
Central sensitisation pain is a predominant mechanism in a proportion of individuals with non-specific chronic low back pain and is associated with poor outcomes. It is proposed that the pre-morbid experiences and contexts may be related to the development of central sensitisation.
ObjectivesThe objective of this study was to explore the pre-morbid experiences and personal characteristics of participants with central sensitisation pain from a non-specific chronic low back pain population.
MethodsThis was a qualitative, exploratory study, using a concurrent nested design within a mixed methods protocol. n=9 participants were recruited purposively based on sensory profiles and trait anxiety-related personality types. Data were collected through semi structured interviews, managed using QSR NVivo 10 software and analysed using theoretical thematic analysis.
ResultsFour themes emerged: developmental learning experiences, personal characteristics, sensitivity and trauma. Reported was lack of confidence, low esteem and a need to please others, physical hyper-sensitivities (smell, light, sound) and emotional sensitivity (anxiety) as well as physical hypo-sensitivity. Participants had also suffered emotional and/or physical trauma. Learning difficulties, sensory sensitivities and trauma are associated with autonomic stress responses, which in turn have been linked to physiological changes seen in central sensitisation pain.
ConclusionCentral sensitisation pain developed in the context of sensory processing differences related to learning difficulties, sensitivities and trauma, and personal characteristics of low confidence and control, in a group of participants with non-specific chronic low back pain. The role of pre-existing sensory processing differences, as a component of altered central nervous system function, in relation to central sensitisation pain warrants further investigation.
Central sensitisation (CS), when it is the predominant pain presentation, contributes towards persistent pain and poor outcomes in many musculoskeletal pain populations, such as whiplash,1 non-specific chronic low back pain (NSCLBP),2 fibromyalgia,3 osteoarthritis (OA) of the knee,4 shoulder pain5 and sports related pain.6 Centrally sensitised individuals experience high levels of pain disproportional to the extent of concurrent tissue pathology, with no clear pattern of provocation nor easement, and that is not distributed in the regular dermatomal patterns.7–9
It is not clear why some individuals develop CS pain, yet others make a full recovery. Compared to non-CS pain populations, individuals with CS pain show associated changes in the central nervous system (CNS), such as sensory processing10 and emotional networks.11 It is not clear whether these differences were present prior to CS pain, or as a result of the onset of pain. Furthermore, the personal and environmental contexts in which CS pain develops might determine whether a person recovers or transitions to chronic pain.
Qualitative research is rare in studies investigating CS pain specifically, and yet it can afford valuable insight into the patient experience and lived life context surrounding their pain. Understanding aspects of pre-morbid CNS-related functioning and the contexts in which pain develops might provide insight into how CS pain arises. It was anticipated that exploring the pre-morbid lives of individuals with CS pain might help to identify areas of interest, which may subsequently inform investigations into the aetiological factors behind CS.
The aim of this study therefore was to explore the pre-morbid experiences and personal characteristics of participants with CS pain from a NSCLBP population.
MethodsTheoretical frameworkThe primary theoretical driver was a concurrent quantitative study12 (submitted). The present study was underpinned by a post-positive philosophical position paying attention to: (i) the quality of the data, whereby questionnaires are one dimensional and do not give voice to the context and reasons behind answers; (ii) the use of an integrated approach whereby subjective experiences account for some of the pain outcome being studied; and (iii) the context of the targeted phenomenon, in this case, the development of CS pain.13 This study is reported according to the Standards for Reporting of Qualitative Research (SRQR).14
DesignThis is a qualitative, exploratory study, using a concurrent nested design within a larger mixed methods protocol.
Recruitment and samplingParticipants were recruited from the quantitative sample by purposive sampling.15 Recruitment for the original quantitative sample was performed by clinical physical therapists experienced in pain neurophysiology and management, from physical therapy-led outpatient and pain clinics in England, Ireland and New Zealand. The inclusion criteria for the quantitative sample were for adults (age 18–64) with chronic (>3 months), non-specific (no specific pathology identified) low back pain (NSCLBP), with a predominant central sensitisation (CS) pain presentation according to the current published clinical guidelines for the clinical recognition of predominant central sensitisation in low back pain populations.2,7,9 The quantitative study recruited n=165 participants with NSCLBP and predominant CS (n=126 female) with a mean age of 45 (SD+/−12), 32% of whom were not on pain-related medication. A pilot study of the concurrent quantitative component had identified a prevalence of trait sensory hyper- and hypo-sensitivity profiles16,17 and anxiety-related personality types18 in individuals with NSCLBP and CS pain.19 Using this information, potential participants were stratified into n=6 groups based on their sensory profiles and personality type combinations. These groups were based on three trait anxiety-related personality type groups (defensive high anxious, high anxious, and repressors20) and two sensory profile (sensory hyper- or hypo-sensitive16,17) combinations. n=12 individuals were purposively selected (n=2 from each group). Individuals were provided with information about the study prior to giving written consent. Those who consented were given the option of being interviewed individually in their own home, at a physical therapy clinic, or the University campus.
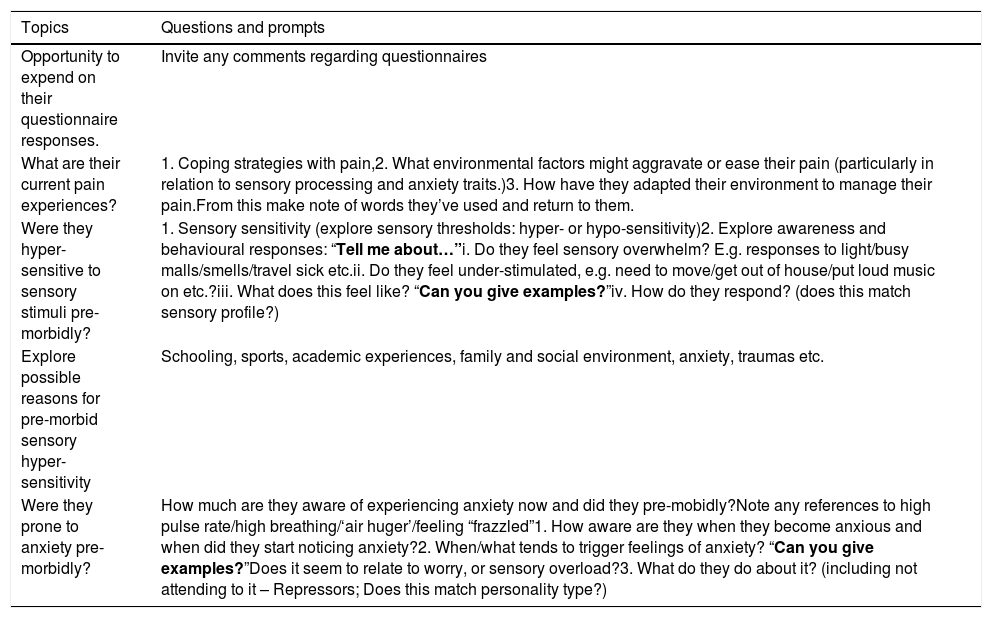
Interview scheduleQuestions for the interview schedule were derived from the literature around sensory sensitivity and trait anxiety and from information which emerged from the pilot study.19 The interview schedule is summarised in Table 1. Interviews were digitally recorded and transcribed verbatim. Transcripts were sent to each participant for verification. Participant anonymity was assured through allocation of a number (P1-9). Data were protected by password encryption and managed using NVivo 10 software.21
The interview guide used for centrally sensitised people with non-specific chronic low back pain, to understand the context in which CS developed in relation to pre-morbid anxiety and sensory sensitivity characteristics.
| Topics | Questions and prompts |
|---|---|
| Opportunity to expend on their questionnaire responses. | Invite any comments regarding questionnaires |
| What are their current pain experiences? | 1. Coping strategies with pain,2. What environmental factors might aggravate or ease their pain (particularly in relation to sensory processing and anxiety traits.)3. How have they adapted their environment to manage their pain.From this make note of words they’ve used and return to them. |
| Were they hyper-sensitive to sensory stimuli pre-morbidly? | 1. Sensory sensitivity (explore sensory thresholds: hyper- or hypo-sensitivity)2. Explore awareness and behavioural responses: “Tell me about…”i. Do they feel sensory overwhelm? E.g. responses to light/busy malls/smells/travel sick etc.ii. Do they feel under-stimulated, e.g. need to move/get out of house/put loud music on etc.?iii. What does this feel like? “Can you give examples?”iv. How do they respond? (does this match sensory profile?) |
| Explore possible reasons for pre-morbid sensory hyper-sensitivity | Schooling, sports, academic experiences, family and social environment, anxiety, traumas etc. |
| Were they prone to anxiety pre-morbidly? | How much are they aware of experiencing anxiety now and did they pre-mobidly?Note any references to high pulse rate/high breathing/‘air huger’/feeling “frazzled”1. How aware are they when they become anxious and when did they start noticing anxiety?2. When/what tends to trigger feelings of anxiety? “Can you give examples?”Does it seem to relate to worry, or sensory overload?3. What do they do about it? (including not attending to it – Repressors; Does this match personality type?) |
Ethical approval was granted by Manchester Metropolitan University, Manchester, United Kingdom (ref: 1205) and permission was granted by the Northern Y Ethics committee, New Zealand.
Data analysisData were analysed using a ‘theoretical’ thematic analysis approach. Analysis was driven by the analytic focus of the primary theoretical driver in the concurrent quantitative study. ‘Theoretical’ thematic analysis provides a detailed analysis of certain aspects of interest predetermined by the researcher.22 The aspects of interest were around pre-morbid trait characteristics related to sensory processing and personality.
Transcripts and field notes were used for analysis. Field notes assisted understanding contexts in which interview data were given. Transcription data were analysed using thematic analysis according to guidelines by Braun and Clarke.22 Data were coded from participant data extracts and collated into categories. Categories were grouped into themes and sub-themes. Two researchers [JC and GY] analysed the data independently and were in substantial agreement over the final themes following the discussion of any semantic differences.
FindingsParticipant demographics will be presented followed by data under the theme and sub-theme headings.
Participantsn=12 participants were initially identified from NZ and the UK. n=4 participants were lost to the study: n=2 participants could not be contacted (n=1 in UK, n=1 in NZ), n=1 UK participant declined due to unavailability at the time of the interviews, and n=1 because she felt she had recovered from her NSCLBP. n=1 further participant was recruited from NZ. In total, nine in-depth, face-to-face, semi-structured interviews were undertaken, n=8 from NZ and n=1 from UK. Seven of the participants elected to be interviewed in their own homes and two male participants elected to be interviewed at the physical therapy clinic of the primary investigator (JC) who conducted all the interviews. Each interview took place over a period of 60–100min. Any follow-up clarification of unclear information was performed by the primary investigator over the telephone.
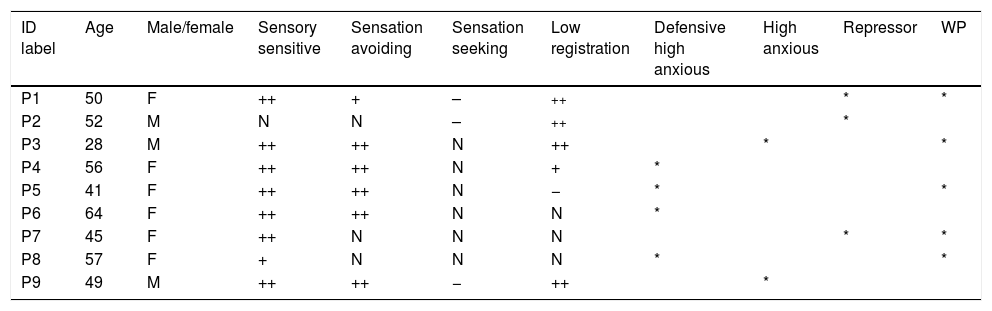
Participants were aged 28–64 years, n=6 female and n=3 male. Based on scores from the Adolescent, Adult Sensory Profile,16n=3 participants scored in the extreme ranges for the Low Registration sensory profile. All scored in the extreme ranges for the Sensory Sensitive Sensory and Sensation Avoidance profiles. Based on measures of trait anxiety and defensiveness,18 personality types included n=4 Defensive High Anxious, n=3 Repressor and n=2 High Anxious individuals. n=5 participants had widespread pain (WP) as well as non-specific chronic low back pain (NSCLBP), the others had regional NSCLBP (Table 2). Data saturation was reached from the 9 interviews.
Participant demographics: identification (ID) label, age, trait sensory profile and personality type characteristics, and the presence of widespread pain (WP).
| ID label | Age | Male/female | Sensory sensitive | Sensation avoiding | Sensation seeking | Low registration | Defensive high anxious | High anxious | Repressor | WP |
|---|---|---|---|---|---|---|---|---|---|---|
| P1 | 50 | F | ++ | + | – | ++ | * | * | ||
| P2 | 52 | M | N | N | – | ++ | * | |||
| P3 | 28 | M | ++ | ++ | N | ++ | * | * | ||
| P4 | 56 | F | ++ | ++ | N | + | * | |||
| P5 | 41 | F | ++ | ++ | N | − | * | * | ||
| P6 | 64 | F | ++ | ++ | N | N | * | |||
| P7 | 45 | F | ++ | N | N | N | * | * | ||
| P8 | 57 | F | + | N | N | N | * | * | ||
| P9 | 49 | M | ++ | ++ | − | ++ | * |
Keys: ++, much more than normal; +, more than normal; N, normal; −, less than normal, *, much less than normal. ‘P’ indicates the participant and their identification label number.
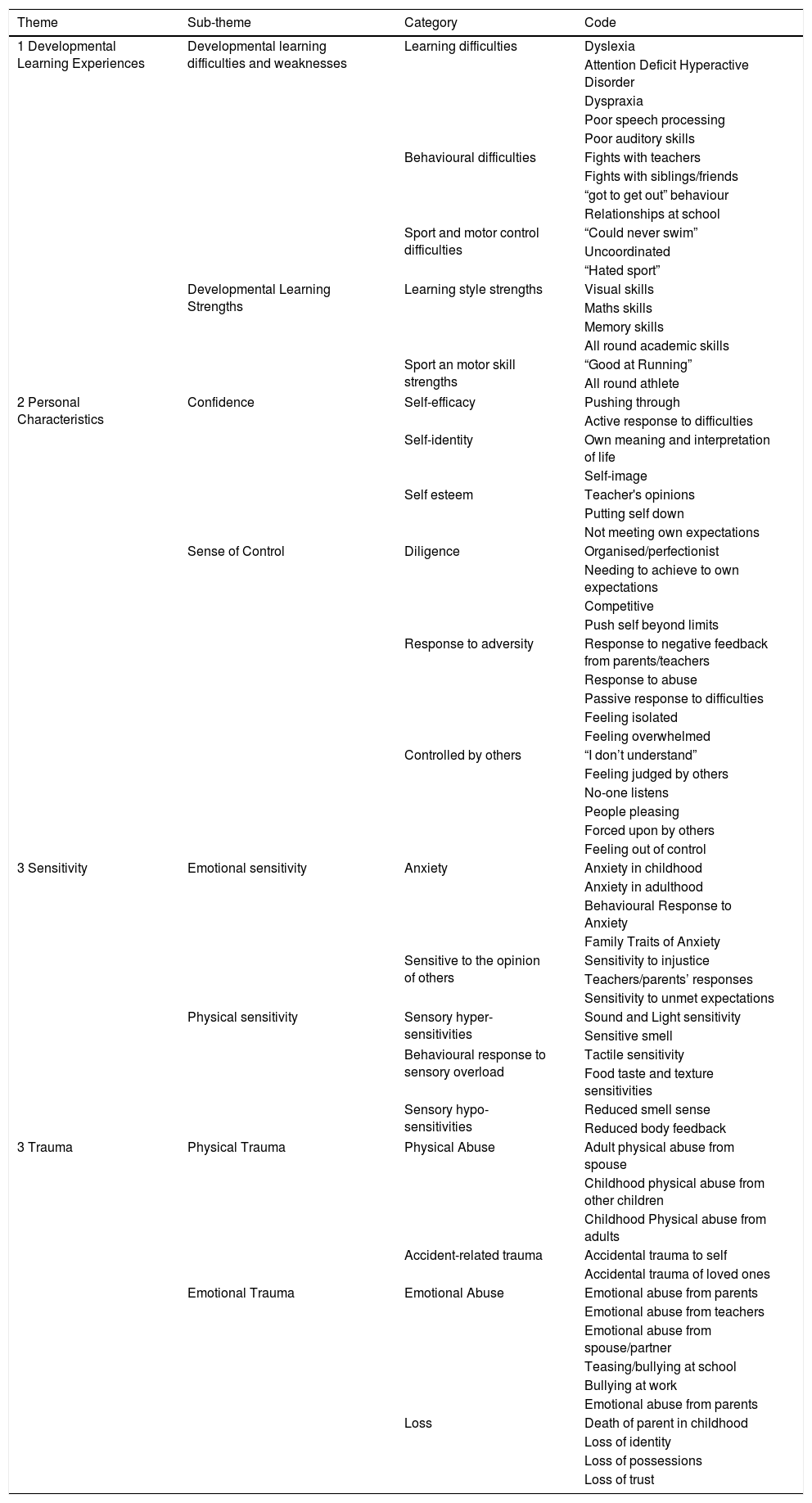
Four themes emerged: Developmental Learning Experiences, Personal Characteristics, Sensitivity and Trauma (Table 3). Findings in relation to each theme were divided into sub-themes and sub-headings. Due to the complexity and number of elements included, sub-themes overlap. The data extracts related to each theme are listed in Table 4.
Themes grouped into sub-themes, categories and codes.
| Theme | Sub-theme | Category | Code |
|---|---|---|---|
| 1 Developmental Learning Experiences | Developmental learning difficulties and weaknesses | Learning difficulties | Dyslexia |
| Attention Deficit Hyperactive Disorder | |||
| Dyspraxia | |||
| Poor speech processing | |||
| Poor auditory skills | |||
| Behavioural difficulties | Fights with teachers | ||
| Fights with siblings/friends | |||
| “got to get out” behaviour | |||
| Relationships at school | |||
| Sport and motor control difficulties | “Could never swim” | ||
| Uncoordinated | |||
| “Hated sport” | |||
| Developmental Learning Strengths | Learning style strengths | Visual skills | |
| Maths skills | |||
| Memory skills | |||
| All round academic skills | |||
| Sport an motor skill strengths | “Good at Running” | ||
| All round athlete | |||
| 2 Personal Characteristics | Confidence | Self-efficacy | Pushing through |
| Active response to difficulties | |||
| Self-identity | Own meaning and interpretation of life | ||
| Self-image | |||
| Self esteem | Teacher's opinions | ||
| Putting self down | |||
| Not meeting own expectations | |||
| Sense of Control | Diligence | Organised/perfectionist | |
| Needing to achieve to own expectations | |||
| Competitive | |||
| Push self beyond limits | |||
| Response to adversity | Response to negative feedback from parents/teachers | ||
| Response to abuse | |||
| Passive response to difficulties | |||
| Feeling isolated | |||
| Feeling overwhelmed | |||
| Controlled by others | “I don’t understand” | ||
| Feeling judged by others | |||
| No-one listens | |||
| People pleasing | |||
| Forced upon by others | |||
| Feeling out of control | |||
| 3 Sensitivity | Emotional sensitivity | Anxiety | Anxiety in childhood |
| Anxiety in adulthood | |||
| Behavioural Response to Anxiety | |||
| Family Traits of Anxiety | |||
| Sensitive to the opinion of others | Sensitivity to injustice | ||
| Teachers/parents’ responses | |||
| Sensitivity to unmet expectations | |||
| Physical sensitivity | Sensory hyper-sensitivities | Sound and Light sensitivity | |
| Sensitive smell | |||
| Behavioural response to sensory overload | Tactile sensitivity | ||
| Food taste and texture sensitivities | |||
| Sensory hypo-sensitivities | Reduced smell sense | ||
| Reduced body feedback | |||
| 3 Trauma | Physical Trauma | Physical Abuse | Adult physical abuse from spouse |
| Childhood physical abuse from other children | |||
| Childhood Physical abuse from adults | |||
| Accident-related trauma | Accidental trauma to self | ||
| Accidental trauma of loved ones | |||
| Emotional Trauma | Emotional Abuse | Emotional abuse from parents | |
| Emotional abuse from teachers | |||
| Emotional abuse from spouse/partner | |||
| Teasing/bullying at school | |||
| Bullying at work | |||
| Emotional abuse from parents | |||
| Loss | Death of parent in childhood | ||
| Loss of identity | |||
| Loss of possessions | |||
| Loss of trust |
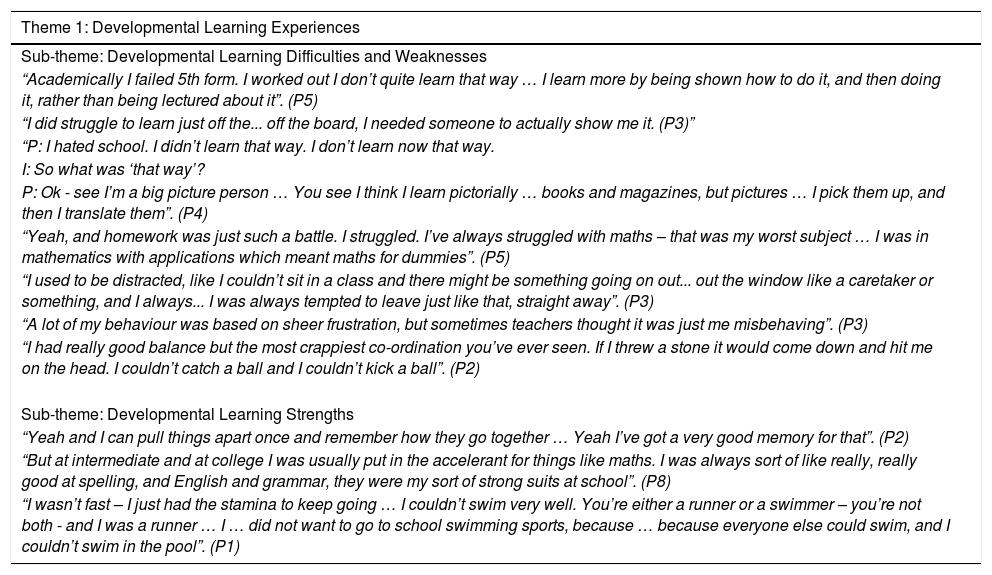
Direct quotations representing identified themes and subthemes from centrally sensitised participants with non-specific chronic low back pain.
| Theme 1: Developmental Learning Experiences |
|---|
| Sub-theme: Developmental Learning Difficulties and Weaknesses |
| “Academically I failed 5th form. I worked out I don’t quite learn that way … I learn more by being shown how to do it, and then doing it, rather than being lectured about it”. (P5) |
| “I did struggle to learn just off the... off the board, I needed someone to actually show me it. (P3)” |
| “P: I hated school. I didn’t learn that way. I don’t learn now that way. |
| I: So what was ‘that way’? |
| P: Ok - see I’m a big picture person … You see I think I learn pictorially … books and magazines, but pictures … I pick them up, and then I translate them”. (P4) |
| “Yeah, and homework was just such a battle. I struggled. I’ve always struggled with maths – that was my worst subject … I was in mathematics with applications which meant maths for dummies”. (P5) |
| “I used to be distracted, like I couldn’t sit in a class and there might be something going on out... out the window like a caretaker or something, and I always... I was always tempted to leave just like that, straight away”. (P3) |
| “A lot of my behaviour was based on sheer frustration, but sometimes teachers thought it was just me misbehaving”. (P3) |
| “I had really good balance but the most crappiest co-ordination you’ve ever seen. If I threw a stone it would come down and hit me on the head. I couldn’t catch a ball and I couldn’t kick a ball”. (P2) |
| Sub-theme: Developmental Learning Strengths |
| “Yeah and I can pull things apart once and remember how they go together … Yeah I’ve got a very good memory for that”. (P2) |
| “But at intermediate and at college I was usually put in the accelerant for things like maths. I was always sort of like really, really good at spelling, and English and grammar, they were my sort of strong suits at school”. (P8) |
| “I wasn’t fast – I just had the stamina to keep going … I couldn’t swim very well. You’re either a runner or a swimmer – you’re not both - and I was a runner … I … did not want to go to school swimming sports, because … because everyone else could swim, and I couldn’t swim in the pool”. (P1) |
| Theme 2: Personal Characteristics: |
|---|
| Sub-theme: Confidence |
| “(The convent was) really where I wanted to go... And if I’m really truthful today, that's where I’d like to be. That is me, that is who I am … that is who I am. I’m a woman of prayer and a lover of God … that is me”. (P6) |
| “I really struggle with low energy because I’m a person of high energy and motivation. So... I really struggle with it”. (P3) |
| “I do believe that what you go through as a child it shapes your core beliefs. It shapes your core beliefs, and in my family you just get on with it, you don’t complain”. (P5) |
| “I think.. a lot of how I grew up was feeling subdued, feeling like I had to be different. I had to be like them, and I wasn’t”. (P4) |
| “And … if I’m thinking I’m stupid, well they’re going to think I’m stupid … so there was two people at the table I didn’t know, and because I didn’t know them, I was tense and stressed for at least the first hour or so. Yeah because it was just out of my comfort zone cause I didn’t know them. Yeah which is silly – it does seem silly”. (P5) |
| “I’ve learnt to relax in terms of you can only do what you can do, you can only influence what you put your hand to so don’t stress out. And I’ve learnt to... even though I may not be able to spell, but I can read it, learnt to write lists or write things down…” (P3) |
| “I just had the stamina to keep going. Mm. Just keep going in life. I don’t know, I just put up with it, I just put up with life really”. (P1) |
| Sub-theme: Sense of Control |
| “It should be like this. … I think ‘this’ was like harmony, like everyone … everyone is in harmony, and there's understanding, and it's happy and it's joyful. Yeah it's harmonious. It's not disjointed and fragmented … it's not fragmented. I felt my life was very fragmented, and I felt very much alone”. (P6) |
| “In my mind if I didn’t get something done, if there was a deadline or there was going to be some kind of negative problem from it, I would push myself, I would just carry on and do it even though I knew that I wasn’t really being very kind to myself”. (P7) |
| “I have to learn to say no, so I’m learning to say no to things … Never (said) no. … I think it was the fear. It was a fear of upsetting someone”. (P7) |
| “Yeah, I just couldn’t handle that. I used to have to go away and crawl under the house... So you lived this life of, “wait a minute, if this is how it is then I’m the only one, I have to take control of me. I have to really make sure that I know what I’m doing and no-one, and I repeat no-one, is going to shake that.” (P6) |
| Theme 3 Sensitivity: |
|---|
| Sub-theme: Emotional Sensitivity |
| “So I’ve always obviously been a bit anxious. My mum is a ‘panicker’ … … Yeah, and she’d install her fear into me I guess without knowing it, and that would make me anxious, you know. Yeah. … It was like ‘oh my goodness’, and that would just instantly put anxiety into me”. (P2) |
| “I absolutely panicked over exams, just panicked in exams and go completely blank just because of the stress of not doing well, more than anything. … My mum always used to say before exams, ‘now we know you’ve worked really hard so don’t worry,’ and then if I didn’t get anything there or what they thought I should get I was in terrible problems – trouble”. (P7) |
| “It's so weird [chuckles]. It's all very, very odd, but yeah I … yeah I worry about what people think too much”. (P5) |
| “… if I have made a mistake I beat myself up... to quite some considerable amount…. And I’ve got a big thing about being normal and not showing anyone any type of weakness. And if people do find that weakness and sort of make a joke about it, it hits home pretty hard”. (P3) |
| “I’ve always thought, and I don’t know if it's exact anxiety as such, but I’ve always thought if I haven’t got something to worry about I’ll make something up … yeah my dad's a worrier, his mother was a worrier, you know, it's a bit of a family trait” (P8). |
| “I think again, seeing my kids is very interesting because I think there's definitely a natural genetic in it that they’re sensitive to people. Particularly (son) and (daughter) are both similar to me in that they’re very sensitive … well they’re all sensitive to other people's feelings, but they are very sensitive to people and what they think and getting things wrong. Yeah so I think for me there's a combination of already being like that naturally…” (P7) |
| Sub-theme: Physical Sensitivities |
| “Yeah, well I know I’ve got sensitivity to light. I don’t recall how long that's been going on, but... needing sunglasses on even if it wasn’t bright sunlight”. (P8) |
| “I’m massively sensitive to sound. I get very irritated with sound, any kind of repetitive sound. And there's one particular kind of music which … is it house music where it's just like the same beat all the time, I literally feel like I want to hit my head against a wall. Yeah sound is one thing, but then the sound of water or something I really like, but there are certain sounds that can very quickly get me highly irritated”. (P7) |
| “I know I’ve always been startled easily by loud noises, like somebody popping a balloon or oooh!” (P8) |
| “…but too strong - if it's a bad smell, like turps or kerosene - and I can smell burning a mile off - I became afraid of smell … The smell I was actually nauseous”. (P1) |
| “Oh I bounced – oh yeah I bounced. Mum would say to me too much cheese would affect me, but yeah different foods … But I had to be a bit careful”. (P2) |
| “It's the texture and the thought of biting down. I mean I’ve tried a few new foods but I can’t even tell you what they taste like because the anxiety level was so high and the thought of chewing down on them is just … (screws up face) … Like even now when I roast the chicken I use tongs to pull the meat off, … there's no way I’d touch them”. (P5) |
| “Often in the evenings I will do my fitness, then come home and that's when I tend to just sort of almost like blob out, just watch something and just try and block all things out. And there's often... if I get too over-stimulated I can’t get to sleep at night”. (P3) |
| “So yes, and I also get quite – not panicky exactly, but agitated if I’ve got too much going on in the week”. (P8) |
| “It doesn’t bother me – strong smells [chuckles]. I’ve worked with sewerage pumps [laughs] … I don’t smell things that other people say they smell, frequently”. (P2) |
| Theme 4 Trauma: |
|---|
| Sub-theme: Physical trauma |
| Some described physical abuse: |
| “…And he just grabbed me and smacked me, like kept on punching me and punching me and punching me and punching me and punching me. And he grabbed a knife and held it to my throat, and that was it, my life was over. … He used to smash all my stuff - … He used to, you name the abuse, he just didn’t care”. (P1) |
| “I mean I used to get smacked, I suppose in those days you’d call it. Well the nuns used to strap me. Oh, they would strap me for being naughty, and I would just go, “I was just having fun”. (P4) |
| Others described physical trauma related to an accident: |
| “It was massive disappointment because I loved it so much and it was really, really fulfilling in every way, sort of emotionally, physically, everything. So yeah it's sort of very hard to then think well what can I do, because you’re so fulfilled with what you do…” (P7) |
| “And then (daughter) was in a car accident when she was... she was 17. So that actually's when all of this started”. (P8) |
| Sub-theme: Emotional trauma |
| “I had a husband before [husband 2] – [husband 1] … he also was abusive … He used to threaten to burn me in my bed, standing with petrol cans and a lighter, and go “shall I do it now, shall I burn you now?” (P1) |
| “I mean I wasn’t (physically) abused as a child or anything like that, but I think there's different ways of damaging children… But I mean mum used to try to get me to eat things, and (step-father) used to really try to the point where the house would just be a tense, stressful, shouting, horrible place to be at the dinner table, every single night”. (P5) |
| “’Cos then my cousin was killed when she was just 18, and her parents I... you know, spent my holidays with so I was really close with her. And then (daughter) was in a car accident. So that is actually when all of this started … I still feel like the worst of everything started up at that accident, the last accident”. (P8) |
| “Growing up with only one parent I think is going to be stressful for a start … So my first stress – obviously my mother (dying). And this is what I think all of this stems from is post-traumatic stress”. (P8) |
Theme 1, Developmental Learning Experiences, related to childhood and adolescent experiences of school and the environment in which they grew up. Participants described diagnosed difficulties in learning such as dyslexia, or related disorders such as dyspraxia and ADHD. Other participants described differences in learning preferences but who had never received any formal diagnoses. Difficulties holding attention in class and a tendency towards boredom was reported by nearly half of the participants. A few participants claimed to be poorly coordinated in sports and play activities as a child; this was found in participants who had learning difficulties and a Low Registration sensory profile, characterised by reduced sensory feedback and slower movement.17
Participants with learning difficulties also displayed learning strengths in other aspects of their development. Contrary to learning difficulties, two of the participants demonstrated all round learning strengths and intelligence, such as reading, writing and maths. Conversely to having all-round sports strengths, two participants (both with extreme scores in the Low Registration sensory profile) described themselves as having strength in only running sport but being uncoordinated in other motor skills.
Theme 2, Personal Characteristics, determines how a person copes with challenges and unexpected events as well as aspects of resilience and confidence. Personal characteristics also determine behavioural responses and their tendency to interpret situations in a positive light or, alternatively, as situations which are threatening. The theme of personal characteristics encompasses two sub-themes, Confidence and Sense of Control.
Confidence covers aspects of attitudes and behaviours related to self-confidence, such as self-efficacy, self-esteem and self-identity. Having a strong sense of self-identity appeared to have a positive and a negative impact on individuals. Self-identities appeared to be enduring and learned from childhood. A negative impact of holding to these strong identities meant that a few of the participants developed a tendency to push themselves past their limits of wellbeing. A mismatch between expectation and the real lived experiences often led to low self-esteem and a sense of being weaker than peers.
A Sense of Control encompasses the categories of diligence and responses to adversity, both of which relate to behaviours of staying in control; and being controlled by others. Responses to adversity to regain a sense of control varied from active through to passive responses across the group and this appeared to relate closely to their individual trait sensory profiles and personality types.
Theme 3, Sensory Sensitivity, relates to the reception and perception of sensory stimuli, with higher sensitivity implying a lower neurological threshold for stimulation. Sensory sensitivity was apparent in the lives of all participants and presented in various forms of emotional and physical sensitivities. A large component of emotional sensitivity was anxiety, in which individuals were prone to responding to potential or actual threats with anxiety. Other emotional sensitivities emerged which were sensitivity to the opinion of others and sensitivity to injustice or unmet expectations. Physical sensitivity included sensitivity to touch, sound, light, smell and body feedback, as well as sensitivity to certain foods and food textures. Participants varied in their responses to sensory discomfort depending on their individual sensory profile.
All participants reported various physical sensitivities. Most participants reported high sensitivity, not handling as much as they considered they should in terms of certain physical stimuli, possibly suggestive of sensory hyper-sensitivity. A small number also reported they were unable to feel or sense certain sensory stimuli as much as others or as much as they thought they should, possibly suggesting sensory hypo-sensitivity. There was clearly overlap between sensory discomfort and emotional response, such as feelings of anxiety, linking together physical and emotional sensitivity.
Theme 4, Trauma, relates to both emotional and physical trauma. Emotional trauma was experienced in the forms of abuse, being controlled by others and in personal loss and overlaps with physical trauma. Physical trauma was experienced by many participants in the form of physical abuse and accident related trauma. Emotional trauma was prevalent in many of the participants, some as a result of abuse from others and some as a result of circumstances outside of their control, such as loss, or being controlled by others.
DiscussionThe aim of this study was to explore the pre-morbid experiences and personal characteristics of participants with CS pain from a NSCLBP population and this is the first time this has been done. The emergence of the theme of developmental learning experiences was unexpected, in so much as a large proportion of the study group appeared to have diagnosed or undiagnosed learning difficulties. Learning difficulties, such as dyslexia, have only been recognised relatively recently in terms of formal diagnoses in New Zealand.23
Learning difficulties are associated with sensory processing differences.24,25 The way the CNS processes sensory information affects learning function.26 Learning difficulties are associated with impaired sensory gating which includes sensory hypo-sensitivity and hyper-sensitivity.25,26 The latter is characteristic of CS pain7,9,27 and found in participants in the current study. The sensory processing differences seen in individuals with learning difficulties are likely to alter sensory-motor function whereby gross motor skills decrease with increasing learning disability,28 noted in the sports performance reported by participants in the current study.
Our data revealed links between sports skills and developmental learning strengths. The most versatile sports skills belonging to the women with the most normal sensory profile scores. Both women (P7 and P8) also alluded to long term tendencies towards anxiety through emotional sensitivity. They might have experienced ongoing stress responses due to anxieties rather than sensory processing difficulties.
Personal characteristics involving people-pleasing and being goal focussed appeared to motivate participants to continue pushing themselves beyond their capacity creating stresses. Participants with repressor personality types appeared to under-play negative affect and report seemingly stressful situations with a “positive spin.” Repressors are known to respond to stressors with autonomic arousal but remain positive in their reporting of information about themselves.29 Participants with high anxious or defensive high anxious personality types reported many events as stressful, such as being bullied for their learning difficulties, difficulty in sports or academics at school, and are therefore very likely to have regularly been prone to physiological arousal through autonomic stress responses.
Sensory hyper- and hypo-sensitivity emerged as having been present from a young age in many participants. This supports the results of other work30 (submitted), in which extreme scores in sensory hyper- and hypo-sensitivity profiles were found in participants with CS and NSCLBP. Pre-morbid hyper-sensitivity found in the current study may also be linked to the results of a systematic review in which pre-morbid or baseline hyper-sensitivity (using quantitative sensory testing and genetic markers) was a factor in the development of CS pain in individuals with chronic musculoskeletal pain.31
Sensory hyper- and hypo-sensitivities have been found by others to be associated with autonomic stress responses in young people.32 Similarly, trauma is known to create a stress response in the traumatised individual, involving autonomic arousal and behavioural responses.33 Trauma and childhood adversities are also prevalent in the lives of individuals with various CS pain disorders such as fibromyalgia and somatoform disorders34,35 although the mechanisms leading to CS are unclear.
Trait anxiety-based personality types are said to be developed from a young age and are linked to the development of defensive coping strategies employed during difficult times in youth.36 Individuals do not “grow out of” learning difficulties or associated sensory processing disorders, they persist into adulthood.37 Persistent sensory processing disorders can include auditory and visual perception, speaking, maths, reading, spelling and coordination difficulties.37 All of these were apparent in the lives of most of the participants in this study. Some of these disorders of the CNS may overlap with those seen in individuals with CS pain (e.g. visual processing disturbance in Refs. 39, 40).
A common link between sensory sensitivity and trauma is in the stress response, which may heighten sensitivity to sensory stimuli through the upregulation of glial cells and neuro-inflammation in the CNS.40 There is some evidence to suggest that individuals with whiplash associated disorder after a trauma experience post-traumatic stress41,42 and CS pain43 which may further link trauma, stress responses and CS pain. Furthermore, post-morbidly, CS pain may heighten emotional sensitivity in individuals with high trait anxiety, by increasing state anxiety. Physical sensitivity to various sensory stimuli was prevalent among all the participants and a few were even hypo-sensitive. Extremes of sensory sensitivity are associated with sensory processing disorders25,44 and anxiety45 and relationships between these and CS pain require further investigation.
Strengths and limitationsThe interviewer was an experienced physical therapist with an in-depth clinical knowledge of individuals with CS pain. This, as well as information from the pilot study, helped inform the interview schedules and direct the theoretical thematic analysis.22 No participants reported being uncomfortable during the interviews and no participant having difficulty expressing their opinion/experience. The quality of the data was ensured through verification by each participant and rigour was improved through having a second data analyst. This study did satisfy our requirements for theoretical representativeness i.e. both male and female participants and representative of all three personality types.
Limitations may relate to the gathering of retrospective interview data which is dependent on memory recall and subsequent interpretation of pre-pain events after CS pain has become established; this may be influenced by personality type insomuch as it is known that repressors tend to avoid negative memory recall.46,47 However, interesting information has emerged from this study to inform future investigations by other means which may further enlarge on the current study findings. All participants had sought treatment and therefore may not reflect people in the community who self-treat or do not seek physical therapy.
ConclusionThis study explored pre-morbid experiences in people with CS pain in order to develop a better understanding of sensory profiles and personality types in relation to CS in this population. Four main themes were identified, developmental learning experiences, personal characteristics, and physical and emotional sensitivity and trauma. There was a general lack of confidence, low esteem and need to please others, although most had coping strategies. All participants recounted multiple physical hyper-sensitivities such as smell, light, sound and/or emotional sensitivity and a few reported physical hypo-sensitivity. Many had suffered emotional and/or physical traumas pre-morbidly. All themes may be related to stress responses in the CNS, which may be linked to some of the physiological changes seen in CS pain. Further investigation into the role of pre-existing sensory processing disorders, as a component of impaired or altered CNS function, in relation to CS pain is warranted.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interestThe authors declare no conflicts of interest.



