three maximal concentric contractions (angular velocity=60°s−1; range of motion=10°–100°) and two sets of three maximal eccentric contractions (angular velocity=60°s−1; range of motion=30°–90°) was used to measure knee extensor peak torques.20 A 2-min resting interval was given between tests. The highest peak torque values from each contraction type were used for analysis.
Functional performanceFunctional performance was assessed through the single hop test.23 Participants were instructed to jump as far as possible standing on the dominant leg only, starting from a static semi-squatting position (approximately 90° of knee flexion) and keeping this position after the jump. Instructions to move the upper limbs freely during the test were also given. The distance between the starting sign (marked on the ground) and the participants’ tiptoe after landing was measured. Subjects performed three to five attempts, with minimal intervals of 30s between attempts.
InterventionsEccentric trainingThe same eccentric training program was used for both ECC and ECC+NMES groups. The difference between groups was the electrical stimulation applied on the quadriceps muscle of those in the ECC+NMES group concomitantly to eccentric exercise execution (see next session for details). Participants attended the eccentric training program twice a week (with minimal 72-h interval) during 6 weeks. In each session, after cycle ergometer warm-up was completed, participants performed one to three sets of 10 repetitions (Fig. 1), resting for 1min between sets.
Eccentric training was performed on a knee extensor chair (5kg each load bar). Training load of each participant was determined based on their unilateral one-maximal repetition (1RM) test performed according to conventional protocol (i.e., concentric followed by eccentric contraction). After warm-up and familiarization with the test using a moderate load, the load corresponding to 1RM was determined through two to four attempts. The 1RM test was performed at the week preceding the eccentric training program commencement and repeated following two and four weeks of training for training load adjustment. The load used in the eccentric training program was the same load obtained at the 1RM test (i.e., unilateral maximal concentric load).
During training sessions, participants performed the concentric movement phase by contracting both limbs and the eccentric phase while using only the dominant limb (i.e., 100% of the load on the dominant limb during the eccentric phase), as shown in Fig. 2. The researcher responsible for applying the training sessions used a metronome to monitor the movement cadence and verbally instructed the participants. The concentric phase was performed during approximately 1s and the eccentric phase during 4s. Between each repetition, a 5-s resting interval was employed. In the ECC+NMES group, the movement cadence was synchronized with the electric current delivered by the equipment.
NMES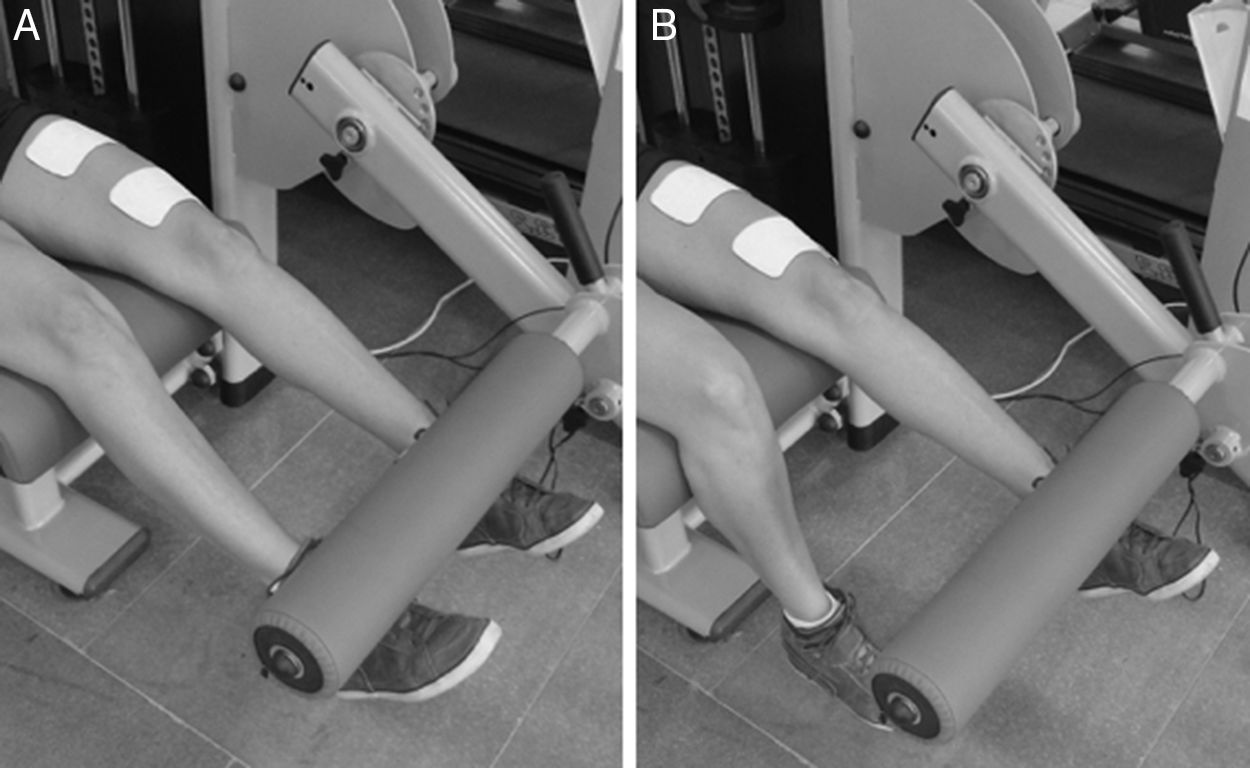
The electrical stimulation of the ECC+NMES group was applied using an Intelect Advanced equipment (Chattanooga Medical Supply, Chattanooga, USA). The current was applied by two electrodes (7.5cm×13cm; Valutrode, São Paulo) attached to the skin over the quadriceps muscle belly of the dominant limb (Fig. 2). The proximal electrode was placed over the RF motor point (individually determined a priori),24 while the distal electrode was placed over the bellies of the vastus medialis and VL muscles. NMES was applied with a biphasic, symmetric, rectangular, pulsed current with pulse duration of 400μs and a frequency of 80Hz.13 ON-OFF (contraction-rest) periods were established as 5s. Current intensity was set at the maximally tolerated level for each subject. As soon as the electrical stimuli began, the participant performed the concentric knee extensor phase using both limbs in approximately one second, followed by the eccentric phase using only the dominant limb during the four remaining seconds of electrical stimulation. The researcher provided verbal instructions and encouragement to the volunteer during the exercise.
Statistical analysisOnly volunteers who completed the full study schedule (assessments for all groups, and training sessions for ECC and ECC+NMES groups) were included in statistical analysis. Within-group analysis to verify training effects were performed with the effect size (ES) calculation through the Cohen's d [ES=(Mpost−Mpre)/SDpooled, where Mpost is the mean post-training measure, Mpre is the mean pre-training measure, and SDpooled is the pooled standard deviation of the pre- and post-measurement], and training effects were considered as “trivial” (<0.2), “small” (≥0.2), “moderate” (≥0.6), “large” (≥1.2), or “very large” (≥2.0).25
Longitudinal percent changes (pre- to post-training) were used for between-group analysis. Data were analyzed for practical significance using magnitude-based inferences because traditional statistical approaches often do not indicate the magnitude of an effect, which is typically more relevant to clinicians than statistical significance.25 The chances of a possible substantial effect favorable to each group were calculated [i.e., greater that the smallest worthwhile change (0.2 multiplied by the between-subject standard deviation)]. Quantitative chances of trivial effects and substantial effects for each group were assessed qualitatively as follows: <1%, almost certainly not; 1–5%, very unlikely; 5–25%, unlikely; 25–75%=possibly; 75–95%=likely; 95–99%=very likely; >99%=almost certain.26 When the substantial values for each group were both >5%, the inference was classified as unclear.26
ResultsTwo participants dropped out of the study due to scheduling incompatibility with the training sessions at the laboratory; thus 43 subjects completed the protocol (Fig. 1) and were included in statistical analysis. Table 1 shows the volunteers’ characteristics.
Within-group analysis is presented in Table 2. Control group had no changes throughout the study in any outcome. ECC and ECC+NMES groups had small to moderate effect sizes for isometric peak torque, eccentric peak torque, VL muscle thickness, VL fascicle length, RF muscle thickness, RF pennation angle, and RF fascicle length. Eccentric training (with or without NMES) did not affect concentric peak torque, hop test and VL pennation angle.
Intragroup analysis for all outcomes assessed in the study.
| Control (n=15) | ECC (n=15) | ECC+NMES (n=13) | |
|---|---|---|---|
| ISO peak torque | |||
| Pre (Nm) | 205.81±52.81 | 197.71±59.88 | 211.49±58.68 |
| Post (Nm) | 198.95±51.09 | 218.23±66.02 | 227.82±65.27 |
| Δ% | −3.18±3.74 | 10.71±8.94 | 7.82±9.82 |
| Effect size | 0.14 | 0.34a | 0.27a |
| CON peak torque | |||
| Pre (Nm) | 177.09±46.25 | 172.21±49.21 | 182.44±57.14 |
| Post (Nm) | 173.80±47.96 | 178.93±50.56 | 185.58±55.74 |
| Δ% | −2.26±5.51 | 4.22±6.30 | 2.14±4.42 |
| Effect size | 0.07 | 0.14 | 0.06 |
| ECC peak torque | |||
| Pre (Nm) | 212.37±72.16 | 218.75±65.16 | 219.22±60.41 |
| Post (Nm) | 217.95±72.67 | 246.13±74.18 | 245.15±61.55 |
| Δ% | 3.10±7.62 | 12.92±9.58 | 13.00±11.30 |
| Effect size | 0.08 | 0.41a | 0.44a |
| Hop test | |||
| Pre (cm) | 166.33±39.95 | 150.33±33.29 | 156.42±38.68 |
| Post (cm) | 167.47±38.34 | 154.47±36.20 | 162.96±41.48 |
| Δ% | 0.96±3.50 | 2.59±3.40 | 4.01±2.65 |
| Effect size | 0.03 | 0.12 | 0.17 |
| VL muscle thickness | |||
| Pre (cm) | 1.91±0.40 | 2.15±0.39 | 2.06±0.30 |
| Post (cm) | 1.91±0.39 | 2.24±0.35 | 2.14±0.26 |
| Δ% | 0.13±1.22 | 4.48±4.44 | 4.59±5.72 |
| Effect size | 0.00 | 0.45a | 0.30a |
| VL pennation angle | |||
| Pre (degrees) | 13.51±1.91 | 15.17±1.52 | 15.05±1.51 |
| Post (degrees) | 13.48±1.92 | 14.96±1.51 | 14.91±1.54 |
| Δ% | −0.23±1.01 | −1.39±0.87 | −0.96±0.74 |
| Effect size | 0.02 | 0.14 | 0.10 |
| VL fascicle length | |||
| Pre (cm) | 8.18±1.04 | 8.56±1.28 | 8.07±0.99 |
| Post (cm) | 8.13±0.97 | 8.94±1.12 | 8.69±1.07 |
| Δ% | −0.54±2.65 | 4.82±4.86 | 7.75±5.21 |
| Effect size | 0.05 | 0.33a | 0.63b |
| RF muscle thickness | |||
| Pre (cm) | 1.75±0.37 | 1.84±0.38 | 1.86±0.44 |
| Post (cm) | 1.75±0.38 | 1.98±0.36 | 2.00±0.45 |
| Δ% | −0.25±1.34 | 8.61±8.19 | 8.33±6.51 |
| Effect size | 0.00 | 0.39a | 0.33a |
| RF pennation angle | |||
| Pre (degrees) | 7.74±0.83 | 8.38±0.69 | 8.66±0.39 |
| Post (degrees) | 7.73±0.86 | 8.18±0.68 | 8.52±0.40 |
| Δ% | −0.11±1.01 | −2.43±1.08 | −1.55±1.13 |
| Effect size | 0.01 | 0.30a | 0.37a |
| RF fascicle length | |||
| Pre (cm) | 11.79±2.26 | 11.09±2.39 | 11.27±2.76 |
| Post (cm) | 11.78±2.23 | 12.31±2.29 | 12.56±2.89 |
| Δ% | −0.07±1.02 | 11.78±7.14 | 11.90±7.29 |
| Effect size | 0.00 | 0.54a | 0.48a |
CON, concentric; ECC, eccentric; ISO, isometric; RF, rectus femoris; VL, vastus lateralis; Δ%, percent change.
Between-group analysis is illustrated in Fig. 3. The magnitude-based inference approach supports that changes in all outcomes “likely”, “very likely”, or “almost certain” favour ECC and ECC+NMES groups when compared to control group (Fig. 3A and B, respectively). When ECC and ECC+NMES were compared: unclear effects were observed for peak torques (isometric, concentric and eccentric), muscle thicknesses (VL and RF), and RF fascicle length; changes on VL and RF pennation angles “likely” favour ECC group; changes on VL fascicle length “likely” favour ECC+NMES group; and changes on hop test “possibly” favour ECC+NMES group.
Discussion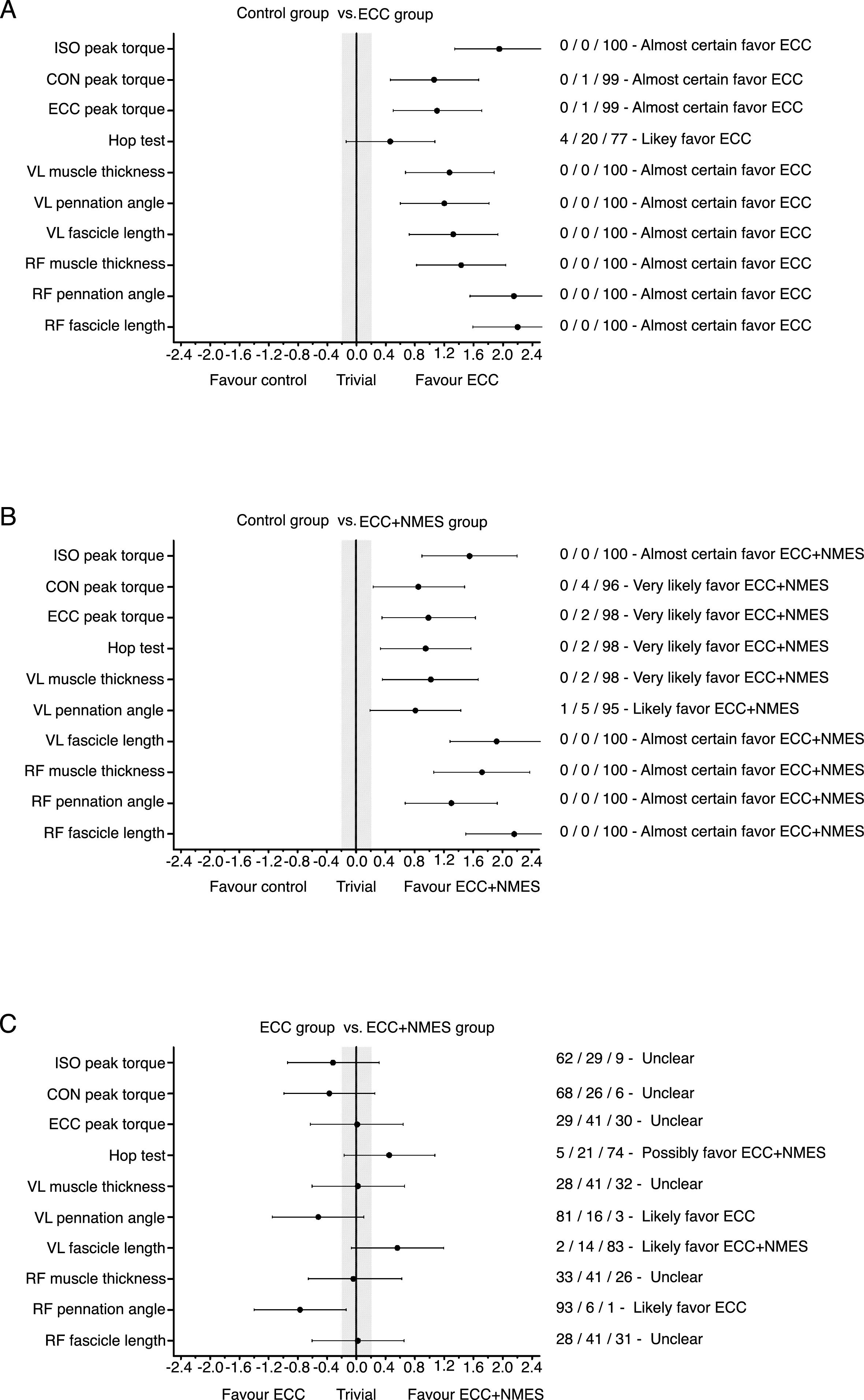
To the best of our knowledge, this study is pioneer in verifying the effects of eccentric training combined to NMES and compare with those provided by eccentric training alone. Our main findings are: (i) the eccentric training increased knee extensor isometric and eccentric muscle strength; (ii) the eccentric training increased VL and RF muscle thickness and fascicle length; (iii) NMES superimposed to voluntary exercise did not influence the type or magnitude of the eccentric training adaptation.
In this study, we opted to substitute the purely eccentric training with isokinetic dynamometers20,21 or the eccentric-overload training with flywheel equipment,27,28 both commonly used in laboratory studies, by a training program using a simple knee extensor chair (i.e., a constant load equipment). The strategy designed to emphasize the eccentric component of the movement was performing the concentric phase with both limbs and the eccentric phase using only the dominant one,29,30 which avoids the need for external assistance to execute the concentric movement phase. Moreover, we chose a low frequency current (80Hz), since there is no difference on evoked strength and discomfort among low- and kilohertz-frequency31; as well as a pulse duration (400μs) close to those commonly used in research and possible to be applied by most commercialized electrotherapy equipment. Thus, the experimental design of this study attempted to mimic the conditions found in most of the training and rehabilitation centers; it means that our training program can be easily applied by clinicians.
Strength gains are classically attributed to increments in motor unit activation capacity (i.e., neural factors) and to the hypertrophy of muscle fibers (i.e., structural factors).32 Although the increased strength in the first weeks of conventional strength training is mainly due to neural factors, our study and other works with knee extensor eccentric training in isokinetic dynamometers20,21 and flywheel equipment27,28 have demonstrated increased muscle mass within the first month of training. This early hypertrophic response through the increased number of parallel arranged sarcomeres contributes to the muscle strength gains.33 However, the lack of concentric strength gain found in our study further supports the specificity effect of eccentric training, which is associated to neural adaptations provoked by type of contraction emphasized in the training program.2,3 Hence, although we have not included a neural adaptation marker in this study, the learning of eccentric action at cortical and peripheral levels34 is the main explanation for a greater magnitude of change observed in eccentric strength tests.
Muscle hypertrophy promoted by eccentric training is evidenced in our study by the increase in VL and RF muscle thickness. The ∼4–9% increment following 6 weeks of eccentric training using knee extensor chair in our study is similar to those observed after 4 weeks of eccentric training using maximal isokinetic contractions.20 Increased muscle thickness is attributed to augmented pennation angle and/or fascicle length. The changes in pennation angle show contradictory evidence in both conventional strength training and eccentric training, and the limited resolution of ultrasound imaging might be a factor.2 On the other hand, eccentric training programs have been proved effective in increasing the fascicle length of quadriceps,21,28,35 hamstrings36 and plantar flexor muscles,37 differently from what have been observed in most of the conventional strength training studies. This adaptative response occurs in short periods of eccentric training (<4 weeks), and studies in isokinetic,21 flywheel28 and constant load35 conditions have shown increments of 10–20% on the fascicle length of knee extensor muscles. To the best of our knowledge, this is the first study demonstrating that the eccentric training strategy here adopted (i.e., bilateral concentric action followed by unilateral eccentric action) increases the quadriceps muscle fascicle length.
The increased fascicle length induced by eccentric training is due to higher number of serially arranged sarcomeres in the muscle fiber (i.e., sarcomerogenesis),38 which results in important modifications on the muscle mechanics and functional performance. Fiber elongation changes the optimal length of strength production and increases the muscle's shortening velocity.39 Longer fibers have also been associated to functional performance of distinct populations, ranging from elderly subjects40 to elite athletes.41 However, the adaptations on quadriceps muscle strength and architecture were insufficient to determine increments in functional performance of our participants at the single hop test.
While the eccentric training was performed in open kinetic chain (uni-articular exercise), hop test requires a more complex movement at closed kinetic chain. The difference of the motor task required for testing and for training is a possible explanation for the absence of functional improvement in this study.42 The transference of gains in specific muscle properties (e.g., maximal strength and muscle architecture) to functional capacity is the aim of numerous training programs intending to improve physical/sport performance, as well as to prevent and rehabilitate musculoskeletal injuries. Therefore, our findings provide support to the need of inserting ‘functional exercises’ (i.e., global exercises that mimic motor demands) in strength training programs with goals related to functional performance enhancement.
There is no consensus on the advantages of combining NMES with voluntary exercise in comparison to voluntary exercise alone in healthy subjects. Some studies showed that the levels of muscle strengthening with superimposed NMES were higher compared to groups with isolated exercise,15–17 while others showed similar gains with the two training methods.18,19 In our study, ECC and ECC+NMES groups had significant and similar effects on strength (isometric and eccentric peak torques), muscle thicknesses (VL and RF) and RF fascicle length. Since there were no significant longitudinal changes on concentric peak torque, hop test and VL pennation angle (see Table 2), between-group differences in that outcomes were not considered. Therefore, our findings support that NMES superimposed to voluntary exercise do not consistently change the muscular adaptation to eccentric training in healthy subjects.
Our hypothesis was that NMES would be able to optimize the eccentric training responses, based on possible preferential activation of large motor units (i.e., responsible for type II fibers innervation, with high strength production capacity and accentuated hypertrophic response) via NMES due to their more superficial location on the quadriceps muscle and greater axon diameter (i.e., more easily excitable by electrical stimulation once imposing lesser resistance to electrical current flow).8 We cannot affirm that NMES stimulated preferentially large motor units in the present study. But our results suggest that using electrical stimulation concomitantly to voluntary exercise did not affect the muscle adaptations promoted by eccentric training, which raises question on the validity of this method to train young and healthy individuals.
Programs with NMES associated to voluntary exercise have shown superior results compared to voluntary exercise alone in patients with knee osteoarthritis43 and following knee arthtoplasty.44 A straight comparison of our findings with those ones from studies with injured subjects seems inadequate due to population specificity and training regimes employed in each research. But it seems plausible to state that individuals with a certain degree of quadriceps muscle inhibition can experience additional benefits provided by NMES when it is superimposed to voluntary contractions. Therefore, future investigation should focus on the effects of NMES superimposed to eccentric exercise in these populations, and assess superimposed NMES effects on neuromuscular properties, such as quadriceps muscle activation (i.e., superficial electromyography) and inhibition (i.e., twitch interpolation technique).
Since the superimposed NMES is usually employed in rehabilitation programs, the healthy volunteers from our sample may be pointed out as a limitation of the current study. Although our main focus of investigation was the possible benefits of NMES added to an eccentric training programe, a fourth experimental group with NMES training alone (without voluntary exercise) could provide interesting comparisons with ECC and ECC+NMES groups.
ConclusionWe conclude that a 6-week eccentric training program with an extensor chair led to knee extensors strengthening, muscle hypertrophic response, and increased fascicle length; but had no effect on subjects’ hop performance. The addition of NMES (with parameters used in this study) superimposed to voluntary exercise did not influence the type or magnitude of the adaptations induced by eccentric training in healthy subjects.
Conflicts of interestThe authors declare no conflicts of interest.
Research registered at Registro Brasileiro de Ensaios Clínicos (REBEC): # RBR-3fg9cd (http://www.ensaiosclinicos.gov.br/rg/RBR-3fg9cd/).



