
Quarantine periods change routines and behaviors with potential impact on different health outcomes.
ObjectiveTo determine the association between changes in physical activity and sedentary behaviors with changes in back pain during the COVID-19 pandemic quarantine among Brazilian adults.
MethodsThis was a nationwide survey through online questionnaires using data from 43,062 adults (≥ 18 years of age). Information on back pain was assessed using questions about episodes of back pain and worsening symptoms during the quarantine. The pattern of movement behaviors adopted before and during the pandemic were considered for physical inactivity (< 150 min/week of activity), high TV-viewing (≥ 4 h/d), and high computer/tablet use (≥ 4 h/d). Covariates included sex, age group, academic achievement, skin color, working status during the quarantine, and adherence to the quarantine. Logistic regression models were used for statistical analyses (weighted for national representativity).
ResultsBecoming inactive (OR=1.76, 95% CI: 1.32, 2.37), with high TV-viewing (OR=1.35, 95% CI: 1.14, 1.61) and high computer/tablet use (OR=1.39, 95% CI: 1.11, 1.73) during the pandemic were associated with a higher incidence of back pain. The incidence of physical inactivity was also associated with increased back pain (OR=2.71, 95%CI: 1.64, 4.48).
ConclusionsWe conclude that increased physical inactivity and sedentary behaviors due to the COVID-19 pandemic quarantine are associated with the incidence and worsening symptoms of back pain among Brazilian adults.
Back pain is an important concern in terms of public health.1 In addition to its high prevalence, back pain is associated with physical constraints, lower quality of life, and reduced life expectancy.2,3 Although back pain is a major public health problem worldwide, it is projected that the burden of back pain will increase even further in the next few decades, especially in low and middle-income countries.2
One of the main challenges when considering back pain at the population level is that the cause is frequently non-specific, being associated with socioeconomic, physical, behavioral, and mental factors.2,4 Among the causes, in general, healthy lifestyles are suggested as protective against back pain; however, doubts remain about the doses and combinations of healthy behaviors to optimize benefits. Although moderate-intensity physical activity in leisure time seems protective for back pain symptoms,5,6 this is not clear considering other domains of physical activity and specific population groups.7 In addition, little is known about the combination of physical activity with other movement behaviors, such as sedentary time spent on TV-viewing and on personal computers.7
Given the social restriction measures imposed due to the Coronavirus Disease 2019 (COVID-19) pandemic, people's lives have changed and “stay-at-home” messages have reduced opportunities for physical activity practice and increased exposure to many types of sedentary behaviors. Therefore, increases in the level of physical inactivity and sedentary behavior have been reported during the COVID-19 quarantine.8 These behavior changes seem to be associated with cardiovascular,9 metabolic,10 and mental health disorders.11 However, it is not clear how changes in movement behaviors due to the COVID-19 pandemic are associated with musculoskeletal conditions, such as back pain. This information would help the development of interventions to mitigate the potentially harmful effects of quarantine on musculoskeletal health, focusing on the specific type and pattern of movement behaviors. Thus, we investigated the association of changes in movement behaviors due to the COVID-19 pandemic quarantine with back pain among Brazilian adults. Our hypothesis was that increased physical inactivity and high screen-based sedentary time due to the COVID-19 pandemic quarantine are associated with the incidence and worsening of back pain.
MethodsStudy design and settingThe “Brazilian behavioral research during the COVID-19 pandemic” is a cross-sectional health survey using a virtual questionnaire to assess the changes that have occurred in the lives of Brazilians after the arrival of the coronavirus pandemic in the country, related to social restriction initiatives for the protection of people, including quarantine and lockdown. Data collection was conducted between April 24th and May 24th, 2020. All procedures were approved by the National Research Ethics Commission applied by the Oswaldo Cruz Foundation, Rio de Janeiro, RJ, Brazil (opinion n° 3.980.277).
ParticipantsParticipants were invited through a chain sampling procedure. In the first stage, the 15 researchers involved in the study chose a total of 200 other researchers from different states in Brazil. In addition, each researcher in the study chose 20 people from their social network, making a total of 500 people chosen. The people chosen in the first stage were denominated ‘influencers.’ These influencers sent the survey link to at least 12 people from their social networks, following guidance for stratification by sex, age range (18–39; 40–59; 60+), and education level (none or elementary school, high school, and more than high school). In addition, information about the study was disseminated through press releases, social communications from participating research institutions, state health departments, and social media. The survey link was also available at the influencers' research institutions. From the initial sample (n = 45,160), 2026 presented missing data for at least one variable and were excluded from the present analyses, and after further exclusions for missing data, the current study analyzed data for 43,062 participants. The sample was weighted according to characteristics from the National Household Sample Survey (conducted in 2019), considering population in each state, education, age, sex, and prevalence of chronic diseases, aiming at a nationally representative sample. All the participants signed a written consent form accepting the study procedures.
VariablesBack painFirst, participants were asked a general question about an already existing back problem. Next, those with no previous back pain were asked about the occurrence of back pain during the pandemic (incidence) and those who already had back pain were asked about any changes in their back pain during the pandemic. Questions were based on the Brazilian National Health Survey.12 The first question was dichotomic (yes or not): “Do you have any chronic back problems such as chronic back or neck pain, low back pain, sciatica, vertebrae or disc problems?”. The incidence of back pain during the pandemic (among those without chronic back pain) was assessed through the question: “During the pandemic, have you started to feel any back or spinal pain due to changes in habitual activities?”. Possible answers were: (a) yes, a little; (b) yes, a lot; and (c) no. We classified the two first options as “incidence of back pain.” In addition, those who already had back pain before the pandemic were asked: “During the pandemic, how have changes in your habitual activities affected your back pain?”. Possible answers were: (a) maintained; (b) slightly increased; (c) strongly increased; and (d) reduced. We classified options b and c as “increased back pain.”
Movement behaviorsMovement behaviors were assessed through questions previously used in the “Brazilian Telephone-based Risk Factor Surveillance System for Chronic Diseases,” which presented good psychometric properties.13 We used questions referring to each behavior before and during the pandemic, categorizing, for analyses purposes as “changes in movement behaviors” participants who changed category (active/inactive and adequate/high screen time) based on previous studies.14,15
For physical activity before the COVID-19 pandemic, participants were asked “Before the COVID-19 pandemic, on how many days a week did you practice any type of physical exercise or sport? (do not consider physical therapy)”. Possible answers were: (a) less than 1; (b) 1,2; (c) 3,4; or (d) 5 or more. For those reporting physical activity practice, we also asked: “How long did this activity last?”. Possible answers were: (a) less than 30 min; (b) 30–45 min; (c) 46–60 min; or (d) more than 60 min. In addition, for physical activity during the COVID-19 pandemic, we asked: “During the COVID-19 pandemic, on how many days a week do you practice any type of physical exercise or sport? (do not consider physical therapy)”. Possible answers were: (a) less than 1; (b) 1,2; (c) 3,4; or (d) 5 or more. For those reporting physical activity practice, we also asked: “How long does this activity last?”. Possible answers were: (a) less than 30 min; (b) 30–45 min; (c) 46–60 min; or (d) more than 60 min. Physical inactivity was classified as less than 150 min/week of physical activity.16 Physical activity practice patterns were created using four change patterns: (1) consistently active; (2) become active; (3) become inactive; or (4) consistently inactive.
TV-viewing and computer/tablet use were adopted as independent proxies of sedentary behavior. For TV-viewing, participants were asked: “Usually, before the pandemic, how many hours a day did you used to spend watching television?” and “During the pandemic, how many hours a day do you spend watching television?”. For computer/tablet use, participants were asked: “Usually, before the pandemic, how many hours a day did you use to spend on a computer or tablet?” and “During the pandemic, how many hours a day do you spend on a computer or tablet?”. We adopted 4 h/day as cut-offs for high TV-viewing and computer/tablet use as separate outcomes.17 TV-viewing and computer/tablet use patterns were created using four change patterns: (1) consistently low; (2) become low; (3) become high; or (4) consistently high.
CovariatesSociodemographic covariates included sex (male/female), age group (18–29, 30–39, 40–49, 50–59, 60+), highest academic achievement (none or elementary school, high school, and more than high school), and skin color (white, black, brown, and other). Domestic labor during the pandemic was assessed through the question: “Has the pandemic affected the amount and type of your domestic labor?”, and those who reported “a little” or “a lot” were classified as “increased domestic labor”. We also used the working status during the pandemic (normal, home office, not working, for any reasons [including vacation]) and adherence to the quarantine. This last item was assessed through the question: “During the Coronavirus pandemic, to what extent have you restricted (or are you still restricting) contact with people?”, with possible answers: “I have done nothing, I lead a normal life”; “I have tried to take care, stay away from people, reduce contact a little, not visit the elderly, but I have continued to work and go out”; “I have stayed at home just going shopping at the supermarket and pharmacy”; or “stayed strictly at home, leaving only for health care needs”. We classified adherence to the quarantine as the answers “I have stayed at home just going shopping at the supermarket and pharmacy” or “stayed strictly at home, leaving only for health care needs”. All the covariates were pre-selected as confounders.
Statistical proceduresDescriptive data were analyzed using prevalence estimates and 95% confidence intervals (CIs). We used univariate analysis to investigate the association of changes in physical activity and sedentary behaviors during the pandemic with back pain. Subsequently, we ran a multivariate analysis adjusted for the pre-selected confounders using a binary logistic model. The outcomes were (1) incidence of back pain and (2) increased back pain. The explanatory variables were (1) patterns of changes in physical activity, (2) patterns of changes in TV-viewing, and (3) patterns of changes in computer/tablet use. The pre-selected confounders were: sex, age group, highest academic achievement, working status during the quarantine, skin color, and adherence to the quarantine. All statistical procedures were conducted using sampling weights (survey command) in Stata 15.1.
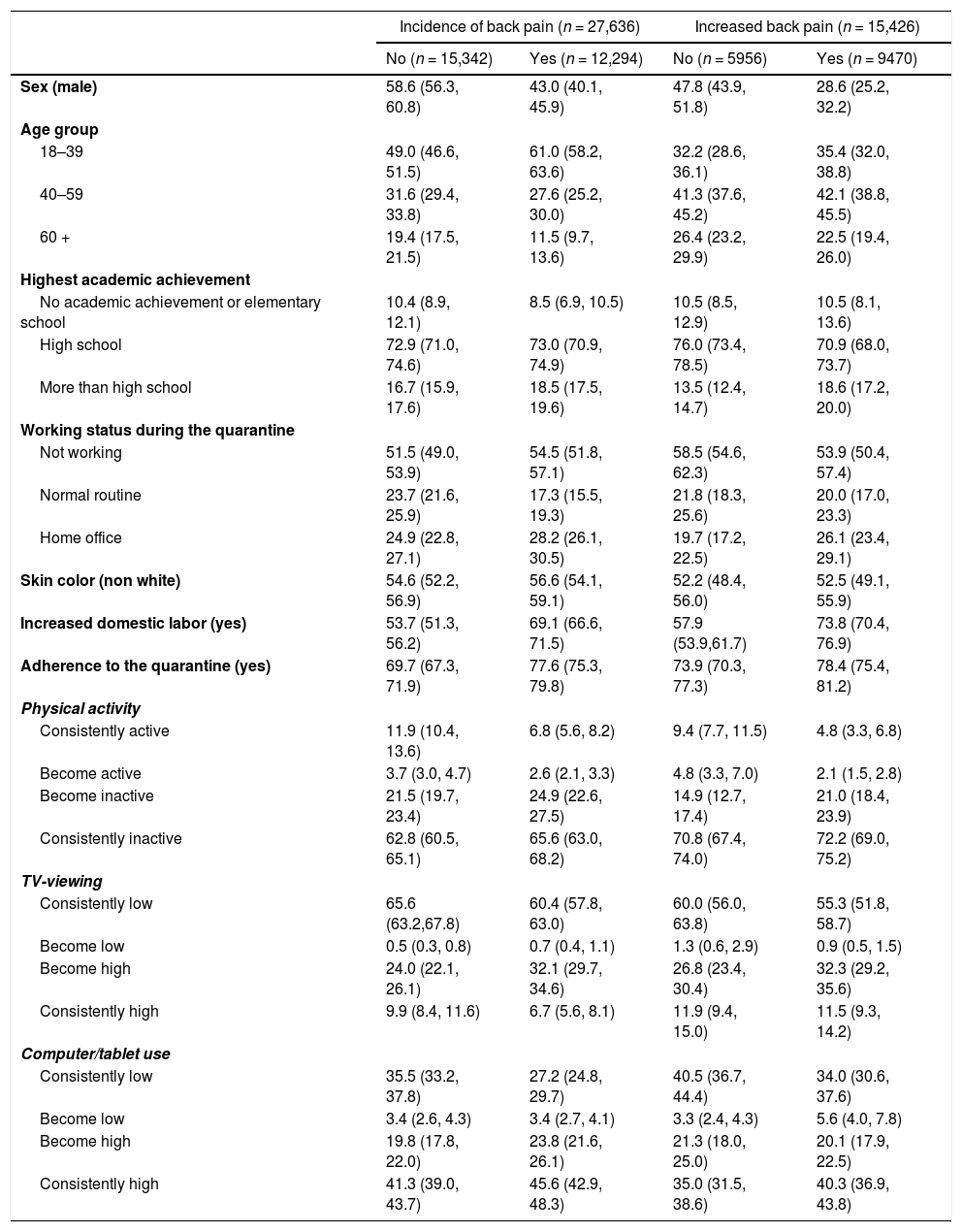
ResultsParticipants and descriptive dataAfter exclusion for incomplete information, 43,062 participants composed the final sample. Around 65% (n = 27,636) of the participants did not report previous back pain, but 44% (n = 12,294) of them started to present this health problem during the pandemic. Among those who already had back pain before the pandemic, 61% (n = 9470) reported increases in back pain. The general characteristics of these groups are presented in Table 1. Women represented the majority for the incidence and worsening of back pain. The younger age group and those who reported adherence to the quarantine were more represented among the incidence of back pain group, while higher educational status and working at home office were more represented among those who reported increases in back pain. Consistently active individuals were the least represented among both incidence and increased back pain groups, while those who reported ≤ 4 h/d of TV-viewing and ≤ 4 h/d computer/tablet use before and during the pandemic were the least represented among the incidence of back pain group. Univariate and multivariate models for the associations between pattern of movement behaviors and back pain (incidence and increase) are presented in Table 2.
Characteristics of the sample.
Note. Values are presented as weighted frequencies and 95% confidence intervals.
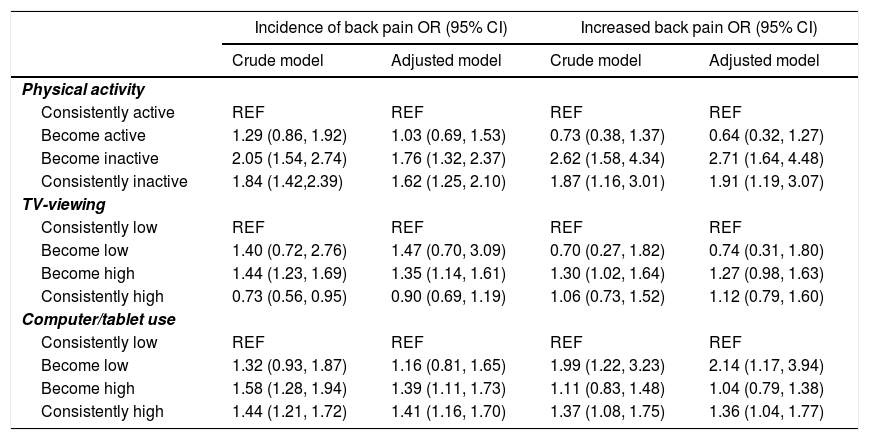
Association of changes in physical activity, TV-viewing, and computer/tablet use, and back pain (incidence and increase).
Note. Adjusted model: adjusted for sex, age group, highest academic achievement, working status during the quarantine, skin color, increased domestic labor, and adherence to the quarantine. OR, odds ratio. CI, confidence interval. REF, reference category.
The results showed a direct association between being consistently inactive (OR = 1.62, 95% CI: 1.25, 2.10) or became inactive during the quarantine (OR = 1.76, 95% CI: 1.32, 2.37) with the occurrence of back pain, when compared to the consistently active group. In the same way, there was a direct association between being consistently inactive (OR = 1.91, 95% CI: 1.19, 3.07) or became inactive during the quarantine (OR = 2.71, 95% CI: 1.64, 4.48) and the increase in back pain, when compared to the consistently active group.
Patterns of changes in TV-viewing timeThe results showed that there was a direct association between high TV-viewing time during the quarantine (OR = 1.35, 95% CI: 1.14, 1.61) and the occurrence of back pain when compared to the group of consistently low TV-viewing time.
Patterns of changes in computer/tablet use timeThe results showed that there was a direct association between high computer/tablet use time (OR = 1.39, 95% CI: 1.11, 1.73) or consistently high computer/tablet use time during the quarantine (OR = 1.41, 95% CI: 1.16, 1.70) and the occurrence of back pain, when compared to the group of consistently low computer/tablet use time. In the same way, there was a direct association between low to high computer/tablet use time (OR = 2.14, 95% CI: 1.17, 3.94) or consistently high computer/tablet use time during the quarantine (OR = 1.36, 95% CI: 1.04, 1.77) and the increase in back pain when compared to the group of consistently low computer/tablet use time.
DiscussionWe investigated associations between patterns of movement behaviors and back pain during the first phase of the COVID-19 pandemic quarantine among Brazilian adults. Our main findings were that physical inactivity and elevated sedentary behaviors due to the COVID-19 pandemic quarantine increased the likelihood of the incidence and worsening symptoms of back pain among those who already had back pain before the pandemic. In this sense, consistently inactive people and those who maintained high computer/tablet use were more affected during the quarantine. Among people who reported high TV-viewing, participants who changed to presenting high TV-viewing were the most affected.
Limitations of the current study include the use of online questionnaires for data assessment, which can imply memory bias (in the case of retrospective information). However, in quarantine times, interviews, or even the use of device-based methods to assess movement behaviors are not possible. The online administration of the questionnaires can also limit access to less affluent people, especially in a middle-income country context. The interpretations of the current findings should consider the opinion of the participants about their back pain being caused by changes in their habitual activities, because questions about changes in back pain during the pandemic included: "back or spinal pain due to the changes in habitual activities". In addition, more details about household activities during quarantine (e.g. carrying weight, squatting, or kneeling) would help in understanding the complex relationship between movement behaviors and back pain in these times. Finally, this is a cross-sectional survey, with limitations in attributing causality. However, this study includes more than 43,000 people from one of the countries most affected by the COVID-19 pandemic, which provides valuable insights into how movement behaviors are associated and can be used to prevent back pain during these difficult times. To the best of our knowledge, this is the first national survey linking changes in movement behaviors due to the COVID-19 pandemic quarantine and back pain.
Other studies from the National Health Survey point out the magnitude of low back pain in the Brazilian population (∼18%).12,18 Although there is no consensus about the overall effect of physical activity on back pain,19 consistent evidence suggests that, especially, leisure-time physical activity at moderate intensities reduces the risk of back pain.6,20 In Brazil, physical exercise/physical therapy was the second most commonly used intervention to treat back pain.4
During the quarantine periods, people are encouraged to stay at home, limiting opportunities to be active (≥150 min/week of moderate physical activity). In this sense, our findings indicate that consistently inactive people and especially those who have become inactive during the quarantine are more likely to report back pain incidence and increased symptoms, which corroborates previous findings.21 This result can be at least partially explained by reduced muscle strength, muscle mass, and flexibility associated with physical inactivity,22 which in turn increase the risk of back pain.23 Interestingly, this relatively short period of inactivity (∼1–2 months) is enough to increase the likelihood of worsening back pain, corroborating previous findings on the harmful effects of short periods of inactivity in other biological systems.24,25 Thus, actions to encourage people to be active during quarantine periods should be developed to mitigate the burden of back pain and the consequences. Although some initiatives have been launched during the COVID-19 pandemic to support an active lifestyle,26 such as physical exercises at home, further studies are needed to identify the effectiveness of these actions.27
In addition to the reduced opportunities for physical activity, people are more prone to sedentary behaviors during quarantine periods. Although the association between sedentary behaviors and back pain is less clear and tends to vary according to occupational status,19,28,29 prolonged sitting seems to be detrimental to musculoskeletal symptoms.30 Here, we observed that becoming more sedentary during the COVID-19 pandemic quarantine increases the likelihood of the incidence of back pain, but only increased TV-viewing was associated with worsened back pain. On the other hand, consistent computer/tablet users were more prone to both an incidence of and increased back pain symptoms, which did not occur among the consistently high TV-viewing group. These results reinforce previous evidence showing that not all sedentary behaviors are equal.31,32 In this case, both TV-viewing and computer/tablet use are behaviors generally performed in different environments and for different purposes. This could suggest that the routine of those who already presented high TV-viewing before the pandemic was less affected in comparison with those with consistent computer-tablet use, especially considering adaptations needed to use a computer/tablet during the quarantine, such as the ergonomic environment.
An unexpected result was the increased likelihood of worsening back pain (not incidence) among those who changed to spending <4 h/d in computer/tablet use during the pandemic. We suppose that this represents specific population sub-groups that were overloaded with family activities, which can be associated with prolonged standing time, inadequate posture, and musculoskeletal disorders.19 In addition, reduced computer/tablet use could also be replaced by other types of sedentary behavior, such as more TV-viewing, explaining the higher likelihood of worsened back pain. Given our cross-sectional design, the non-use of the computer and tablet may also have occurred due to the worsening back pain, resulting in the inability to use computers for a long time. This result highlights how the complex composition of daily activities can explain musculoskeletal health. Future studies should consider a wider range of movement behavior information (e.g. type, intensity, duration) with objective measures of the patterns of physical activity and sedentary behaviors (e.g. bouts and breaks).
These findings highlight how patterns and changes in specific movement behaviors due to the COVID-19 quarantine affected musculoskeletal health. Although the reports could represent isolated episodes of back pain, persistent cases could disable people, affecting quality of life and the health systems.2 These results should support policies from Primary Health Care managers, supporting physical activity programs, such as the Health Academy Program,33 as well as supporting the maintenance of family health support teams (NASF), which need to be financed, and expansion of the supply of professionals, such as physical therapists, physical educators, and others, who can act in primary care, minimizing the effects of musculoskeletal diseases, such as back pain, in the post-pandemic period.
ConclusionsPhysical inactivity and elevated sedentary behaviors due to the COVID-19 pandemic quarantine are associated with the incidence and worsening symptoms of back pain among Brazilian adults. These findings reinforce the need to promote active lifestyles during periods of quarantine to mitigate the burden of pandemics on people's health.
André Werneck is supported by the São Paulo Research Foundation (FAPESP) with a PhD scholarship (FAPESP process: 2019/24124-7). Deborah C. Malta (process 308250/2017-6), Marilisa B. A. Barros (process: 303241/2019-5) and Célia L. Szwarcwald are supported by the National Council of Technological and Scientific Development (CNPq), which funded the productivity scholarship. This paper presents an independent research. The views expressed in this publication are those of the authors and not necessarily those of the acknowledged institutions.



