


Older adults have a high probability of experiencing falls during activities of daily living, which can lead to fear of falling, alterations in gait patterns, decreased mobility, reduced social interactions, and limited ability to perform various tasks. Previous studies examining gait in the presence of perturbations have identified and analyzed several protective gait strategies aimed at preventing falls. However, there is a lack of standardized terminology and definitions for these strategies, hindering comparison and collaborative progress among researchers and professionals.
ObjectiveTo unify definitions of compensatory protective step strategies and establish a standardized terminology.
MethodsThis study adapted the Conducting and Reporting of Delphi Studies (CREDES) guidelines and followed a chronological sequence: 1) Preliminary phase: A literature review and both quantitative (three dimensions: relevance, wording, and identification, assessed using a Likert-type scale (1 to 5) and qualitative (an open-ended question) assessment were conducted; 2) Exploratory phase: Expert panel selection (n = 14) and the e-Delphi study were conducted; and 3) Final phase: Expert opinions were collected and analyzed. Content validity was assessed using Aiken’s V coefficient.
ResultsThe results demonstrated high levels of validity (V ≥ 0.68) for all definitions, with none being eliminated based on Aiken's V critical value.
ConclusionA precise definition was developed for each of the 14 compensatory protective step strategies (13 identified in the scoping review and one added by the expert panel). In total, the number of definitions was reduced from 61 to 14, with one definition for each of the compensatory protective step strategies identified.
Falls consistently rank as the second leading cause of unintentional injury-related deaths globally. Approximately 684,000 individuals die from fatal falls, and an estimated 37.3 million non-fatal falls requiring medical treatment occur annually.1 Falls contribute to increased hospitalizations and early admissions to rehabilitation centers, placing a significant economic burden on healthcare systems.2,3 Additionally, falls can adversely affect the daily living activities of older adults, reducing their quality of life, fitness, psychological and social well-being, and independence.4 Furthermore, adults older than 60 years-old have the highest risk of falling and a high probability of suffering a fall during daily activities5 because of declines in cognitive, physical, and sensory functions.1
Researchers have employed perturbation methods in controlled environments to investigate balance recovery during gait. Techniques such as waist-pull, mobile platforms,6,7 slippery floor surfaces,8 release systems,9,10 and robotic devices11 have been employed to elicit protective step strategies to prevent falls.12,13 Despite this progress, inconsistencies in the terminology used across studies have made comparisons difficult. For instance, the strategy known as “cross-step” has also been referred to as “unloaded sidesteps”,14 “unloaded crossover step”15,16 or “crossover step”17,18 in some studies.
Melo-Alonso et al.19 addressed this issue by conducting a scoping review that grouped these terms under the broader concept of “compensatory protective step strategies,” offering clear definitions to promote greater consistency in future research. This review revealed a wide range of terms, abbreviations, and definitions for these strategies. Navigating the existing variety of terms and definitions can be complex and frustrating, as some authors provide definitions,19 while others do not, and the available definitions vary significantly in detail and accuracy. To resolve these, researchers need to clearly and precisely define the strategies they intend to investigate.
The Delphi method has been proposed as an effective approach to address this issue and achieve consensus on complex issues.20 This method systematically synthesizes expert opinions to build a cohesive understanding, harnessing the collective expertise of a diverse panel while encouraging independent and unbiased input.20,21 By minimizing the limitations inherent in relying on a single expert’s perspective, the Delphi method is recognized for its cost-effectiveness, ease of implementation, and capacity to incorporate a broad spectrum of expert insights.22 With the rise of the internet, the e-Delphi method has become a popular adaptation of the traditional Delphi process. This approach enhances efficiency by reducing resource use, streamlining communication, and enabling broader expert participation.22
This study employs the e-Delphi method to unify definitions of compensatory protective step strategies, aiming to establish a standardized terminology accessible to physical educators, physical therapists, occupational therapists, physicians, and researchers.23,24 A unified language will strengthen collaboration among professionals focused on fall prevention in at-risk populations, advancing both research and practice in this critical area.
MethodsDesignThe present e-Delphi study employed an adapted version of the Conducting and Reporting of Delphi Studies guidelines (CREDES)25 to structure this descriptive research, integrating both quantitative and qualitative methods.26
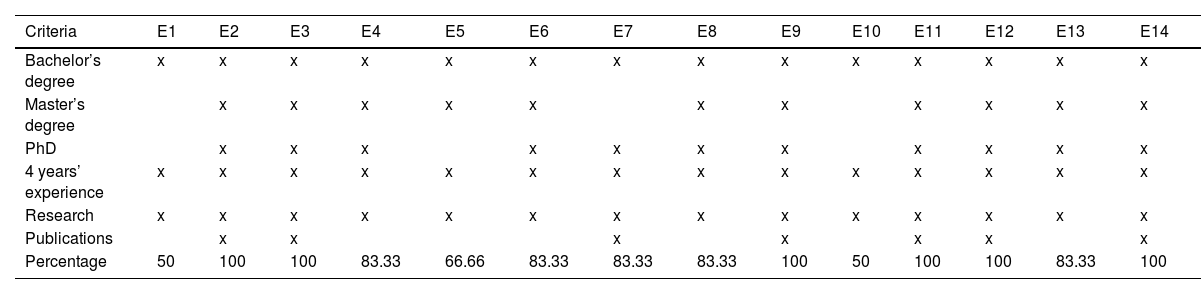
ParticipantsTwo researchers (MMA and SV) established specific inclusion criteria for panel selection. To qualify as an expert, participants were required to meet at least three of the six established inclusion criteria (50 %). The inclusion criteria were: 1) holding a Bachelor’s degree in Physical Activity and Sport Sciences, Physical therapy, Medicine, or Occupational Therapy, 2) possessing a Master’s degree in research, 3) holding a Ph.D., 4) having a minimum of four years of experience on fall risk, postural control, and biomechanics, 5) engaging in research related to fall risk, postural control, and biomechanics (through scientific work, educational roles, or project leadership) and 6) having publications on fall risk, postural control, and biomechanics in older adults. The expert panel was required to complete an online questionnaire to assess compliance with the inclusion criteria. Panel selection was intentional and based on verified research backgrounds in fall risk among older adults.
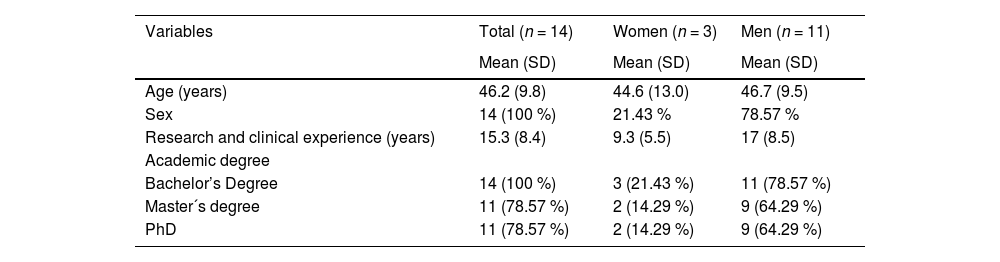
Therefore, a total of 16 experts were invited to participate in the study via institutional email in February 2024. Of these, 14 Spanish experts agreed to collaborate, resulting in an 87.5 % participation rate. Among the 14 experts, 11 were men (78.57 %) and three were women (21.43 %), see Table 1.
Characteristics of the expert panel.
SD, standard deviation.
Eleven experts held a Bachelor’s degree in Physical Activity and Sport Science (78.57 %), while the remaining panel members held a Double Bachelor’s degree in Physical therapy and Sport Science (7.14 %), Medicine (7.14 %), or Occupational therapy (7.14 %) (Table 2).
Inclusion criteria complied with by the experts.
E, expert.
Literature review: The coordinating group conducted a search for the most recent studies on the topic. In this regard, a previous scoping review conducted by Melo-Alonso et al.19 compiled the compensatory protective step strategies as well as their definition. The compensatory protective step strategies and definition compiled in this review were used in the present article. Thus, the first step of the CREDES was omitted because the scoping review article was conducted by the same research group as the current article.
Questionnaire design: First, a formal introduction letter was prepared to present the research group and outline the study's objectives. Second, an instruction letter was developed to inform participants about the study process, including a summary of all strategies and definitions compiled by Melo-Alonso et al.19 Third, an initial draft was created using Google Forms, containing one definition for each strategy identified in the scoping review, totaling 14 strategies.19 These definitions were formulated and translated by the coordinating group. To ensure linguistic and conceptual accuracy, the definitions underwent two forward and two backward translations, following the recommendations of Beaton.27 Finally, in the Google Form, each definition was accompanied by a question to assess its relevance, wording, and clarity. Additionally, an open-ended question was included to allow experts to provide qualitative feedback on any of the three evaluation criteria.
Exploratory phaseExpert panel: The coordinating group selected the expert panel based on inclusion and exclusion criteria. Once the panel was formed, a formal letter and study instructions were sent to the experts via institutional email. e-Delphi Study: The instructions outlined the study's aim (to validate the proposed definitions of the compensatory protective step strategies), the estimated time commitment, and the link to round 1. In this round, experts were asked to quantitatively assess the relevance, wording, and clarity of the definitions using a Likert scale (1 to 5) and provide qualitative feedback for improvement. At the end of round 1, the evaluations from the expert panel were collected and analyzed. Definitions and strategies that received optimal scores were retained, while those with acceptable content validity scores were revised. These revised definitions were then returned to the experts for further quantitative and qualitative assessment (Fig. 1) together with a summary report of round 1. The experts panel had one week to individually answer the Google Form questionnaire sent to them by the coordinating group; the experts responded twice to a questionnaire (2 rounds). Between each round, the experts had a week’s rest.
Final phase
Documentation: The coordinating group collected and analyzed the expert evaluations from Round 2. The expert panel was sent a report with the quantitative and qualitative evaluations obtained in the final round. Additionally, a final document containing the definitions was provided. The study was conducted from February 3 to March 31, 2024.
Content validityContent validity refers to the extent to which the selected concept adequately represents the concept being measured or observed.28 This study employed the Delphi method to establish an optimal level of consensus for content validity.22 The expert panel conducted both quantitative and qualitative evaluations. The qualitative evaluation consisted of an open-ended question, allowing experts to suggest improvements to the proposed definitions. The quantitative evaluation involved three dimensions, each assessed using a Likert-type scale (1 to 5) for each definition proposed by the coordinating group:
a). Degree of relevance: This dimension assessed the importance of each definition and strategy, determining whether it was essential and should remain in the compensatory protective step strategies group. For example, a strategy with limited information about the movement would receive a low rating and would not be retained.
b). Degree of wording: This dimension evaluated the clarity, conciseness, and overall quality of the wording used in the definitions. Experts rated how well the definitions were drafted. For instance, a straightforward and easy to understand definition would score higher, while a vague or overly complex definition would receive a lower rating. In this dimension, clarity and conciseness were integral components.
c). Degree identification: This dimension focused on whether the definitions accurately represented the type of compensatory protective step strategies to be observed. For example, a definition that aligns well with established strategies would be rated high. Accurate identification of the core elements of the strategies was essential to ensure a comprehensive understanding.
Data extracted from the Google Forms questionnaires were organized using Microsoft Excel 2019 (Microsoft® Corp., Redmond, USA). Also, Microsoft Excel 2019 software (Microsoft® Corp., Redmond, USA) was used to calculate and analyze the Aiken V coefficient and its confidence intervals.
Aiken's V coefficient was used to analyze the content validity of the definitions of the compensatory protective step strategies evaluated by the expert panel. This Aiken’s V coefficient is an index that quantifies the content validity of each item according to the opinion of an experts panels.29 Aiken´s V coefficient ranges between 0 and 1, the latter showing high content validity,29 indicating high agreement between experts on the content evaluated. The Aiken’s V coefficient calculation lets us know which items should be eliminated, modified, or accepted. The following equation modified by Penfield and Giacobbi30 was used to calculate Aiken´s V coefficient:
Where X¯ represents the sample mean of the judges’ rating, l represents the lowest possible rating and k represents the range of possible values of the rating scale used. In this case, l=1 and k=5−1=4 for Likert scale from 1 to 5.
To establish the criteria for removing, modification, and acceptance, the table elaborated by Aiken was used to obtain the exact critical value of V for 2 to 7 rating categories (c) and 2 to 25 items (m) or rater (n). A confidence level of 95 % was considered to obtain the cut-off point for the eliminations, modification, or acceptance of the items, resulting in a value of 0.68. The confidence level of 99 % was considered for acceptance and not modification of the wording, relevance, and identifications of items, with a value of 0.73, according to the Aiken table.29 Therefore, items with values below V < 0.68 were eliminated, items with values between V = 0.68 and V = 0.73 were modified, and items with values higher than V > 0.73 were considered optimal (Table 3). The coordinating group did modifications in some items if the experts panel felt that it was necessary to improve the comprehension of wording or identification, although the Aiken´s V coefficient was optimal.
Criteria of elimination, acceptance, or modification.
W, wording; R + I, relevance + identification.
Finally, the lower (L) and upper (U) limits of the 95 and 99 % confidence interval for each Aiken V coefficient were calculated using the following equatio:n30
Where n is the number of experts, k represents the range of possible values of the rating scale used, V is Aiken´s V coefficient, and z corresponds to the confidence interval level applied at 95 or 99 %.Results

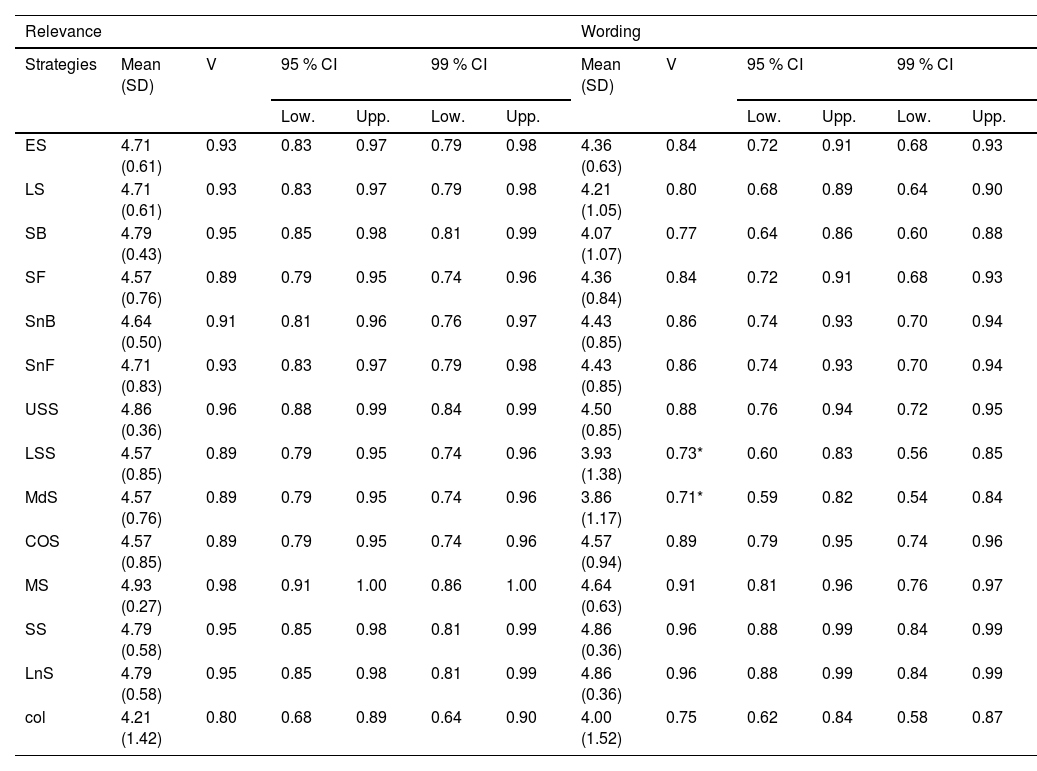
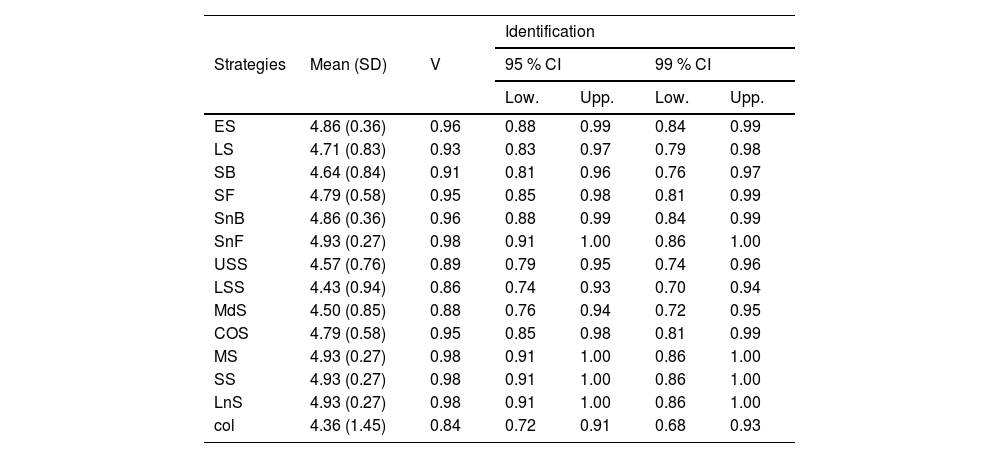
Table 4 and Table 5 show the results from the initial round of evaluation, including the Aiken's V coefficient and corresponding confidence intervals at 95 and 99 % for each compensatory protective step strategy. No items were eliminated, as all obtained values were equal to or greater than 0.68 for relevance. However, two items—specifically the loaded sidestep (LSS) and medial sidestep (MDS)—fell within the range of V = 0.68 to V = 0.73 for the degree of wording. Additionally, two strategies, the lowering strategy (LS) and limb collision (COL), were considered for modification, although they did not fall within the modification range (Table 3). These strategies were revised based on qualitative feedback from the expert panel. Finally, all experts were able to correctly identify all compensatory protective step strategies (Table 4).
Round one for the degree of relevance and wording of the compensatory protective step strategies.
CI, confidence interval; col, limb collision; COS, crossover step; ES, elevation strategy; LnS, long step strategy; Low, lower limit; LS, lowering strategy; LSS, loaded sidestep; MdS, medial sidestep; MS, multiple steps; SB, slip backward step; SD, standard deviation; SF, slip forward step; SnB, single backward step; SnF, single forward step; SS, short step strategy; Upp, upper limit; USS, unloaded sidesteps; V, Aiken´s V; *,V= (0.68–0.73).
Round one for the degree of identification of the compensatory protective step strategies.
CI, confidence interval; col, limb collision; COS, crossover step; ES, elevation strategy; LnS, long step strategy; Low, lower limit; LS, lowering strategy; LSS, loaded sidestep; MdS, medial sidestep; MS, multiple steps; SB, slip backward step; SD, standard deviation; SF, slip forward step; SnB, single backward step; SnF, single forward step; SS, short step strategy; Upp, upper limit; USS, unloaded sidesteps; V, Aiken´s V.
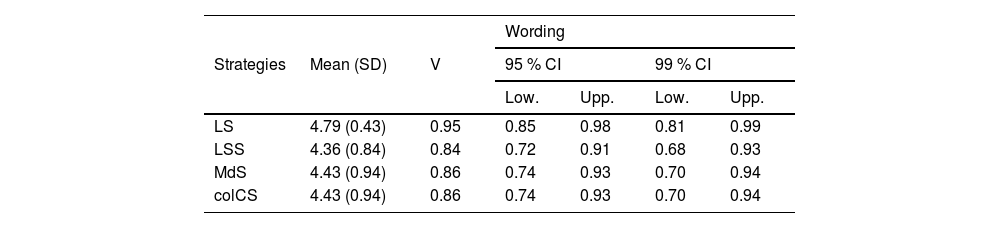
Subsequently, the coordinating group made significant changes by renaming the limb collision strategy (col) to compensatory limb collision step (colCS) as well as adding more description about it. Following these modifications, the expert panel conducted a second round, focusing solely on the wording for the four items from round one that had values below 0.68 or within the range of 0.68 to 0.73. Table 6 shows the values for the degree of wording obtained in the second round. No items were modified, as all values exceeded the modification range (>0.73).
Round two for the degree of wording after modifications of the compensatory protective step strategies.
CI, confidence interval; colCS, compensatory limb collision step; Low, lower limit; LS, lowering strategy; LSS, loaded sidestep; MdS, medial sidestep; SD, standard deviation; Upp, upper limit; V, Aiken´s V.
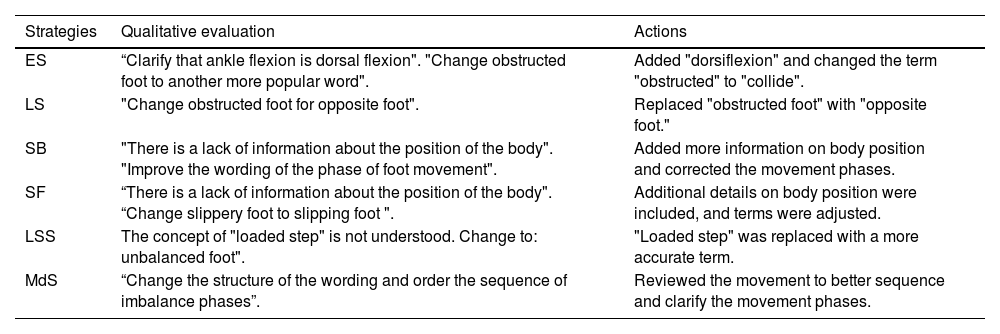
Table 7 presents examples of qualitative feedback provided by the expert panel during both rounds, as well as the actions taken by the coordinating group to refine the definitions of compensatory protective step strategies. The final results of all definitions from this process are detailed in the online Supplementary Material online (Document D1), available in English.
Qualitative evaluation and actions taken to refine definitions of compensatory protective step strategies.
ES, elevation strategy; LS, lowering strategy; LSS, loaded sidestep; MdS, medial sidestep; SB, slip backward step; SF, slip forward step.
Recent years have seen a significant increase in studies focused on fall strategies. However, inconsistencies in the definitions of compensatory protective step strategies across various studies have hindered the establishment of standardized terminology. This study represents a pioneering effort to clarify and refine these definitions using the Delphi method. The goal was to develop a simple and standardized terminology that could be widely adopted across multiple professional domains within the field of falls. To achieve this, a diverse expert panel—comprising sports specialists, physical therapists, occupational therapists, doctors, and researchers—was assembled to ensure comprehensive representation of key stakeholders. The results indicated that the definitions required adjustments to improve clarity and conciseness. Notably, the compensatory protective step strategies that needed substantial revisions were the lowering strategy, loaded sidestep, and medial sidestep (LS, LSS, and MdS). Additionally, the term 'limb collision' (col) was revised to 'limb collision compensatory step' (colCS).
As part of the refinement process, the coordinating group consolidated the strategies into one definition per compensatory step, reducing the total number of definitions from 61 to 13. This simplification significantly improves comprehension, identification, and clarity, as previously, strategies such as USS and COS required reading through multiple definitions—six for each. This advancement enhances the accessibility and efficiency of strategy identification while also reducing the time required for comprehension.
During the first round of the Delphi method, all items exceeded the cut-off point for acceptance (V = 0.68). Although each item met the minimum threshold, several definitions achieved higher validity thresholds: a V > 0.80 for the wording dimension was reached for strategies such as ES, SB, SF, SnB, SnF, USS, COS, MS, SS, and LnS, while a V ≥ 0.85 was reached for relevance and identification dimensions. This suggests that the definitions proposed by the coordinating group aligned well with those from the original scoping review,19 facilitating their recognition and reinforcing their relevance to the category. However, despite achieving high validity in wording, the expert panel recommended additional modifications to further improve clarity. For instance, in descriptions of elevation, terms like “obstructed foot” were replaced with “foot hits” to enhance readability.
In addition, the expert panel suggested that the term limb collision was not an adequate descriptor, considering it more an isolated action that could occur at any point, rather than a compensatory protective stepping strategy. The panel viewed its inclusion in this group as an error, aligning with observations from Melo-Alonso et al.19 scoping review, which noted that limb collisions had merely been reported by other researchers without a clear rationale for classification as a compensatory strategy. While both the author of the scoping review and the expert panel agreed that limb collision does not constitute a distinct strategy for balance recovery, they acknowledged that its occurrence increases the risk of falling. The panel further indicated that the limited literature describing this movement, compared to other strategies, also supports its exclusion from the core group. Nevertheless, previous studies have associated limb collisions with an elevated fall risk, especially when multiple steps are needed to recover balance.31,32 Consequently, the expert panel opposed the complete elimination of the limb collision action, highlighting its relevance due to its increased fall risk, particularly in older adults who use multiple steps to regain balance.32,33 To address these concerns, the experts proposed redefining this as the limb collision compensatory stepping strategy to better capture its implications. This revision would enable the documentation of whether limb collisions influence the primary compensatory strategy employed, as the panel posits that such collisions often lead to a less effective recovery response, ultimately increasing the likelihood of a fall. Given its nature, limb collisions are often seen as unintentional actions occurring when balance recovery fails, thus representing a less adaptive response compared to other compensatory steps intentionally aimed at maintaining stability.
During the study's development, certain terms used in the definitions led to confusion among the expert panel. Specifically, terms like ‘early’ in the descriptions of lowering strategies were replaced with ‘prematurely’ to enhance clarity. Additionally, a more precise description of the position of the legs and feet when encountering an obstacle was provided, resulting in better understanding. Similarly, the term ‘passively loaded leg’ in the definition of the loaded side step (LSS) was replaced with ‘the leg bearing the greater weight’ to eliminate ambiguity. Furthermore, the coordinating group, in collaboration with the expert panel, added supplementary information to most definitions regarding the plane of imbalance onset and its cause (i.e., object interaction, slip, push or pull) leading to a better comprehension. This additional information clarifies the phases involved in fall prevention strategies, resulting in more straightforward and concise definitions that achieved a higher validity score in the second round.
To mitigate heterogeneity in future studies, it is advisable to adopt the definitions provided in this study for identifying strategies, thereby fostering exchanges and discussions among experts in fall-risk assessment and management. This practice enables practitioners to uniformly employ a singular terminology or definition for each specific strategy, facilitating clearer identification of the strategies under examination. By doing so, confusion stemming from the disparate use of definitions, as observed previously, can be minimized. Moreover, establishing a unified terminology may facilitate the development of new clinical assessment tools aimed at identifying or evaluating fall risk based on specific types of compensatory step strategies. Additionally, these standardized definitions could serve as a foundation for designing targeted training programs to enhance body control and decision-making tailored to different types of perturbations. Although this study pretends standardizing the definitions of compensatory protective step strategies in this area, the conclusions should be taken with caution due to the identified heterogeneity and the potential for future refinements in the definitions.
LimitationsThe current study has some limitations. Firstly, the selection of the expert panel was carried out through a convenience sample but contacted people who were knowledgeable about the topic from different disciplines. This approach may have introduced selection bias. However, efforts were made to mitigate this by involving professionals from various health-related disciplines. The interdisciplinary selection of experts (physical therapy, medicine, and occupational therapy experts) allows an interdisciplinary generalized consensus but it could be interesting to check its use in specific disciplines with more experts in each discipline, different cultural languages, or special populations with different locomotion impairments. Secondly, the definitions obtained in this study were developed from the compensatory step strategies contemplated in single research. However, the scoping review facilitated to the expert panel for setting the compensatory step strategies definitions in this study is the most up-to-date and incorporates most of the information regarding the field of study of compensatory step strategies.
ConclusionThis study represents the first comprehensive effort to define and clarify compensatory protective step strategies using the Delphi method. Fourteen strategies are detailed: thirteen identified from a previous scoping review and an additional strategy proposed by the expert panel due to its relevance to fall risk, termed the limb collision compensatory step. This strategy underscores the role of limb collisions in increasing fall risk by potentially impeding balance recovery and heightening the likelihood of a fall. Therefore, a precise definition was developed for each of the 14 strategies, reducing the initial number of 61 definitions, to promote consistency and clarity in future research and practice.
In the framework of the Spanish National R + D + i Plan, the current study was co-funded by the Spanish Ministry of Sciences and Innovation (reference PID2019–107191RB I00/AEI/10.13039/501100011033). The author M.M.-A. was supported by an internship contract (Resolution no 586/2022) from the Spanish Ministry of Sciences and Innovation (reference PID2019-107191RB I00/AEI/10.13039/501100011033) and M.M-A. was supported by a grant from the “Sistema Extremeño de Ciencias, Tecnología e Innovación” by Junta de Extremadura and co-financed by FSE+ of Extremadura (PD23108). This study was also funded by the Research Grant for Groups (GR21176) funded by the Junta de Extremadura (Regional Government of Extremadura) and the European Regional Development Fund (ERDF/FEDER) “a way of doing Europe”. This study was supported by the Biomedical Research Networking Center on Frailty and Healthy Aging (CIBERFES) and FEDER funds from the European Union (CB16/10/00477). The funders played no role in the study design, the data collection, and analysis, the decision to publish, or the preparation of the manuscript.



