





To analyze the influence of previous aerobic exercise on cardiovascular responses during resistance exercise.
MethodsThis is a crossover observational study. The sample included 19 normotensive men aged between 19 and 39 years. Subjects performed two experimental sessions in random order: resistance exercise (R: three sets of knee extension exercises with 40% of one repetition maximum) and aerobic exercise+resistance exercise (A+R: 30min of aerobic exercise followed by R protocol). In both sessions, blood pressure (BP) and heart rate were monitored beat-by-beat by finger photoplethysmography.
ResultsAfter aerobic exercise in the A+R session, there was a maintenance of systolic BP −2 (95% CI: −6; 2) mmHg (P=0.35), diastolic 1 (95% CI: −2; 5) mmHg (P=0.40) and mean BP 0 (95% CI: −4; 4) mmHg (P=0.91) and an increase in heart rate 11 (95% CI: 7; 16)bpm (P<0.001). Diastolic and mean BP increased and peak heart rate was higher during resistance exercise in the A+R session compared to the R session. Differences between sessions: diastolic BP 7 (95% CI: 2; 12) mmHg (P=0.03); mean BP 8 (95% CI: 2; 13) mmHg (P=0.05); and peak heart rate 18 (95% CI: 13; 23)bpm (P<0.001). The increases in systolic BP during resistance exercise were similar between sessions 16 (95% CI: 6; 26) mmHg (P=0.43).
ConclusionAerobic exercise before resistance exercise increased diastolic and mean BP and heart rate. However, due to the sample size of 19 individuals, the results must be interpreted with caution.
Resistance exercises increase strength, muscle mass and power, functional capacity, and quality of life,1–3 therefore they have been consistently recommended for individuals with and without the presence of cardiovascular diseases.4–6 However, during resistance exercise, there are abrupt increases in heart rate,7–11 cardiac output,10 and blood pressure (BP),7–10,12–14 which have been a concern.5,6 Thus, strategies to attenuate the cardiovascular responses during resistance exercise have been sought.
A single bout of maximal dynamic exercise has been shown to attenuate the BP response to mental stress.15,16 These responses were attributed to an increase in vasodilation, decreases in sympathetic outflow from the central nervous system, and post-exercise hypotension observed after aerobic exercise.17 Therefore, it is plausible that cardiovascular responses during resistance exercise could also be attenuated after aerobic exercise.
The aim of this study was to analyze the influence of previous aerobic exercise on cardiovascular responses during resistance exercise. We hypothesized that previous aerobic exercise would attenuate the increase in BP during resistance exercise.
MethodsSubjectsConsidering a moderate effect size between sessions (0.05), power of 80%, and an alpha error of 0.05, the sample size estimated for this condition was 13 subjects. Nineteen healthy subjects were recruited from Universidade de Pernambuco and Universidade Estadual de Londrina. The inclusion criteria were: (a) male; (b) aged between 18 and 45 years; (c) without musculoskeletal injuries that could be aggravated by physical exercise; (d) systolic and diastolic BP at rest ≤140/90mmHg, respectively; (e) non-obese (BMI<30); (f) insufficient physical activity (not engaged in regular physical activities for more than 150min a week); and (g) not using medication that influences the cardiovascular variables.
All patients who volunteered to participate were informed of the benefits and risks of the investigation before signing the informed consent statement. This study was approved by the Ethics Committee of Universidade de Pernambuco, Recife, PE, Brazil (protocol: CAAE 15505613.0.0000.5207/UPE).
ProceduresSubjects performed the 1-RM test to evaluate the maximum strength in the knee extension exercise.18 After an interval of at least 72hours, subjects underwent two sessions in random order: resistance exercise (R) or aerobic exercise followed by resistance exercise (A+R). All subjects performed both sessions in a crossover design, in simple random order generated by a computer software.19 An interval of at least 72h was observed between sessions. Subjects were blinded to which session they were going to perform until the beginning of the exercise.
The design of the study is described in Fig. 1. The sessions started between 8am and 9am. After arriving at the laboratory, subjects were referred to the hemodynamic evaluation room (with a controlled temperature between 20 and 24°C) and remained resting in the seated position on the knee extension equipment for 10min, after which cardiovascular parameters were recorded for 5min.
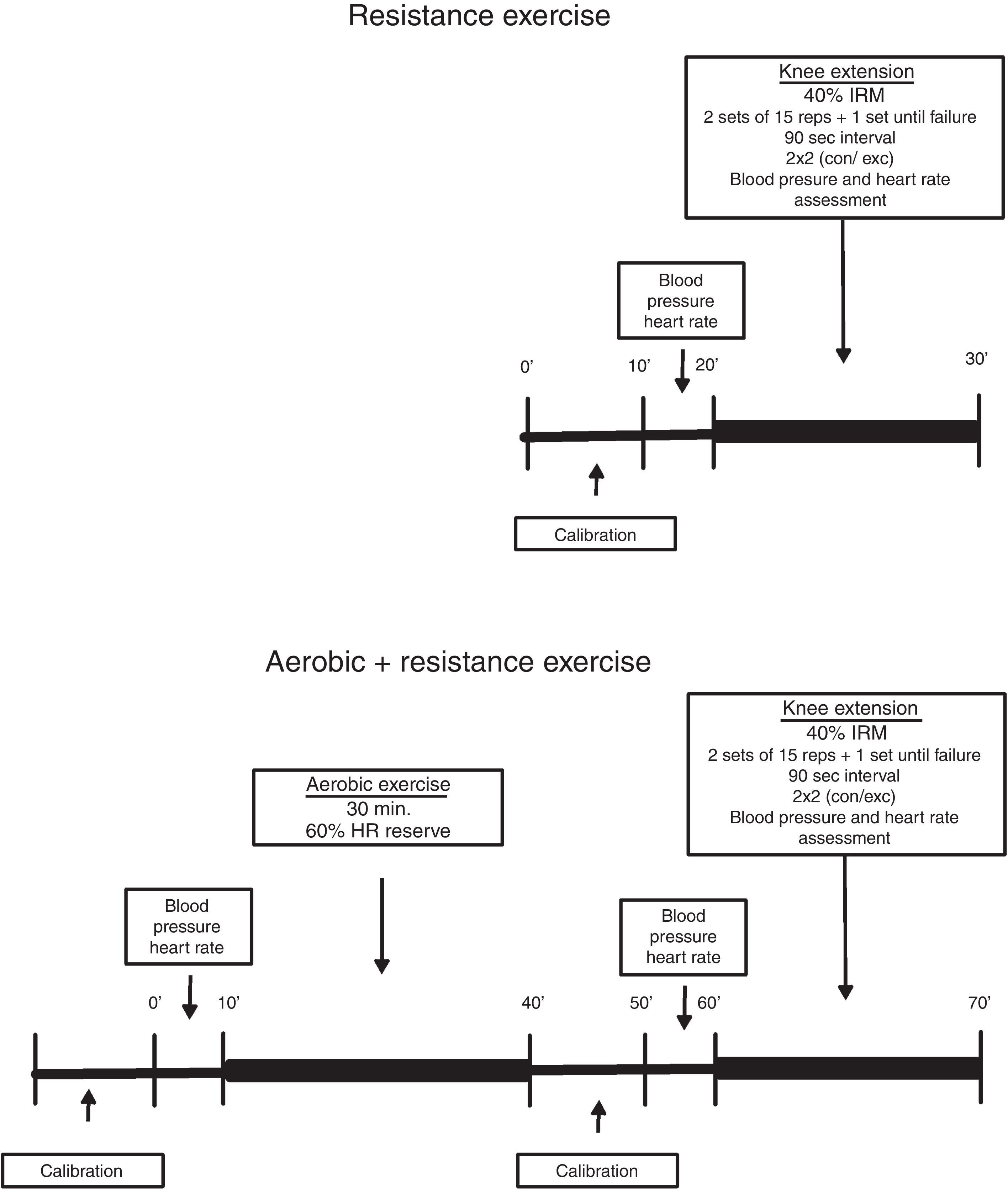
After that, subjects performed the experimental session (A+R or R). The R session consisted of three sets of knee extension exercises with 40% 1-RM, with a 90-s interval between sets. In the first two sets, 15 repetitions were performed, while in the last set repetitions were performed until failure. This intensity was employed to avoid a complete mechanical compression of the arteries, commonly observed at higher intensities, and because a previous study observed higher systolic BP responses during 40% of 1-RM compared to 80% of 1-RM until concentric failure.12 Furthermore this intensity has been prescribed to cardiac patients because it is demonstrated to be safe.20
The A+R session began with 30min of aerobic exercise on a treadmill (T200 Cosmed, Rome, Italy) at 60% of heart rate reserve. After that, subjects returned to the seated position, on the knee extension equipment, and performed the same resistance exercise protocol employed in the R session. The transition between aerobic and resistance exercises lasted approximately 10min.
OutcomesIn both sessions, BP and heart rate were obtained beat-by-beat on the middle finger of the left hand using an automatic photoplethysmography monitor (Finometer, Finapress Medical System, Netherlands). Height correction was used and a brachial cuff was placed on the upper arm to adjust pressure differences between heart and hand. Calibration was performed following the manufacturer's instructions. The exercise cadence was controlled by a metronome (Dolphin Metro-Tuner DP30, Germany), with 2s for concentric and 2s for eccentric phases. Subjects were instructed to avoid the Valsalva maneuver while performing the exercise.
For analysis, the average of the highest five consecutive beats was used to determine the peak values, while the average of the lowest five consecutive beats was used to determine the lower interval values. Changes in cardiovascular parameters during exercise (Δ) were defined as the peak value during exercise minus the prediction interval value. For the pre-exercise values, the average of 5min before the resistance exercise was considered.
Statistical analysisData analysis was performed in Statistical Package for the Social Sciences (SPSS) version 16.0. Normality and homogeneity were confirmed with Shapiro–Wilk and Levene tests, respectively. Data are presented in mean and 95% confidence intervals.
The Student's t-test for dependent samples was used to compare baseline variables between sessions. The changes in blood pressure during the set and intervals were analyzed employing two-way ANOVA for repeated measures (factors: sessions and sets). The Newman–Keuls post hoc test was used when necessary. The significance level was set at P<0.05.
ResultsThe characteristics of the sample are presented in Table 1. All subjects were healthy and without pre-hypertension, hypertension, or history of health issues. No subjects were on medication.
Table 2 presents the cardiovascular variables before and after aerobic exercise in the A+R session. Except for the heart rate, which increased (P<0.001), all other variables remained similar after aerobic exercise. There were no differences between sessions in systolic, diastolic, and mean BP before the onset of resistance exercise (P>0.050).
Cardiovascular responses before and after aerobic exercise in the A+R session, n=19.
| Pre | Post | Δ | P | |
|---|---|---|---|---|
| Systolic blood pressure, mmHg | 107 (103; 111) | 105 (100; 111) | −2 (−6; 2) | 0.35 |
| Diastolic blood pressure, mmHg | 65 (62; 68) | 66 (62; 71) | 1 (−2; 5) | 0.40 |
| Mean blood pressure, mmHg | 81 (78; 84) | 81 (77; 85) | 0 (−4; 4) | 0.91 |
| Heart rate, bpm | 65 (62; 67) | 76 (73; 80)a | 11 (7; 16) | <0.001 |
Data presented as mean (95% confidence interval). Δ: Post−Pre difference values.
Fig. 2 presents the changes in cardiovascular response during resistance exercise in both sessions. Systolic, diastolic, and mean BP progressively increased throughout the sets, achieving the highest values in the third set. There was time vs. session interaction for diastolic and mean BP (P<0.050). The A+R session presented greater changes in diastolic BP for the first set 47 (95% CI 39; 64) vs. 54 (47; 60) mmHg (P=0.003) and in mean BP for the first set 54 (95% CI 46; 62) vs. 62 (95% CI 57; 67) mmHg (P=0.008) and for the second set 63 (95% CI 57; 69) vs. 70 (95% CI 64; 76) mmHg (P=0.02), compared to the R session. However, the changes for the third set were similar in both sessions. The heart rate changes were similar for all sets in both sessions. Consequently, the peak was higher in the A+R 147 (95% CI 138; 157)bpm compared to the R session 137 (95% CI 127; 146)bpm (P<0.001).
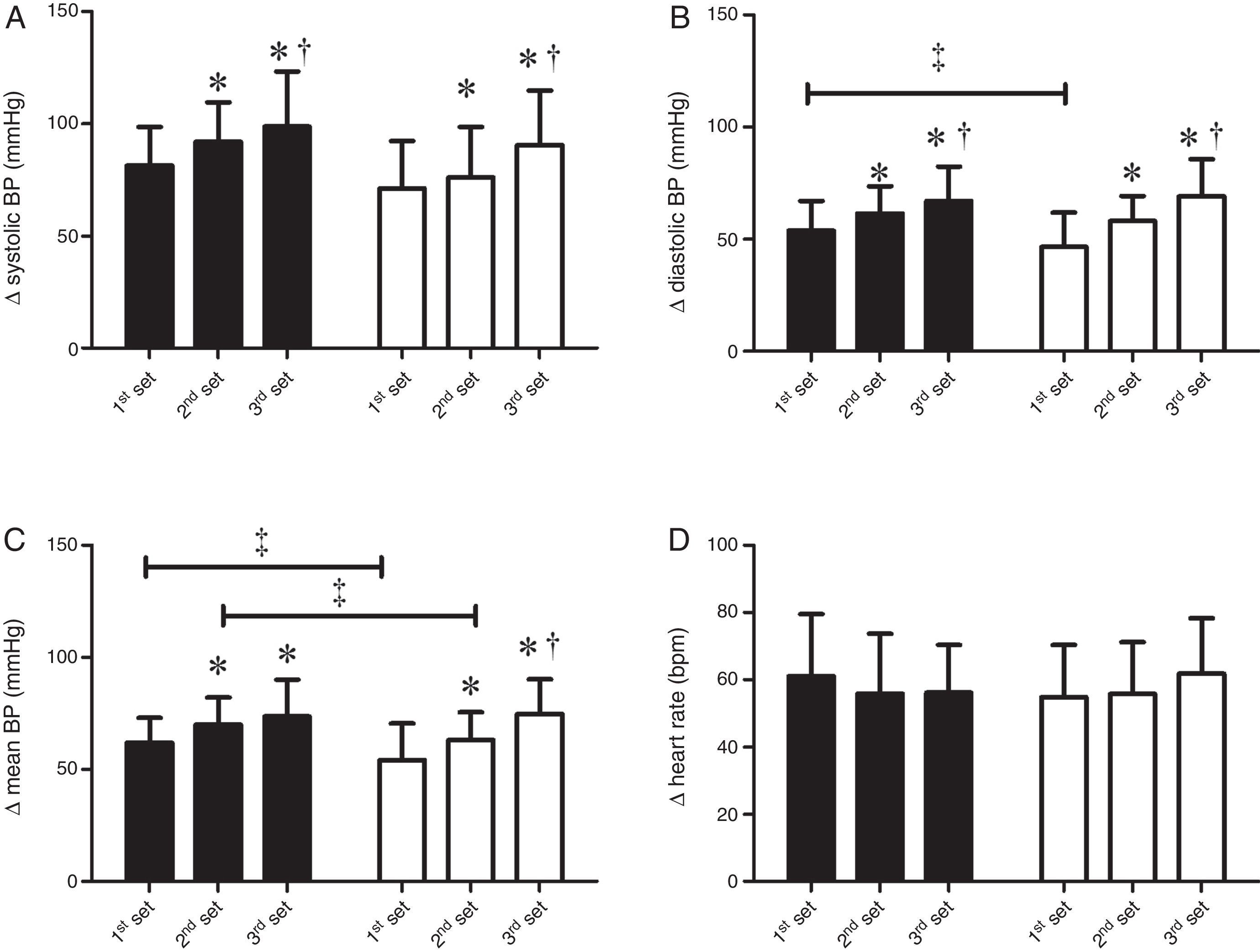
Table 3 presents the cardiovascular parameters during the rest interval between sets. Systolic and diastolic BP were higher during the first and second rest intervals compared to pre-exercise values in both sessions. Heart rate progressively increased from the first to the second rest intervals compared to pre-exercise values in both sessions; however, A+R was higher in pre-exercise compared to the R session. The mean BP in rest intervals was similar to pre-exercise values in both sessions.
Cardiovascular parameters during the intervals between resistance exercise sets in both experimental sessions, n=19.
| Pre-resistance exercise | First interval | Second interval | Time effect | Interaction effect | |
|---|---|---|---|---|---|
| Systolic blood pressure, mmHg | |||||
| Resistance exercise | 107 (103; 111) | 114 (108; 121)a | 118 (111; 124)a | <0.01 | 0.10 |
| Aerobic+resistance exercise | 105 (100; 111) | 109 (104; 115)a | 109 (101; 118)a | ||
| Between group difference | 2 (−1; 5) | 5 (1; 9) | 9 (1; 16) | ||
| Diastolic blood pressure, mmHg | |||||
| Resistance exercise | 63 (60; 66) | 60 (56; 63)a | 61 (56; 65)a | 0.04 | 0.47 |
| Aerobic+resistance exercise | 66 (62; 71) | 64 (61; 68)a | 64 (60; 68)a | ||
| Between-group difference | −3 (−6; 0) | −4 (−8; −2) | −3 (−7; 0) | ||
| Mean blood pressure, mmHg | |||||
| Resistance exercise | 80 (77; 83) | 80 (76; 84) | 81 (76; 86) | 0.93 | 0.62 |
| Aerobic+resistance exercise | 81 (77; 85) | 81 (77; 86) | 81 (75; 86) | ||
| Between-group difference | −1 (−4; 2) | −1 (−5; 2) | 0 (−5; 6) | ||
| Heart rate, bpm | |||||
| Resistance exercise | 64 (62; 67)c | 71 (67; 75)a | 75 (69; 80)a,b | <0.01 | 0.27 |
| Aerobic+resistance exercise | 76 (73; 80) | 84 (79; 90)a | 91 (82; 100)a,b | ||
| Between-group difference | −12; (−16; −8) | −13 (−18; −9) | −16 (−23; −11) | ||
Data presented as mean (95% confidence interval).
The main results of this study were: (i) after aerobic exercise, there was maintenance of BP and an increase in heart rate; (ii) there were greater increases in diastolic and mean BP and higher peak heart rate values in the A+R session compared to the R session; (iii) the cardiovascular variables during the interval between sets were similar between sessions.
The results of the present study indicated maintenance of BP after aerobic exercise, which is contrary to several studies that reported significant decreases in BP after a single bout of aerobic exercise.21,22 Although post-exercise hypotension has been observed in normotensive and hypertensive subjects21–23 and in patients with cardiovascular diseases,24,25 a significant correlation has been observed between the resting BP levels and the magnitude of post-exercise hypotension.26 Thus, the non-occurrence of post-exercise hypotension in this study was probably affected by the lower resting systolic BP levels (<110mmHg on average). Another possible explanation is that post-exercise hypotension is commonly observed after 30min of exercise,23 while in the present study the time between the end of the aerobic exercise and the onset of R was approximately 15min.
In both sessions, there were progressive increases in BP across the sets, which is partly explained by the non-return of BP to resting values during recovery, leading to the onset of a new set with higher BP values. In a previous study, Nery et al.12 found that a 90-s interval was enough for systolic BP to return to the resting values during knee extension exercises with 80% of 1-RM. Thus, the time required for the BP to return to resting values is intensity/volume dependent.27 This is an important variable because the increases in BP across the sets were probably caused by the insufficient recovery that may have led to the accumulation of metabolites increasing fatigue over the sets.
The changes in diastolic and mean BP during resistance exercises in the first and second sets were higher in the A+R session compared to the R session. Although the A+R session was longer in duration than the R session, we do not believe that this is the only factor influencing BP response given that, before resistance exercises, BP was similar between both sessions. The residual fatigue of aerobic exercise performed prior to resistance exercise is a potential mechanism of these responses. In fact, the fatigue generated by previous aerobic exercise increases the recruitment of motor units and the involvement of accessory muscles.28 Furthermore, greater fatigue resulting from aerobic exercise may lead to an increased accumulation of metabolites, stimulating chemoreceptors and thus increasing peripheral sympathetic activity.29 However, it is important to highlight that, although the change in BP was 10% greater in the A+R, data should be interpreted with caution, given that a ‘threshold risk’ for BP has not been established in the literature.
In this study, the changes in heart rate were similar between sets in both sessions. Consequently, higher peak heart rate values were observed when aerobic exercise was performed before resistance exercise (A+R session) in comparison with the R session. After aerobic exercise, the autonomic cardiovascular system is changed compared to resting values.30–32 Although a vagal reactivation occurs quickly after the end of aerobic exercise, sympathetic activity remains increased until 25–30min after moderate intensity aerobic exercise.33,34 Thus, since the resistance exercise was performed 15min after aerobic exercise in the A+R session, the increased sympathetic activity at the onset of the resistance exercise may contribute to the greater increase in heart rate in that session.
In practical terms, the results of the present study indicated that the peak systolic and diastolic BP during resistance exercise were 208±32 and 131±15mmHg (data not shown), independently of the held session. These values are lower but close to the values found in the study by Nery et al.12 with the same exercise (knee extension) and intensity (40% RM), in normotensive and hypertensive individuals. On the other hand, the response of the BP of our study was much lower than that found by MacDougall et al.9, who recorded BP during resistance exercise in resistance exercise practitioners who carried out the leg press exercise sets with high intensity until exhaustion. An analysis of all of the study results seems to indicate that, when the resistance exercise is prescribed with moderate loads in exercise with less muscle mass12,14, the BP peak values obtained are less severe than those previously described in the literature.9,35,36
The second practical message is that the performance of aerobic exercise before resistance exercise does not minimize the increase in BP during resistance exercise, but increases diastolic and mean BP responses during the first and second sets and maintains a peak heart rate higher than R only during the resistance exercise protocol. Thus, aerobic exercise cannot be used to minimize the cardiovascular responses during resistance exercise in normotensive subjects.
Some limitations should be emphasized in this study. The sample size is small; therefore, the results of this study must be interpreted with caution. The transition time between aerobic exercise and resistance exercise in the A+R session was kept as short as possible in order to simulate practical conditions. Consequently, a longer transition time may have caused different results that should be investigated in future. In the present study, the sample included healthy male normotensive individuals to elucidate the phenomenon per se, without the influence of disease and medication. Despite concerns regarding the extrapolation of the results to hypertensive populations, a previous study showed that BP responses during a resistance exercise protocol are similar between normotensive and hypertensive subjects.12 Another limitation is that, although finger-occlusion photoplethysmography has been validated for assessment of cardiovascular responses during resistance exercise,13 slight overestimation of systolic BP and underestimation of diastolic BP has been reported. In this sense, we presented change values (absolute deltas) of cardiovascular responses during resistance exercise, as recommended.13 The physical activity status was not measured directly; therefore, we assume that there would be differences in exercise response in an individual who does not exercise versus an individual who exercises 150min per week.
In conclusion, the results of this study indicated that the performance of aerobic exercise before resistance exercise promoted greater increases in diastolic and mean BP and generated higher peak heart rate. Thus, we do not recommend aerobic exercise prior to resistance exercise in order to minimize increases in BP and heart work during resistance exercise.
Conflicts of interestThe author declares no conflicts of interest.
We wish to thank Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), and Fundação de Amparo à Ciência e Tecnologia de Pernambuco (FACEPE).



