
The production of finger force control is essential for a large number of daily activities. There is evidence that deficits in the mechanisms of accuracy and control of finger force tasks are associated with children's motor difficulties.
ObjectiveTo compare the effect of practice of an isometric finger force/torque task between children with significant movement difficulty and those with no difficulty movement.
MethodsTwenty-four children aged between 9 and 10 years (12 at risk of developmental coordination disorder and 12 with no movement difficulty – typically developing children) were asked to produce finger force/torque control in a continuous and constant 25% of maximum voluntary torque with visual feedback during 15s. Practice was given during five consecutive days with 15 trials per day. After the practice with visual feedback, children were asked to perform five trials without visual feedback. In these trials, feedback was removed 5s after the start of the trial.
ResultsTypically developing children were consistently more accurate in maintaining finger force/torque control than those children at risk of developmental coordination disorder. Children from both groups improved the performance in the task according to practice sessions. Also, children at risk of developmental coordination disorder poorly performed the task without visual feedback as they did when visual feedback was available.
ConclusionThe present study give support to the idea that movement difficulty is associated with finger force/torque control and children at risk of developmental coordination disorder can improve finger force/torque control with practice when visual feedback is available.
A functional feature of the hand is to hold and manipulate objects through an integration action between the fingers and the thumb to perform many daily activities, such as using cutlery, brushing teeth, writing and painting with pencil. The action between the index finger and the thumb is pinch grip and requires from central nervous system to control digit-tip force production during prehension tasks.1 The control of force production of children's fingers in these tasks shows a larger degree of variability than that of adults.2,3 This may occur because human beings use visual information in a more flexible way over the years, leading to a shift in strategy from dependence on visual information to feedforward control of grip force.4,5 However, for some children this trend does not occur throughout development. These children are often identified with Developmental Coordination Disorder (DCD)6 by showing impairments in overall motor coordination that affect motor performance in daily activity tasks, with the impairment not related to medical condition.6
Difficulties as in the execution of daily manual activities7,8 such as shoe lacing and writing7 are the first observed in children with DCD due to their lack of control of finger force production.1,9–11 Previous studies showed that children with DCD have higher variability in controlling finger force pulses,12 higher grip forces during lifts of objects of difference textures,10 and poor control in the manipulation in tasks with torque production,1 than typically developing children (TD). King et al.9 showed that the development of finger force control in children with DCD is similar to TD children, but it is delayed. It has been suggested that children with DCD cannot use visual information efficiently to feedforward control of finger force because their motor behavior is associated with poor visuospatial processing.13,14
There are evidences that children with DCD depend more on visual information for execution of the control of walking15 and for execution of rhythmic tasks16 than TD children. However, other studies suggested that children with DCD, compared with TD children, did not exhibit increased dependency on vision but show less recognition of accuracy demands, less adaptation to the removal of vision, and less use of minimal visual information when it is available.17 Van Waelvelde et al.16 associated poor visuospatial processing to a difficulty of children with DCD in building up an internal representation of the movement task. In this way, the use of concurrent visual feedback in the performance of manipulative tasks could be a tool behind the improvement of the level of performance, i.e., reduction in variability as well as in error in the control of force and torque production3,18 by children with DCD.
Deutsch and Newell3 showed that, with practice, children reduced the variability of pinch grip force control by changing the structure of the force output as adults do. The authors concluded that regardless of age, variability on the production of force is associated with visual feedback information available during the execution of the task and with practice. Studies with special populations (Down syndrome,19 Parkinson's disease20 and cerebral palsy21), the practice of tasks involving force production with constant visual feedback was an important factor in the improvement of the level of performance.
The first aim of the study was to compare the effect of practice on the performance of an isometric force/torque control task (i.e., index finger and thumb) between children at risk of DCD (rDCD) and TD children. The hypothesis was that practice of the isometric force/torque task by children at rDCD leads to a reduction of variability and error in the force control. The second aim was to investigate the effect of visual feedback of force/torque control in children at rDCD. The hypothesis was that supplementary (visual) information could help the children at rDCD control finger force/torque.
MethodsParticipantsTwelve children, recruited from a public school in São Paulo state, aged between 9–10 years (10 females and 2 males; 10.12±0.49 years), scoring below or at the 5th percentile for total impairment in the Movement Assessment Battery for Children (M-ABC)22 were classified as being at risk of DCD (rDCD group). We adopt the term rDCD because our procedure did not consider all criteria described in the DSM-56 for DCD. The M-ABC provides a reasonable view of basic motor abilities functioning of each child. Furthermore, children with comorbidities such as attention deficit disorder, autism spectrum disorder, any neurological diagnosis screened by the school team at the commencement of the school year or children attending a specialized center for additional education were not included in the sample.
Other 12 children recruited from the same school matched by age and gender (10.04±0.55 years), scoring above or at the 35th percentile for total impairment in the M-ABC,22 with no movement difficulty, were classified as typically developing (TD group) children. We choose the 35th percentile to avoid select TD children scoring close to the cut-off point of at risk of movement difficulties, and to avoid poor performance in one of the three motor components of M-ABC. A physical therapist and a physical education teacher, both trained to administer the battery, tested the children. Participants were right-handed, according to their preferred hand for writing and had no history of neuropathy or trauma to their upper limbs. Parents of the participants gave informed consent for their participation according to the study protocol approved by the Ethics Committee of the Biosciences Institute, Universidade Estadual Paulista (n. 3030), Rio Claro, SP, Brazil.
Apparatus and taskThe device for the finger force/torque task consisted of a load cell sensor (S-Bean) mounted on an aluminum frame (rectangular base of 20cm of length, 7cm of width and 7.5cm of height) with moment arm of 0.0125m. The torque produced by thumb and index finger was calculated as torque=force×moment arm. The signals from the force transducer were sampled at 100Hz, amplified (MCS1000VB-EMG System) at an excitation voltage of ±5V with a gain of 300Hz and routed to an A/D converter of 12-bit resolution, and then stored on a personal computer. A MINIPA analog oscilloscope (MO-1221) was used to provide online visual feedback (20MHz) of the isometric finger force/torque. Participants were asked to perform two tasks: the maximum voluntary finger force/torque task (MVT); and the constant isometric finger force/torque task (CONST) at 25% of MVT. In both tasks participants pinched a knob attached to the load cell sensors with the index and thumb fingertips of the right hand and applied an isometric force contraction in the clockwise direction.
ProcedureParticipants seated on a comfortable chair facing the oscilloscope centered to the participant's eyes at a distance of 45cm. For preventing compensatory movements during the task, the participant's forearm was stabilized on a polyvinyl chloride (PVC) support and fixed with Velcro. First, participants executed five familiarization trials, which consisted of practicing the constant isometric finger force/torque task observing the force/torque produced in the oscilloscope. Participants were able to understand and follow the online visual feedback, according to the instructions. After 2min of rest, children were requested to exert the MVT on the force transducer after a verbal signal ‘go’ and maintain for 3s until the verbal signal ‘stop’. The maximum instant peak torque value registered over two trials served as the participant MVT.
For the practice phase, participants were asked to maintain a constant isometric force/torque output at a target force/torque level corresponding to 25% of the MVT (CONST task) on 20 trials per day for five consecutive days. Participants performed the first 15 trials with visual feedback and the last five trials without visual feedback. The visual feedback consisted of a horizontal line displayed on an oscilloscope screen, indicating the force/torque produced by the participant in relation with the 25% of MVT target of each participant. Participants should to superimpose the two lines (target and force/torque produced) for 15s. For trial without visual feedback, visual feedback was removed after 5s from the start of the trial. A retention test was administered two days after the last practice session, with participants performing five trials of the CONST task with visual feedback. Participants received resting intervals of 30s between trials.
Data analysesThe raw data were filtered using a low-pass second-order Butterworth filter with a cut-off frequency of 25–30Hz. The first 5s of each trial were cutoff to allow participants to adjust the required force/torque output. Performance accuracy for the CONST task was assessed by means of the root mean square error (RMSE) of force/torque produced, that was defined as: RMSE=√((∑(T−xi)2)/n), where T=the y axis target value (25% MTV), xi=the participant's value produced and n=the number of samples.4
The index of variability for the CONST task was assessed by the coefficient of variation (CV), defined as: CV=(SD/mean)×100, where SD was calculated as the square root of the average squared deviation of each number from its mean.
Statistical analysisThe last five trials with visual feedback and all five trials without visual feedback from each day of practice were used for statistical analyses. Shapiro–Wilk normality test showed that the set of means of all variables met the normality criteria. T-test was used to compare MVT results between groups. Mixed design 2 (Group)×6 (Day) ANOVAs with repeated measures were carried for CV and RMSE. Huynh-Feldt corrections were applied, when appropriate, to the degrees of freedom of F tests to compensate for violation of homogeneity assumptions. Significant main effects were analyzed using Tukey post hoc test. Interactions between factors were analyzed through the simple effects and contrasts by T-tests. Alpha level of 0.05 was adopted for statistical analysis.
ResultsMaximum voluntary finger force/torqueThe MVT of rDCD and of TD groups were similar, p=0.50 (rDCD=0.45Nm, SD=0.10; TD=0.48Nm, SD=0.16).
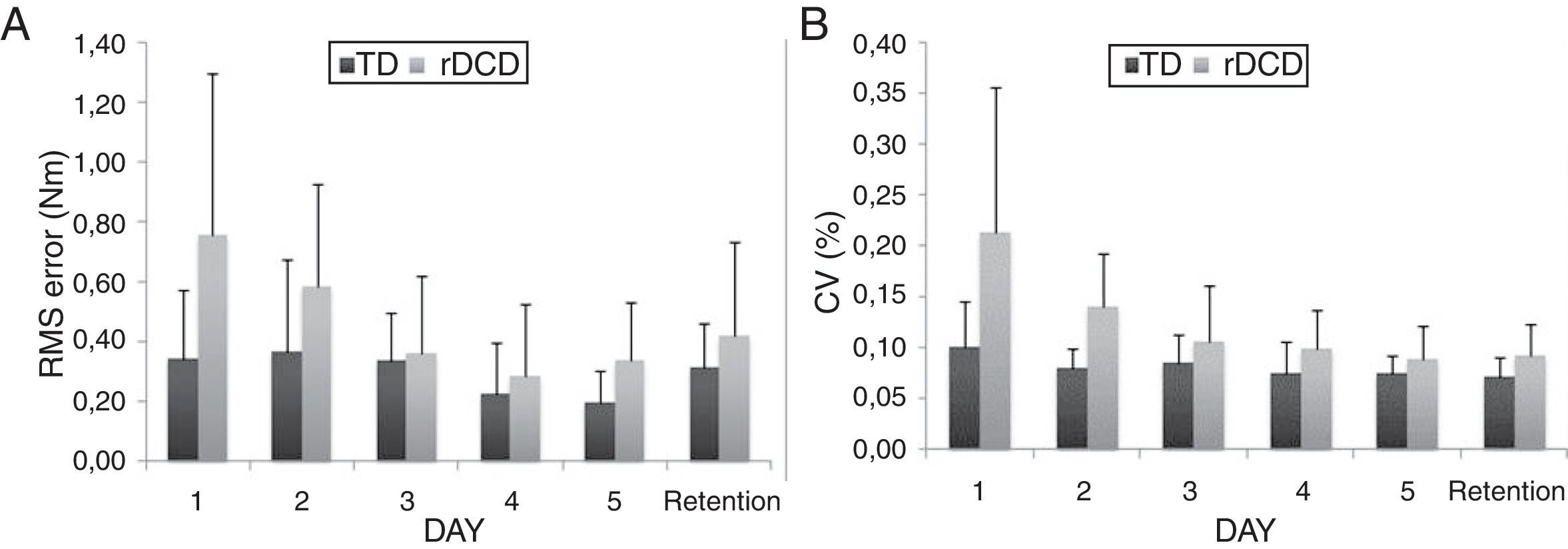
CONST task with visual feedbackRMSE. The results revealed significant Group (p<0.05) and Day effects (p<0.001). The rDCD group was significantly less accurate (0.45Nm) than the TD group (0.30Nm). Post hoc analyses indicated that the RMSE for both groups diminished significantly on Day 4 (0.25Nm) and 5 (0.26Nm, all p<0.05) compared with Day 1 (0.55Nm) of practice. Although the interaction between Group and Day was not significant, Fig. 1A shows that RMSE of rDCD group were gradually reduced throughout practice days (1=0.75Nm; 2=0.58Nm; 3=0.36Nm; 4=0.29Nm; 5=0.33Nm). TD children did not exhibit such RMSE reduction across the practice sessions as their peers (1=0.36Nm; 2=0.36Nm; 3=0.33Nm; 4=0.22Nm; 5=0.20Nm). With respect to the retention phase, children at rDCD (0.42Nm) showed higher RMSE than TD children (0.31Nm).
 and coefficient of variation (B) across the five days of practice and retention phase of children at risk of developmental coordination disorder and typically developing children.")
CV. The results indicated significant Group (p<0.01) and Day effects (p<0.001) and interaction between these factors (p<0.05) (Fig. 1B). Subsequent analyses of the significant interaction showed that the CV of rDCD group (p<0.05) was significantly higher on Day 1 of practice compared with Day 2 (p=0.05), 3, 4, 5, and retention phase (all p<0.01). The CV of TD group was significantly higher on Day 1 than on Day 4, 5 and retention phase (all p<0.05). Comparisons between groups for each day of practice showed that the CV of rDCD group was higher than the CV of TD group on Day 1 and 2 (p<0.05 and p<0.001, respectively).
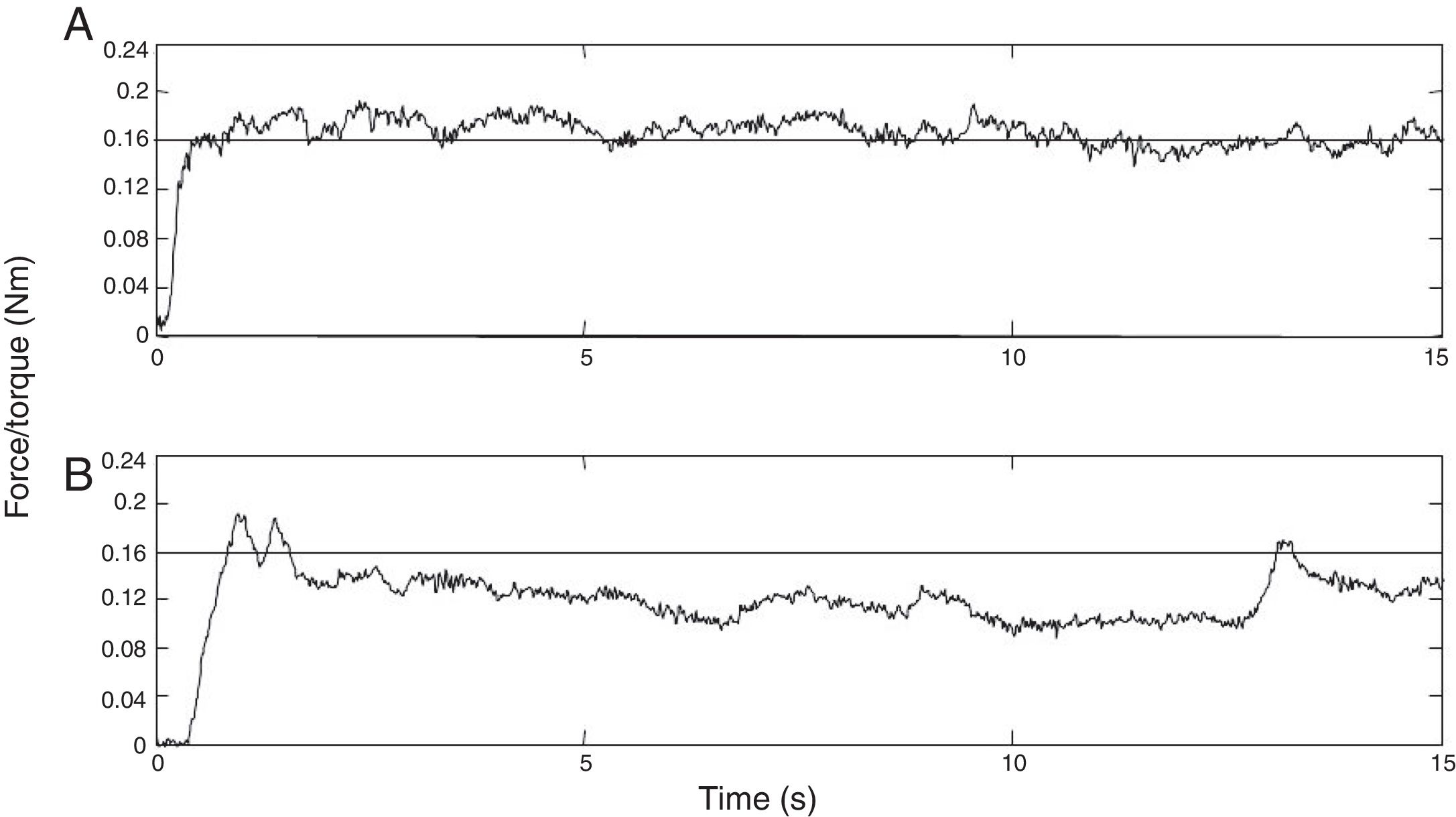
Fig. 2 shows examples of finger force/torque output trajectories corresponding to the 25% MVT, with visual feedback. The participant at rDCD (Fig. 2B) displays both lower accuracy and higher variability of control of isometric force/torque production throughout the trial compared to a TD child.
CONST task without visual feedback and isometric thumb/index force/torque outputs at 25% of the individual maximum voluntary finger force/torque of a typically developing child (A) and a child at risk of development coordination disorder (B).")
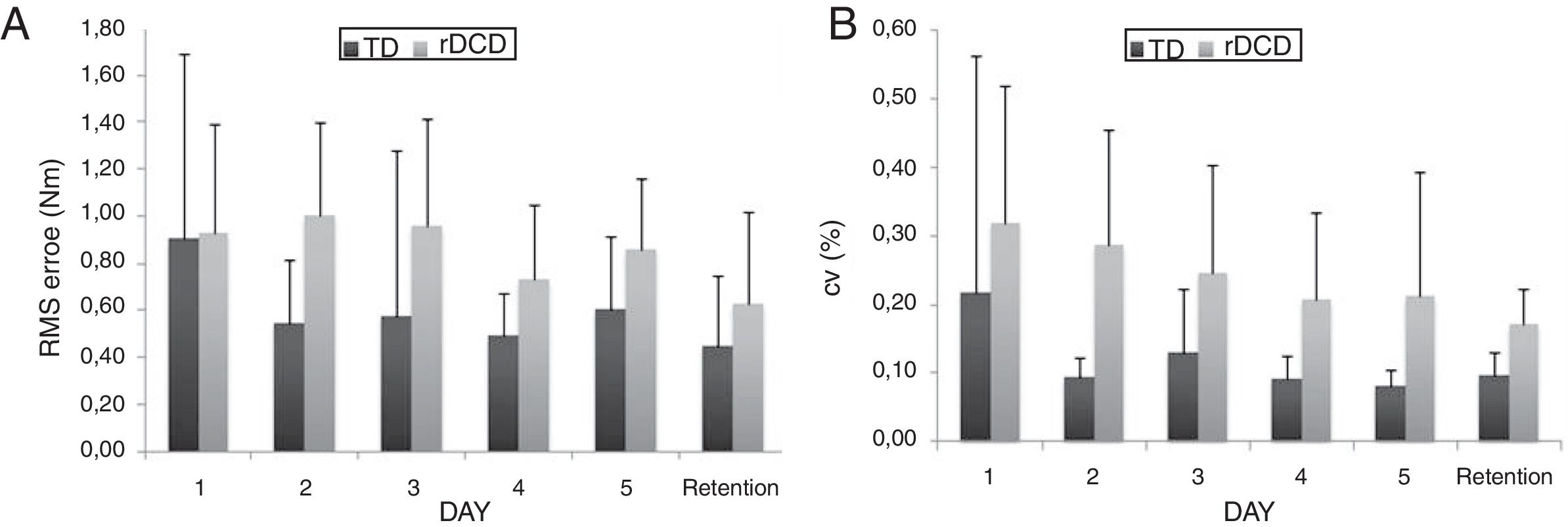
RMSE. The results indicated significant Group and Day effects (both p<0.05). The rDCD group (0.85Nm) was significantly less accurate than TD group (0.59Nm). However, both groups displayed similar performances only on Day 1 (Fig. 3A). On Day 2, 3, 4, 5, and in the retention phase, TD children were more accurate to perform the task than children at rDCD.
 and coefficient of variation (B) across five days of practice and retention phase for children at risk of development coordination disorder and typically developing children.")
CV. The results revealed significant Group (p<0.01) and Day effects (p<0.05). Overall, across five days and retention phase the rDCD group (0.24Nm) displayed higher CV than the TD group (0.11Nm). Post hoc tests revealed that rDCD and TD groups showed lower CV on Day 4, 5 and retention phase compared to Day 1. Fig. 3B shows the difference between groups, as well as a tendency for both groups to reduce variability of the force/torque fingers isometric contraction across five days and retention phase.
DiscussionEffect of practice on force/torque controlIn agreement to previous researchs,1,23 children at rDCD were able to produce similar level of MVT as their TD peers. This result is frequently explained due to their increased levels of co-activation, programming problems, lack of movement experience and difference in muscle-fiber distribution.11,24 Muscular strength does not appear to be the problem for these children, but the ability to control required force from a set of muscles and joints involved in the task.1,9 The results on Day 1, which served as a baseline for comparison between groups, are congruent with previous research in which children with DCD showed lower accuracy as well as higher variability to maintain the required level of force/torque compared to TD children in a similar task used in the present study1 and in an index finger pressing task.23
There is evidence that difficulties in generating a precise control of manual force by children with DCD may be associated with neuromuscular timing.12,25 Specifically, the lack of coordination in the temporal relationship between agonist and antagonistic muscles reflects on force production and control. Previous studies11,26 showed that children with DCD extend the activity of agonist muscle and delay the activity of antagonist muscle, leaving to difficulty in performs fast and accurate actions. Recently, Fuelscher et al.27 showed, in a meta-analysis, that children with DCD presented reduced neural activation in five anatomical loci, including cerebellum, during manipulative tasks. It has been suggested that there is an influence of the reduced cerebellar activation on DCD, given that cerebellum has an important whole in the sequence, force and timing of muscle (agonist/antagonist) contractions during performance of postural and motor actions.
Assuming that the isometric force/torque control in children with DCD is less accurate and more variable than that of TD children, the main interest issue of this study was to examine whether practice of the isometric force/torque task performed by children at rDCD would alter variables such as accuracy and variability. If practice alters these variables, then training is an essential source to provide opportunities of improvement to these children.
The results of the present study support the hypothesis that practice improves the force/torque control in children at rDCD. Fig. 2 indicated that children at rDCD did reduce variability and enhance accuracy to a similar level as TD children did, specifically the improvement occurred from Day 3–5 and on retention. It has previously been shown that younger children needed more practice trials to reach a criterion level for isometric force modification when compared to older children.3 The ability to better control and adjust a constant force might be a skill that takes several years3,4 giving older children and adults with small advantage to successful perform the task on the first attempts. If the motor problems of children at rDCD are associated with a delay in the course of motor development,9 then the practice or intervention could make children at rDCD perform at the same level of TD children. Further practice sessions across days or months are needed to examine whether the effective force/torque modulation shown by children at rDCD is a consistent alteration in the control of fine motor adjustments. The evidence shown in the present study that children at rDCD are capable of improving the performance with practice supports the view that motor difficulties imposed on fine force control might not be a chronic disorder and can, in part, be improved through practice.
According to the literature, the reduced error and variability of force/torque production after practice may generally be attributed to neural adaptation18 and/or motor learning.28 The co-contraction of agonist and antagonist muscles during a motor task could be associated with little experience in a new movement,11 such one of the present study. The more experienced the child becomes in the motor task requested, the better your temporal coordination relationship among the muscles involved in the action becomes and, thus, better is its performance.
Force/torque control without visual feedbackThere are evidences that children with DCD are sensitive to poor performance when visual information is removed.15,16 Fuelscher et al.27 showed that children with DCD have greater activation in parts of the thalamus, reflecting a reduced ability to integrate predictive sensory information with the unfolding motor command, and, as consequence, a greater dependence on visual feedback during tasks of finger and manual motor control.27 Other studies suggest that despite the fact that children with DCD do not show increased dependency of visual feedback, but poor recognition of the demands of the task, they also show minor adaptation when feedback is removed.17 In the present study, performance of children at rDCD was lower than TD children after the removal of visual feedback and confirms the hypothesis that children at rDCD need visual information for the control on the production of force/torque, even after practicing the task. Grip force/torque increased during the task without visual feedback was observed in children at rDCD and may thus be considered a strategic response to sensory loss that counteracts unexpected perturbations as example when the information about the target is not present. This selective dependence on visual information can be associated with deficits in other sensory modalities.29 Movements generated in the absence of visual feedback have a greater reliance on memory, especially of cutaneous and proprioceptive feedback information.20,30
The control of force/torque production during manipulative tasks may result from internal model built by means of the visual and haptic information about the propriety of the objects and position of the body that influence the neuromuscular adjust for actions. The muscle and joint receptors could provide the necessary sensory feedback to update the relevant internal models used to predict sensory events and estimate the grip force output in anticipation of the movement.30 In the present study, TD children seemed to execute the trials without visual feedback with basis in an internal representation, construed by means of the adjustment acquired in the practice phase, when the visual feedback was provided, what do not happen with children at rDCD. These children seemed to use visual information to strength of mechanics of detection and correction of errors to adjust task demands only in the practice phase. This suggests that children at rDCD may have difficulties in perceiving or using other sensory channels, as cutaneous and proprioceptive, to construct internal representation of task demands during practice phase to compensate the lack of visual information.
The results give support to the hypothesis that children at rDCD are capable of learning to reorganize their sensorimotor output in an effective way as TD children do. However, it is suggested that they need more time to adjust to task demands when visual feedback is removed. In general, it was expected that repeated practice was one of the intervention strategies to minimize some motor problems faced by these children. One of the limitations of the present study was the time and the type of practice. If there were more practice sessions, maybe children at rDCD could construct and use an internal representation of the movement required for the task when visual feedback was removed. Other limitation of the present study refers to sample characterization as well as the sample size. However, the selection of participants was reasonably controlled so that no children were included with any known diagnosis or school difficulties sufficient for special care. Also, no kind of blinding of assessors was applied in any phase of this study. Whether this is an influence on the effects of torque/force production results is a matter of investigation.
ConclusionChildren at rDCD showed a significant improvement in force/torque modulation with practice and they seem to have reached their limits that were close to the performance of TD children. However, they are more dependent of the available information in feedback than TD children are. Thus, visual feedback was an important component in the process of control and production of force of children at rDCD mainly in the strength of the mechanisms of detention and correction of errors for the necessary adjustments to the demands of the task. Finally, the practice is one of the forms of give chance for better motor development of children with DCD and can be considered as strategies of intervention for force production and control.
Conflicts of interestThe authors declare no conflicts of interest.
We thank to Dario Donatti (UNESP/Rio Claro) for the availability of the oscilloscope and to Robson Pederiva and members of the Office of Mechanical Projects (Oficina de Projetos Mecânicos – UNICAMP/Campinas) for their collaborations in the calibration process of the equipment used in the present study.



